
ABSTRACT
The world has seen many problems with man-made chemicals such as thalidomide, PCB’s, DDT etc. In many people, this has sparked a fear of all chemicals, including many that are naturally occurring. Members of the scientific community are not immune to these fears. Formaldehyde in dentistry is a classic example of the irrational fear, in the scientific community, of a substance that is present in every cell in the human body. There is significant controversy among formaldehyde researchers about the connection of formaldehyde to cancer in humans but one common theme seen in their research is that formaldehyde is a concern only in high concentrations. A review of the literature and a knowledge-based approach should allay the fear of the use of this substance in quantities that are used in dentistry. Formaldehyde is an essential part of human cellular function. The dental community should be reminded that the investigation of naturally occurring substances, with which we have evolved over thousands of years, is very different than that of man-made chemicals. It is also essential to remember that any discussion on the toxicity of a substance must be related to dosage.
Introduction
There is significant anxiety concerning the use of formaldehyde (CHHO) in dentistry. The carcinogenicity and cytotoxicity of CHHO is always noted in the dental literature as a significant problem. The Royal College of Dental Surgeons of Ontario proclaimed in 1996 that the use of paraformaldehyde containing endodontic filling materials constituted professional misconduct. This was proclaimed in the RCDSO magazine Dispatch1 with no scientific references, although the article did refer to the “extensive scientific research into the biological effects of paraformaldehyde containing endodontic filling materials”. Yet a search of the literature mainly reveals case reports of injury from overfills into the mandibular nerve canal. There have been reports of problems with overfills using many endodontic filling materials, including gutta percha extruded into the maxillary sinus.2 To claim that these overfills make CHHO unsafe in dentistry is an improper use of case reports.
Formaldehyde – The Ubiquitous Substance
CHHO is a naturally occurring substance but is often used in a manmade way. It is in our food chain and is a natural product of cell metabolism but it is also a product of automobile and truck combustion, cooking of our food, the fixing of tissue in research and pathology laboratories, the embalming of the dead and the production of a wide array of products from particle core wood products to carpets, wood cabinets and resins Workers in these fields are exposed to significant levels of CHHO every working day. Policy makers do have some concerns and have a tendency to err on the side of caution because of the number of people worldwide that work in environments with very high levels of CHHO. However, they also recognize that CHHO is ubiquitous and that low levels are not a concern.
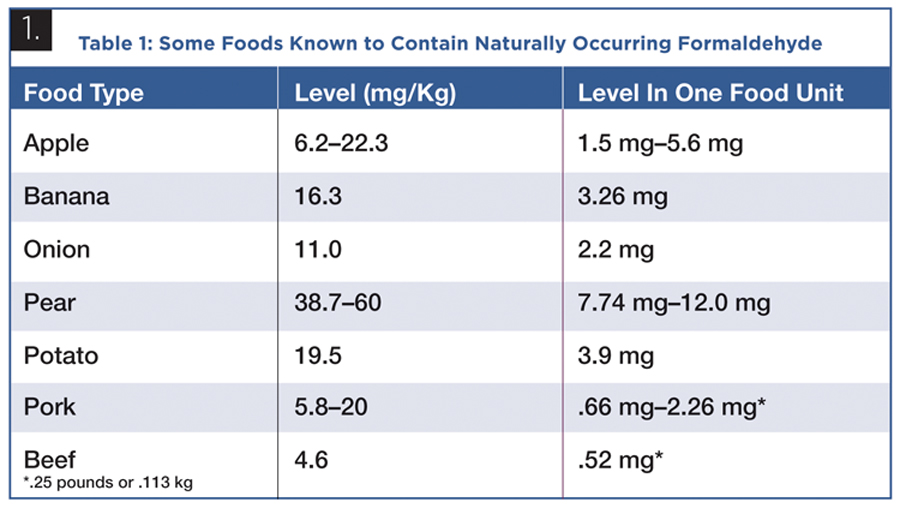
Table 1 lists common foods and their formaldehyde levels. The amount for one unit of each food (a single fruit or single vegetable) is calculated using figures provided by the Centre For Food Safety, Government of Hong Kong.3 The simple concept that low levels of CHHO cause problems for humans is difficult to reconciled with its prevalence in nature.
TABLE 1. Some Foods Known to Contain Naturally Occurring Formaldehyde
Formaldehyde and Cancer
The study of CHHO’s effects on humans has an experimental advantage in that it is not only ubiquitous, but is used in many environments where workers are exposed to unnaturally high levels of the substance. From pathologists to morticians to chemical plant workers, it stands to reason that these populations, like those that use tobacco, would have a dose response curve between inhalation of CHHO and cancer. The literature does not bear that out. The study of CHHO as a human carcinogen is an area that, today, sparks significant controversy among those that do the research.
The first report of CHHO causing nasopharyngeal cancers in rats appeared in the literature in 1980. Swenberg et al4 reported on carcinomas appearing in rats exposed to 15 ppm CHHO daily for 18 months. Carcinomas were not found in rats exposed to 2 or 6 ppm of formaldehyde.
This study and one by Kerns et al5 stimulated considerable research on the effects of CHHO on workers with significant exposure. Hauptmann et al6 produced the research that was pivotal in the classification of CHHO as a possible carcinogen among exposed workers. The assumption was that there would be an increase in the occurrence of nasopharyngeal carcinomas as a result of the observations in rats. In 10 workplaces studied there was a significant number of nasopharyngeal cancers in only one plant. The data from that plant was dismissed as invalid7 because many of the workers were involved in metal treatment with acid mists and other toxins in the air. The other nine plants showed a rate of nasopharyngeal cancer that was actually lower than the rate in the general population.
Hauptmann et al8 then implicated CHHO exposure in morticians with a higher rate of leukaemia. Casanova et al9 demonstrated that exposure of rhesus monkeys to CHHO by inhalation did not change its blood level, which supports the generally accepted fact that it is quickly absorbed and metabolized at the point of contact. The link between CHHO and leukaemia became tenuous. Furthermore, Frank,10 using mathematical modeling, concluded that it was unlikely that exogenous CHHO could reach distant sites and it would therefore be difficult to implicated it as a cause for leukaemia in humans.
It is notable that a 2013 article by Swenberg et al11 refers to the fact that in 30 years of research, after Swenberg’s group reported on CHHO’s carcinogenic effects in rats,4 the method of action for carcinogenicity has not been determined and the article places doubt on current cancer risk assessments for humans.
The controversy surrounding the carcinogenicity of CHHO can be seen in the results of the WHO’s International Agency for Research on Cancer (IARC) monograph on CHHO published in 2012.12 In the conclusion of the monograph it states that a small majority of reviewers found sufficient evidence that CHHO causes leukaemia. A minority did not agree and found the evidence insufficient. They did, however, classify CHHO as a known human carcinogen. The controversy grows even more when one examines the report of the Second International Formaldehyde Science Conference13 held in Madrid in 2012 after the release of the IARC position paper. The pre-eminent researchers in the field highlighted some of the discrepancies in the research but, notably, Swenberg reported that, whereas endogenous CHHO adducts are found in all cells and tissues, the exogenous CHHO adducts in nasal epithelium found after exposure to it were not found in the bone marrow. He concluded that the plausibility of CHHO inducing leukaemia could not be supported. The research continues and the controversy continues but, in the meantime, people refer to CHHO as a carcinogen without qualifying the statement with “in high concentrations”.
Formaldehyde in Dentistry
There is significant concern regarding the use of formocresol for primary tooth pulpotomies. In this technique a primary tooth with a large carious lesion, which demonstrates symptoms of pulpitis, has the tissue removed from the pulp chamber leaving the radicular tissue intact. These “nerve stumps” are then directly treated for five minutes with formocresol on a cotton pellet. A popular product for this technique is Buckley’s formocresol which, at full strength, is made up of 19% CHHO, 35% cresol, 17.5% glycerine and water.
Formocresol pulpotomy was a topic prominently discussed at a joint meeting of the American Academy of Paediatric Dentistry and the American Association of Endodontists held in 2007.14 The title was “Emerging Science in Pulp Therapy: New Insights into Dilemmas and Controversies”. Formocresol and hence CHHO was the source of much of the controversy. Casas et al15 referred to CHHO’s “mutagenicity, carcinogenicity and immune sensitization” in their suggestion that formocresol may no longer be appropriate in primary tooth pulpotomies. Milnes16 undertook a thorough literature review of the toxicity and carcinogenicity of CHHO in his defence of formocresol pulpotomies and calculated that if all the formocresol in the cotton pellet used to apply it to vital pulp tissue were absorbed, a child would be exposed to .1 mg of formocresol. Assuming that the solution contained 19% CHHO, the exposure would be .02 mg of CHHO. This is well below any level of concern especially when a child would ingest 75 to 280 times that amount by consuming an apple.
In 2003 Boj et al17 injected, into the veins of rats, the equivalent dose of CHHO as a child would receive after 100 pulpotomies. They found no evidence of nephrotoxicity. This was followed in 2007 by an experiment by Cortes et al18 in which rats were again infused with the same high dose to determine if any damage would be seen in the liver. No signs of hepatotoxicity were found.
In 2008 Kahl et al19 reported rather convincing research on the safety of formocresol pulpotomies. They collected venous blood samples from thirty children ranging from two to six years old who had formocresol pulpotomy treatment under general anesthetic. They found no change in the blood level of CHHO in any of the patients, above the pre-surgical baseline level, during and after the procedures. They concluded that, “It is unlikely that formocresol, when used in the doses typically employed for a vital pulpotomy procedure, poses any risk to children”. This study would seem to confirm that CHHO is quickly metabolized at the site of contact.
The greater controversy in dentistry is on the subject of the use of CHHO containing compounds in the endodontic treatment of permanent teeth. This is a highly political controversy and it is not the purpose of this review to endorse or analyze any particular methodology for endodontic treatment. This review attempts to make the point that the CHHO used in these endodontic treatments, as with formocresol in pulpotomies, is not a legitimate concern for dentists. In fact AH 26 is a sealer that is promoted and distributed by a prominent dental supplier in the U.S. as a resin based sealer that is touted to be eugenol free. Athanassiadis et al20 devoted an entire paper to the safety of the CHHO released by AH26 because as a resin it does, in fact, also release it but it has somehow escaped this CHHO controversy.
The chemical most often used in “controversial” endodontics is paraformaldehyde. CHHO is a gas and paraformaldehyde is produced by making an aqueous solution of CHHO and then removing all the water. The resultant powder is 90 to 95% CHHO. The two most popular products used in endodontics which contain CHHO are Sargenti N2 paste and Endomethasone-N. The major difference with Endomethasone is the addition of corticosteroid. This is apparently done to counteract possible post endodontic pain resulting from inflammation. The powder in these products contains five to six percent paraformaldehyde and is combined with eugenol to form a paste that can be carried into the debrided root canal space with a lentula spiral. The canal can be completely filled with this paste as it has barium sulphate added for radiopacity, or a size matched single gutta percha cone is used so that the paste takes the place of other types of sealers. The quantity of CHHO that is placed in the canal depends on whether the material is used as an endodontic filler or a sealer. The concern expressed regarding these products is the claimed harmful effects of paraformaldehyde which releases the CHHO into the tooth and the periapical tissues.
The difficulty in accepting this concern regarding the harmful effects of such small amounts of CHHO is rooted in the fact that in the volumes of literature by experts in the field of CHHO there is no concern about it in small amounts. The research being conducted currently is focused on high exposure over long periods of time, i.e. CHHO exposed workers. Limited exposure is not of concern to the CHHO experts.
As an analogy to the release of CHHO in endodontic treatment one can examine the paper by Dhareshwar and Valentino21 in which they tackled the problem of prodrugs that release CHHO during biotransformation. They conclude that, “Considering the normal formaldehyde levels in humans (2-3 gm/kg) it seems unlikely that formaldehyde from a prodrug will adversely effect normal physiological functions within the human body”. The oral prodrugs that they discuss release from 1.2-50.5 mg of CHHO per dose. This is far more than a canal fully filled with N2 paste.
Venuti22 has calculated the amount of CHHO that would be applied to an average root canal space utilizing Sargenti N2 paste. In a case of complete fill with the paste, the amount is calculated to be .4-.8 mg and, in the case of a single cone gutta percha point used to fill the space, the amount would be .04-.08 mg. These amounts are negligible in the context of the amount that the body is continuously metabolizing and the amounts released by prodrugs.
There have been claims made that paraformaldehyde containing pastes are cytotoxic. Yet studies have shown cytotoxicity caused by sealers that are in regular use today which do not incorporate paraformaldehyde.23,24 The historical literature has also shown the cytotoxicity of eugenol. Vidya et al25 conducted an interesting histological study implanting polyethylene tubes in the soft tissue and bone of rats. The tubes contained N2 paste, Endomethasone and zinc oxide-eugenol respectively with empty tubes as controls. The lumen of the tubes were made to match those of the apical foramina of human teeth. The soft tissue responses were interesting in their similarities after six weeks, but the significant findings were noted when the bone was examined, as this would be most representative of these sealers in completed endodontic cases. They found the smallest reactive area of bone around the N2 but these areas had evidence of necrotic bone. By the end of four weeks the necrotic bone had resolved and there was considerable new bone with normal marrow in the adjacent bone. A reparative bone response was found with all three materials after six weeks. A search of the literature on the subject of the histopathology of dental sealers only revealed a few, more current studies but they were not as sophisticated as the Vidya et al study as they simply injected the materials directly into rat connective tissue.
Another major complaint regarding the use of paraformaldehyde in endodontic treatment is the nerve damage and paresthesia caused by the overfill of these materials into the mandibular canal. Of course, case reports are of limited use and there are cases in the literature that deal with these types of overfills with AH26, softened gutta percha, calcium hydroxide, Endomethasone, zinc oxide-eugenol as well as N2. Gluskin references the literature on these overfills in his thorough review of complications in obturation.26 Blanas et al27 described a case of nerve damage from an overfill of softened gutta percha. They pointed out the obvious when they cautioned, “…practitioners must take care to ensure proper technique during both instrumentation and obturation”. It confuses the subject of the safety of CHHO in endodontics by referring to cases of poor endodontic technique.
The use of a paraformaldehyde endodontic paste in dentistry has become a political issue and has pitted the American Endodontic Society (users of N2) against the American Association of Endodontists (the endodontic specialists). Again, this has served only to get in the way of a rational examination of the science of CHHO because it has injected conditional bias into the science of endodontics.
Dunbar28 explains how a significant amount of research has shown that scientists have a variety of biases and that “people ignore much relevant information when evaluating whether a potential cause really is relevant”. If one enters a search phrase online, “anaphylactic reaction to formaldehyde in endodontics”, there are actually articles asserting that this occurs. If one keeps in mind that exogenous formaldehyde is the same chemical as endogenous formaldehyde and we have a natural level of 2-3 gm per kg in our bodies, an anaphylactic reaction to formaldehyde is physiologically impossible. This is comparable to proclaiming that people can have anaphylactic reactions to epinephrine. Conditional bias against CHHO must be the reason that these conclusions are made.
Conclusion
Irrational fear is related to a distorted sense of risk and can range from mild discomfort to crippling phobia. The essential ingredient in the fear of a substance is forgetting that toxicity is related to dosage. Every toxicologist knows that every material that can be ingested or inhaled, including water, has toxic effects at certain threshold doses. Yet, members of the scientific community often forget this essential point. The most research done on the effects of very small amounts of CHHO is primarily found in the dental literature. There it is forgotten that this chemical, that is claimed to be harmful, is endogenous and in a greater quantity than the exogenous amount that the researchers are examining.
The use of the internet is also a prime example of irrational fear. Websites are set up, the subject is sensationalized and like minded followers are recruited. The science is distorted so that if one enters a search word, negative websites appear. If the reader thinks that this refers only to “anti-fluoridationists” and “anti-vacciners” one only has to type Sargenti N2 as a search term online to see the same thing in the dental profession.
As dentistry moves to become more of a knowledge based profession it is time to accept what the experts on CHHO already know. Low levels of this substance are not harmful. It is irrational to fear CHHO at the minuscule levels used in dentistry. Endodontics and vital pulpotomy have very high success rates and one can only imagine how many millions of teeth have been saved, yet almost every material used in these treatments has some cytotoxicity. Could it be that the materials, used in such minute amounts, are not critically important? Perhaps the most important thing that the research shows is that excellent technique is key to successful treatment.OH
Dr. Pasquale Duronio is a general dentist in private practice in Lion’s Head, Ontario. He completed his DDS at Western University in 1976.
Oral Health welcomes this original article.
Acknowledgement:
The author wishes to thank Peng Zhang, a PhD candidate in the Experimental Medicine program at the University of British Columbia, for some formocresol calculations. His information was one of the factors that motivated the author to go ahead with this literature review.
The author reports no conflicts of interest nor has he received any financial support from any source in the preparation of this literature review. He can be reached at patduronio@amtelecom.net.
Oral Health welcomes this original article.
References:
1. Royal College of Dental Surgeons of Ontario. Use of paraformaldehyde materials in endodontic treatment unacceptable. Dispatch April 1996.
2. Hodnett B L, Ferguson B. Case report: retained gutta-percha as a cause for persistent maxillary sinusitis and pain. Published online 2014. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3999928.1/
3. Centre for Food Safety, Government of Hong Kong. www.cfs.gov.hk/english/whatsnew/whatsnew_fa/files/formaldehyde.pdf
4. Swenberg JA, Kerns WD, Mitchell RI, Gralla EJ, Pavkov KL. Induction of squamous cell carcinomas of the rat nasal cavity by inhalation exposure to formaldehyde vapor. J Cancer Res 1980. 40: 3398-402. http://cancerres.aacrjournals.org/content/40/9/3398.abstract
5. Kerns WD, Pavkov KL, Donofrio DJ, Gralla EJ, Swenberg JA. Carcinogenicity of formaldehyde in rats and mice after long term inhalation exposure. J Cancer Res 1983. 43: 4382-92. www.ncbi.nlm.nih.gov/pubmed/6871871
6. Hauptmann M, Lubin JH, Stewart PA, Hayes RB, Blair A. Mortality from solid cancers among workers in formaldehyde industries. Am J Epidemiol 2004. 159: 1117-30. www.ncbi.nlm.nih.gov/pubmed/15191929
7. Marsh GM, Youk AO, Buchanic JM, Erdal S, Esmen NA. Work in the metal industry and nasopharyngeal cancer mortality among formaldehyde exposed workers. Regul Toxicol Pharmacol 2007. 48: 308-19. www.ncbi.nlm.nih.gov/pubmed/17544557
8. Hauptmann M, Stewart PA, Lubin JH, Beane Freeman LE, Hornung RW, Herrick RF, Hoover RN, Fraumeni JF, Blair A, Hayes RB. Mortality from lymphohematopoietic malignancies and brain cancer among embalmers exposed to formaldehyde. J Nat Cancer Inst 2009. 101: 1696–708. www.ncbi.nlm.nih.gov/pubmed/14600094
9. Casanova M, Heck H d’A, Everitt J I, Harrington Jr W W, Popp J A. Formaldehyde concentrations in the blood of rhesus monkeys after inhalation exposure. Food Chem Tox 1988. 26(8): 715-16. www.ncbi.nlm.nih.gov/pubmed/3198038
10. Frank S J. A mathematical model for the absorption and metabolism of formaldehyde vapour by humans. Tox Appl Pharmacol 2005. 206(3): 309-20. http://gel.berkeley.edu/formaldehyde/FranksSJ_2005.pdf
11. Swenberg, J A, Moeller B C, Lu K, Rager J E, Fry R C, Starr T B. Formaldehyde Carcinogenicity Research: 30 Years and Counting for Mode of Action, Epidemiology, and Cancer Risk Assessment. Toxicologic Pathol 2013. 41 (2): 181-9. www.ncbi.nlm.nih.gov/pubmed/23160431
12. International Agency for Research on Cancer. Formaldehyde monograph. 2012. http://monographs.iarc.fr/ENG/Monographs/vol100F/mono100F-29.pdf
13. Bolt B M, Morfeld P. New results on formaldehyde: the 2nd International Science Conference (Madrid, 19-20 April 2012). http://link.springer.com/article/10.1007/s00204-012-0966-4/fulltext.html
14. Pulp Symposium. J Endo 2008; 34(7S). www.aae.org/managedfiles/pub/0/pulp/joejulysupplement.pdf
15. Casas MJ, Kenney DJ, Judd PL, Johnston DH. Do we still need formocresol in pediatric dentistry? J Can Dent Assoc 2005; 71(10):749-51. www.cda-adc.ca/jcda/vol-71/issue-10/749.pdf
16. Milnes A R. Persuasive evidence that formocresol use in pediatric dentistry is safe. J Can Dent Assoc 2006. 72(3): 247-54. www.cda-adc.ca/jcda/vol-72/issue-3/247.pdf
17. oj J R, Marco I, Cortes O, Canalda C. The acute nephrotoxicity of systemically administered formaldehyde in rats. Eur J Pediatr Dent. 2003; 4(1):16-20. www.ncbi.nlm.nih.gov/pubmed/12870983
18. Cortes O, Fernandez J, Boj J R, Canalda C. Effect of formaldehyde on rat liver in doses used in pulpotomies. J Clin Pediatr Dent. 2007; 31(3):181-4. www.ncbi.nlm.nih.gov/pubmed/17550043
19. Kahl J, Easton J, Johnson G, Zuk J, Wilson S, Galinkin J. Formocresol blood levels in children receiving dental treatment under general anesthesia. Pediatr Dent. 2008; 30(5):393-9. www.ncbi.nlm.nih.gov/pubmed/18942598
20. Athanassiadis B, George GA, Abbott PV, Wash L J. A review of the effects of formaldehyde release from endodontic materials. Int Endo J. 2014; 10(1). Online purchase with no page numbers. http://onlinelibrary.wiley.com/doi/10.1111/iej.12389/abstract
21. Dhareshwar S S, Valentino J S. Your prodrug releases formaldehyde: Should you be concerned? No! J Pharm Sci. 2008; 97(10):4184-93. www.ncbi.nlm.nih.gov/pubmed/18288723
22. Venuti Studio Dentistico. http://www.studiodentisticovenuti.it/2012/12/10/n2-and-sargenti/
23. Lodiene G, Morisbak E, Bruzell E, Orstavik D. Toxicity evaluation of root canal sealers in vitro. Int Endo J. 2008; 41(1):72-77. www.ncbi.nlm.nih.gov/pubmed/17931390
24. Karapinar-Kazandag M, Bayrak O F, Yalvac M E, Ersev H, Tanalp J, Sahin F, Bayirli G. Cytotoxicity of 5 endodontic sealers on L929 cell line and human dental pulp cells. Int Endo J. 2011; 44(7):626-34. www.ncbi.nlm.nih.gov/pubmed/21306404
25. Vidya S, Parameswaran A, Sugumaran VG. Comparative evaluation of tissue compatibility of three root canal sealants in Rattus Norwegicus: A histopathological study. Edodontology. 1994; 6(2):7-17. http://medind.nic.in/eaa/t94/i2/eaat94i2p7.pdf
26. Gluskin A H. Mishaps and serious complications in endodontic obturation. Endodontic Topics. 2006; 12(1):52-70. http://onlinelibrary.wiley.com/doi/10.1111/j.1601-1546.2005.00194.x/abstract
27. Blanas N, Kienle F, Sandor G K B. Inferior alveolar nerve injury caused by thermoplastic gutta-percha overextension. J Can Dent Assoc. 2004; 70(6):384-7. http://cda-adc.ca/jadc/vol-70/issue-6/384.pdf
28. Dunbar K. Page 130, Chapter 5–What scientific thinking reveals about the nature of cognition. From Ward, Smith and Vaid: Conceptual Structures and Processes: Emergence, Discovery and Change. 1997. Washington D.C., American Psychological Association Press. www.utsc.utoronto.ca/~dunbarlab/pubpdfs/dunbar-desSci.pdf











