
Digital radiography can improve our ability as clinicians to treat patients effectively, quickly and in a manner that leads to treatment allowing for less pain and recall. This article describes digital radiography techniques, which help with diagnosis for all aspects of dentistry and implant treatment planning. It describes procedures, which merge the use of CEREC, from Sirona Dental Systems, with ConeBeam (or dental CT).
Diagnostic Assistance
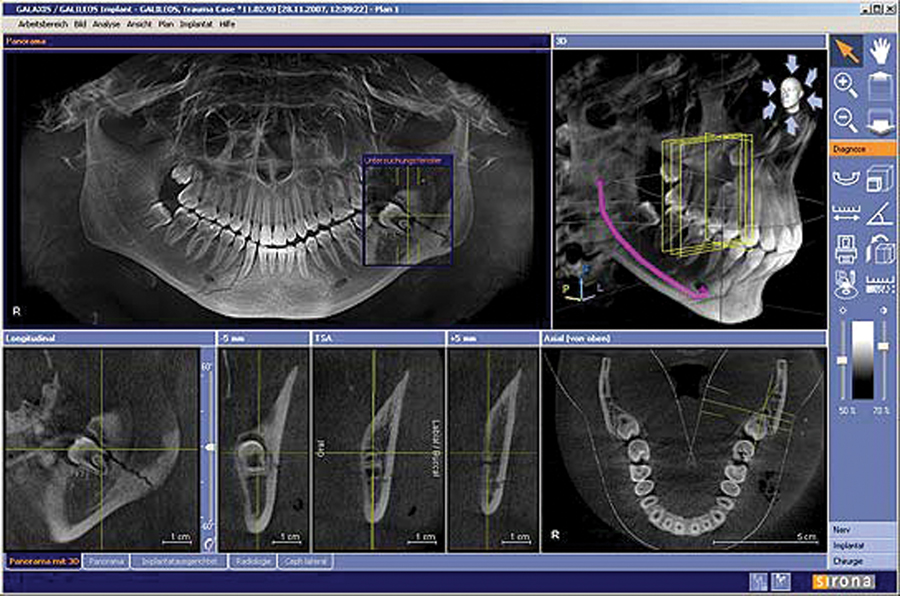
A dental CT allows for diagnosis of endodontic lesions, pathology, nerve localization prior to surgery, periodontal disease conditions, airway assessment and the assessment of bone volume prior to implant surgery (Figs. 1 & 2).
Figures 1 and 2 demonstrate how a dental CT helps the clinician localize pathology or aid in diagnosis. The three dimensional view allows us to visualize a diagnosis via slices of the area of interest, while the traditional two dimensional view makes it difficult, to impossible, at times to see the same pathology. The visualization is also more rapid, immediate and intuitive because the third image is more closely aligned to how we actually see the patient.
FIGURE 1.

FIGURE 2.
Implantology
The three dimensional capability also assists with implantology. Here, careful prosthetic planning is a must in the treatment plan for prosthetic success.
• We can take an optical impression (Fig. 3) of the patient’s mouth with CEREC and decide where the new tooth should be positioned.
• We would then propose on the optical impression the soon to be replaced tooth with the CEREC software (Fig. 3a). In this fashion, we will have the opportunity to ideally place the implant via guided implant surgery.
• For guided surgery, one would merge the optical impression taken with a CEREC to Sirona’s XG3D ConeBeam or Galileos.
• Once the files have been merged, one can analyze the ConeBeam volume and place the implant in the ideal position for the tooth to be replaced (Fig. 4).
FIGURE 3.

FIGURE 3A.
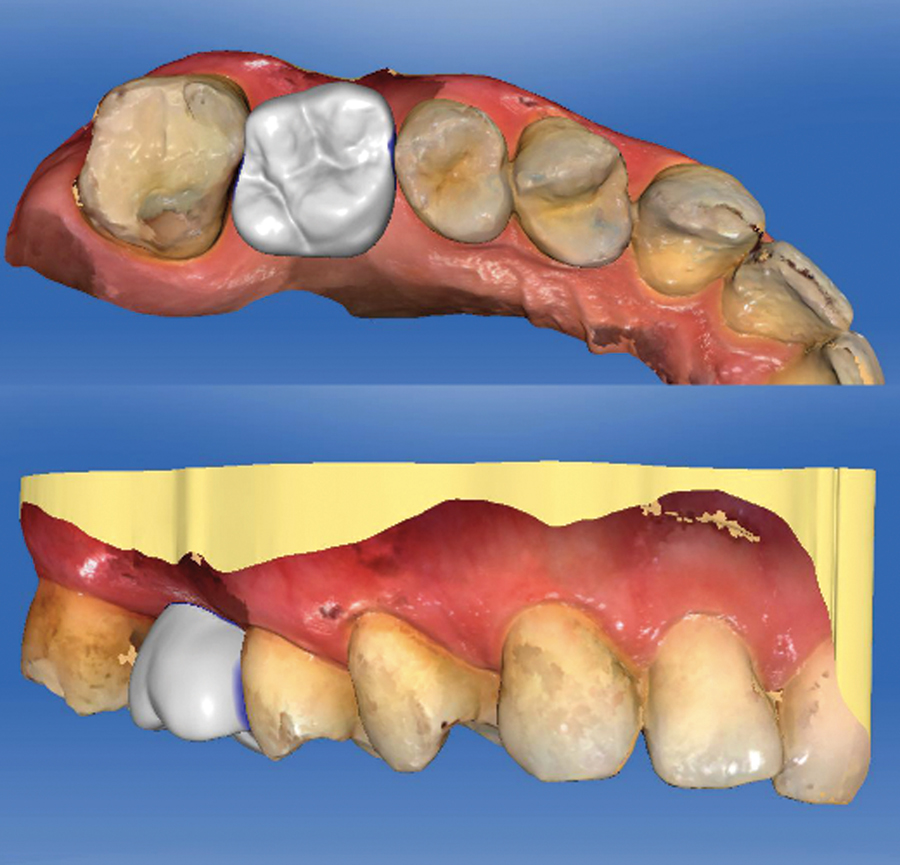
FIGURE 4.

Placing the Implant Effectively – The Surgical Guide
Ideally placing the implant allows for the ideal distribution of force factors. At this time, one will be able to properly assess if there is a sufficient amount of bone for implant success and a decision can be made to proceed forward with implant placement or consider bone augmentation procedures.
The next step in treatment is to fabricate a surgical guide. A surgical guide allows for the placement of a dental implant in the precise location that was planned on the ConeBeam volume.
With guided surgery, surgical guide keys are placed in the surgical guide to allow for the creation of sequential osteotomies. In addition, a surgical guide allows for, when indicated, a flapless procedure. Utilizing a tissue punch, the implant would be placed in the predetermined position with confidence that one would not be inadvertently placing the implant in the incorrect location and not inadvertently perforating the sinus, touching an adjacent root or the inferior alveolar nerve. This approach is beneficial to the patient, as they would have reduced risk for post surgery complications such as bleeding and pain. This process also leads to increased implant success.
The surgical guide (Fig. 5) can be fabricated in one of two fashions. The first method is to digitally send the ConeBeam volume and optical impression to SiCAT. Alternatively, if one does not have an optical impression, a stone model would be sent to SiCAT. SiCAT would create a surgical guide to place implants from one implant to an entire arch.
The second method for the fabrication is the in-office CEREC solution. One would merge the ConeBeam volume with the optical impression taken with the CEREC system. A surgical guide can then be milled in the office on the CEREC milling system to place the dental implants.
FIGURE 5.

Once the dental implant is placed, a custom-healing abutment can be fabricated with the CEREC system to create the proper gingival architecture. The CEREC system would be utilized to take an optical impression of the dental implant, adjacent teeth and the gingiva. The custom healing abutment could then be fabricated utilizing a TiBASE and a material that can be milled on the CEREC milling chamber such as e.MAX, Telio CAD or Enamic.
After the dental implant has fully integrated, the digital patient is now ready for their final prosthetic tooth. The implant, the adjacent teeth and the gingiva would be imaged with the CEREC as a digital optical impression (Fig. 6). Digitally on the CEREC, a custom abutment with the final crown could be proposed (Fig. 7). Once the digital tooth has been designed, it can be milled in the office utilizing a material from Ivoclar Vivadent called e.MAX. Alternatively, one could create a screw retained hybrid crown that attaches to the implant. This method allows for the insertion of the final prosthesis without the use of dental cements. Figure 8 illustrates an uncrystallized e.MAX abutment and hybrid crown. In Figure 9, the same e.MAX abutment and hybrid crown have been crystallized with staining and glazing. By utilizing e.MAX as a restorative material, beautiful restorations can be created that blend seamlessly in the oral cavity (Fig. 10).
FIGURE 6.
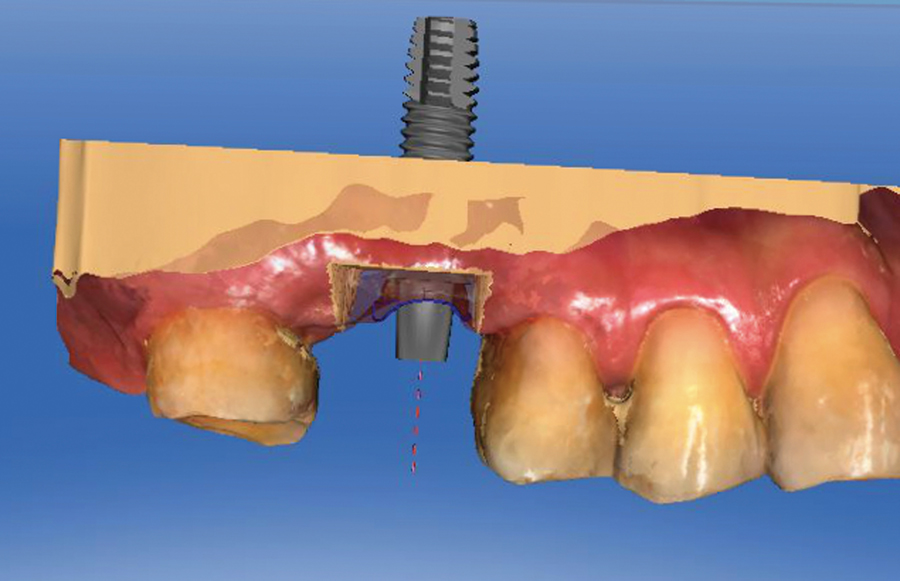
FIGURE 7.

FIGURE 8.

FIGURE 9.

FIGURE 10.

In this workflow, a patient can be fully diagnosed, treatment planned and treated digitally. The CEREC-ConeBeam integration allows for better diagnosis capabilities, more precise treatment planning and a solution for implant placement and prosthetic treatment that harnesses digital dentistry. OH
Dr. Bobby Chagger is a graduate of the University of Toronto and has a strong interest in dental implantology utilizing ConeBeam and CEREC. He has successfully integrated CEREC and ConeBeam into his four ChaggerDental Offices in Southern Ontario, which are situated in the cities of Mississauga, Oakville and Burlington. His passion and insight have brought him international recognition as a speaker and educator.
Oral Health welcomes this original article.











