
Cracked teeth present both diagnostic and restorative challenges to any dentist. A cracked tooth can present with varied signs and symptoms based on the location and extent of the crack, which can be difficult to determine and visualize. Treatment of cracked teeth has been controversial in recent literature. Previously, stainless steel bands were often used as a temporary and diagnostic tool before a full coverage restoration.1 Root Canal Treatment (RCT), followed by a crown is recommended if the pulp becomes irreversibly inflamed.2 One study reported successful treatment with a bonded composite restoration after six months, with no differences between restorations with or without cuspal coverage.3
The prognosis of the relevant tooth depends on the extent of the crack and whether the crack has pierced through enamel, dentin, pulp and/or the chamber floor. Long-term data involving cracked teeth is rare in the literature, which makes clinical decisions more difficult. Additional information regarding cracked teeth would provide a better perspective on the clinical management and outcome of these teeth. Cracks that communicate with the pulpal floor or beyond alveolar bone have been deemed hopeless.4 The purpose of this article is to summarize the evidence for survival of cracked teeth, as well as the management to prevent further propagation of cracks.
The 1997 American Association of Endodontists (AAE) article entitled “Cracking the Cracked Tooth Code” defined five different types of tooth cracks.5 Four out of the five types of defects are generated from chewing and biting events. Category one is defined as teeth with craze lines that exhibit no pain, show lines in enamel, but do not block light with transillumination.5 The second category is of teeth with fractured cusps that have mild pain to biting on a specific cusp, usually a marginal ridge and buccal or lingual groove crack in the dentin, which is seen as a shadow with transillumination and a class 2 restoration. Removal of the existing restoration may result in the cusp breaking off. The third category, cracked teeth, may or may not present with a restoration. Cracked teeth are often associated with pain on mastication, brief pain to cold, centrally located mesial to distal marginal ridge cracks seen in the dentin as shadows with transillumination and normal to deep probing depths associated with the crack. One cannot separate the segments of a cracked tooth, and they are often very difficult to diagnose. In the fourth category, being split teeth which can be considered an extension of cracked teeth, there are deep probing depths with both marginal ridges, buccal and lingual cusp separation with an explorer, and have mesiodistal cracks extending across both marginal ridges. Vertical root fractures, the fifth category, stem from radicular structure and extend coronally, which differs from the other four categories. Fractured teeth have often been endodontically treated, contain posts or large restorations, usually have minimal signs/symptoms, may have normal probing depths and can be very difficult to diagnose.5
The ability to properly diagnose cracked teeth is a great asset to a practitioner. Early diagnosis can assist restorative dentists to more appropriately treat cracked teeth before fractures, pulpal involvement and/or periodontal breakdown occurs. The value of early diagnosis to prevent tooth loss will become more important with an aging population. The presenting symptoms of a crack are dependent on the underlying disease process in the dental pulp and peri-radicular tissues that have been caused by the crack.6 The simplest way to consider a crack is that it is a potential cause of pulpal and periodontal problems, similar to caries or poor restoration margins, which can lead to endotoxins entering the pulpal tissue. A crack in a tooth is a clinical finding, not a diagnosis, and should be considered as a potential entry for bacteria into dentinal tubules.7 Not every crack will cause pulpal or periapical disease. Rather, disease is only caused by those cracks where the particular bacteria are virulent enough to cause pulpal disease. To properly investigate the extent of a crack, the removal of all restorations, caries, and associated crack lines is critical.6 Historically, methylene blue, caries indicator dye and transillimunation have all helped with visualization.8 Transillumination is based on the application of physics, where a beam of light will continue to penetrate through a substance until it meets a space, after which the light beam is reflected which results in a light and a dark area separated by the fracture line.9 Using a surgical operating microscope (SOM) is useful so one can turn off the light source and use only magnification with the transilluminator and a dental mirror (Fig. 1). Transillumination is particularly useful when all restorations have been removed. Transillimunation is very popular among clinicians. However, there are two drawbacks if one is not using transillumination under a microscope. Transillumination dramatizes all cracks to the point where craze lines appear as structural cracks and subtle color changes are rendered invisible.9
FIGURE 1. Transillumination under the SOM showing a fractured cusp.

Historically, methylene blue has been used by endodontists during surgery to identify radicular fractures and is now being used to identify coronal cracks. Methlyene blue can be useful in identifying the extent of the crack because of its pooling tendency and flocculent nature.8 However, methylene blue has its downfalls, such as that plaque can stain profusely, and lightly decalcified enamel and dentin absorbs the dye, which can obscure cracks. As well, sodium hypochlorite after prolonged exposure can cause massive absorption of dye by dentin. Therefore, methylene blue should be used immediately after accessing the pulp chamber.8 All posterior teeth that are evaluated with methylene blue should be polished with a rubber cup and coarse pumice slurry. When applied to a desiccated tooth, the methylene blue has the best chance of adhering to the crack.8 Visual inspection using both dies and transillumination remain a critical part of the diagnosis (Fig. 2).
FIGURE 2. Methylene Blue outlining a fracture into a canal.

Traditional cavity designs and materials for incipient lesions are being questioned as to whether they predispose teeth to fracture. Minimally invasive preparation to remove cracks, combined with the flexibility of composite bonded restorations, provide alternative treatment options to traditional designs and materials. The goal of minimally invasive preparations is to avoid connecting individual occlusal or interproximal preparations.6 In 2008, Opdam et al investigated whether a direct composite restoration would be effective for treatment of a painful, cracked tooth.3 Pain corresponded with a more painful response to cold then control teeth, albeit for a short duration. No peri-apical inflammation was noted at the time of examination and treatment. Direct restorations were compared with a cusp covering restoration. Forty of the 41 cases were evaluated at seven years. Three of the forty teeth that were evaluated became irreversibly inflamed and required endodontic treatment during the seven-year period. At seven years, no failures were recorded in the group with cuspal coverage, whereas restorations without cuspal coverage failed at an annual rate of 6%, which was statistically significant.3 Another similar study by Signore et al, in 2007, investigated cracked teeth that were a direct composite restoration followed by an indirect composite onlay with cuspal coverage. This study showed a six-year survival of 93%; the remaining 7% needed endodontic therapy.10 A study by Krell and Rivera in 2007 examined teeth diagnosed with reversible pulpitis (RP) and crowned without RCT.11 The authors looked at eight thousand one hundred and seventy-five patients referred for evaluation and treatment during a six-year period. Cases with RP were treatment planned for crowns regardless of peri-apical diagnosis. Of the 127 teeth diagnosed with reversible pulpitis, 27 converted to irreversible pulpitis or to a necrotic pulp, which equaled 21% of the total. The outcome of that particular study indicated that if a crack was identified early enough and a crown was placed in cases diagnosed with reversible pulpitis, root canal treatment would be necessary in about twenty percent of cases within a six-month period. Similar studies have indicated that 15-19% of teeth required endodontic treatment after crown placement12. Therefore, the conclusion of Krell and Rivera was only slightly higher. These studies underscore the difficulty in predicting whether a cracked tooth will eventually need root canal treatment and the communication with one’s patient. Based on the current evidence, it is the author’s advice to quote to patients that 10-20% of cracks will eventually need root canal treatment, however, early diagnosis and treatment will only prevent irreversible pulpal inflammation. The diagnosis of RP must always be considered a temporary diagnosis until the pulp can be re-evaluated, which usually occurs six to eight weeks later. The longer the time period before re-evaluation, the easier it is for a clinician to distinguish between irreversible pulpitis, pulp necrosis or normal pulp and to formulate the appropriate treatment plan.
Another important decision a clinician faces is whether to keep a tooth with a crack in the root canal chamber or to extract and replace such a tooth. The success of dental implants has resulted in substantial shifts in treatment planning paradigms. The success of endodontic treatment is comparable to that of single tooth implants.13 However, this does not include cracked teeth. Long-term data clinical studies regarding the survival of cracked teeth are scarce. Sim et al., in February 2016, looked at 86 cracked root filled posterior teeth.14 All teeth were treated by endodontists and restored with full coverage restoration unless the patient opted out, in which case an amalgam core and orthodontic band was placed. At the time of endodontic treatment, the extent of the crack was recorded using an SOM and methlyne blue staining. Multivariable analysis showed that if the crack extended onto the pulpal floor, the odds of tooth loss increased 11-fold with other factors remaining constant. They concluded that a five year survival rate of root filled posterior teeth in the absence of cracks on the pulpal floor was 95% versus 81% in the presence of extension of cracks onto the pulpal floor.14
FIGURE 3. Flow chart outlining the author’s protocol for managing teeth with cracks and pulpal inflammation.
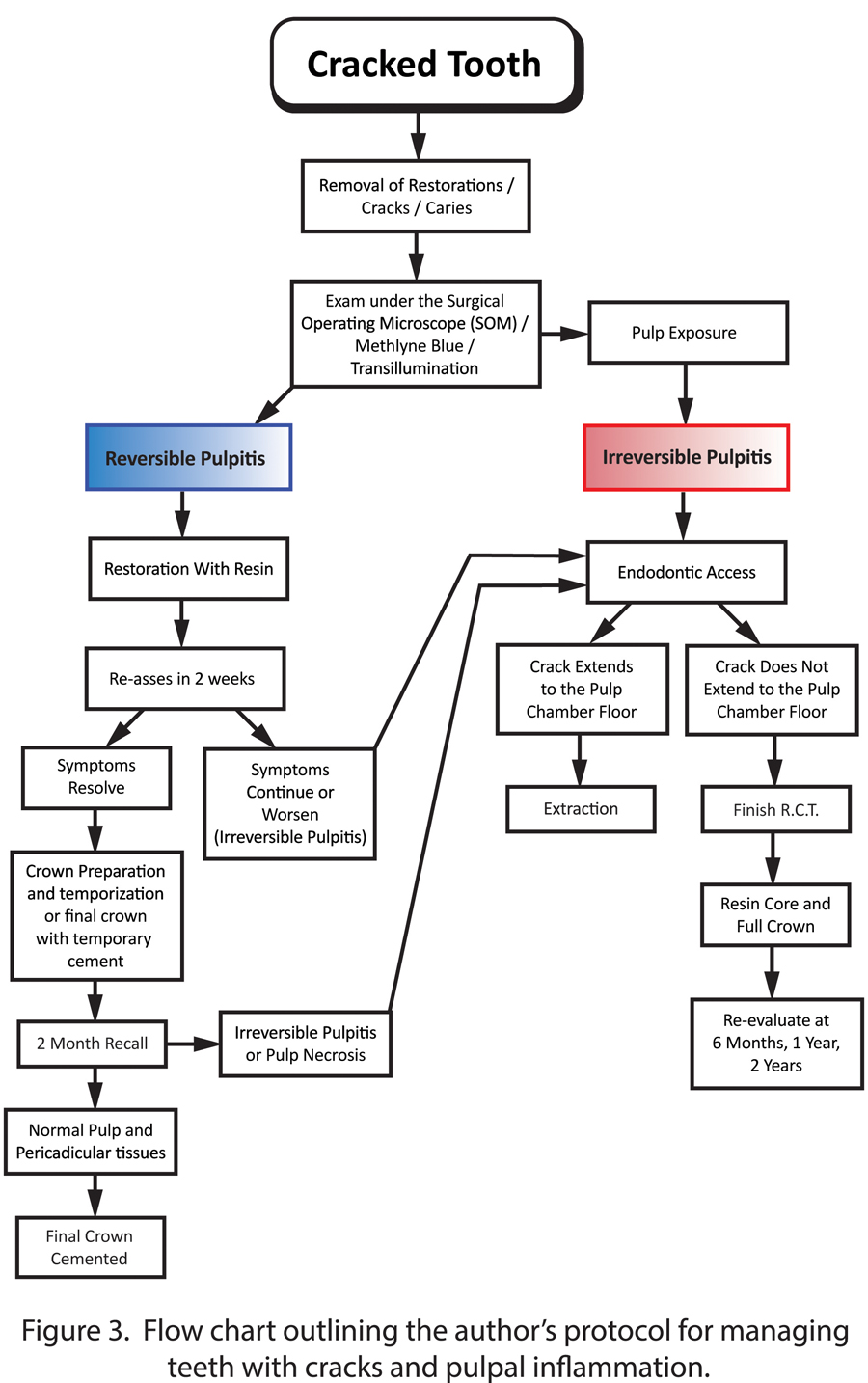
The aim of this article was to provide information regarding diagnosis and treatment of cracked teeth. Figure 3 was constructed to help the clinician navigate the difficult treatment planning when approaching cracked teeth. Provided that there is an accurate diagnosis of the pulp status and its cause, teeth with reversible pulpitis due to cracks can be treated conservatively without the need for root canal therapy in approximately 80% of cases. Only when the crack extends onto the pulpal floor does the long-term prognosis change, and extraction and replacement should be considered. Coronal cracks can be predictably treated. Endodontic treatment may be required for mechanical, restorative, or pulp inflammation if the crack extends into the pulp chamber. Timely diagnosis and treatment planning of cracked teeth will be particularly helpful when treating an aging population especially when cracks are a diagnostic and restorative challenge. OH
Dr. Geoffrey Sas is an Endodontist who received his post-graduate training at Nova Southeastern University. He is a Fellow of the Royal College of Dentists of Canada. Dr. Sas maintains a private practice in Toronto, and is a clinical instructor, part-time, at the University of Toronto. He can be reached at glsas@yorkhillendo.com.
Oral Health welcomes this original article.
References
1 .Ehrmann EH, Tyas MJ. Cracked teeth syndrome: diagnosis, treatment and correlation between symptoms and post extraction findings. Aus Den J 1990; 35: 105-112.
2. Ailor JE Jr. Managing incomplete root fractures. J Am Dent Assoc 2000;131: 1168-74.
3. Opdam NJM, Roeters JM, Loomans AC, Brokhorst EM. Seven-year Clinical Evaluation of Painful Cracked Teeth Restored with a Direct Composite Restoration. 2008; 34: 808-811.
4. Turp JC, Gobetti JP. The Cracked tooth syndrome: an elusive diagnosis. J AM Dent Assoc. 1996;127: 1502-7.
5. Cracking the cracked tooth code. Endodontics: Colleagues for Excellence 1997 (Fall/Winter) 1-13.
6. Abbot P, Leow W. Predictable management of cracked teeth with reversible pulpitis. Aus Dent J 2009; 54:306-15.
7. Love RM. Bacterial penetration of the root canal intact incisor teeth after a simulated traumatic injury. Endod Dent Traumatol 1996; 12:289-293.
8. Clark DJ, Sheets CG, Paquette JM. Definitive Diagnosis of Early Enamel and Dentinal Cracks Based on Microscopic Evaluation. J Esthet Restor Dent 2003. 15:XXX-XXX.
9. Transillumination: The “Light Detector: Endodontics: Colleagues for Excellence 2008 (Bonus Material) 1-2.
10. Signore A, Benedicenti S, Covani U, Ravera G. A 4- to 6 year retrospective clinical study of cracked teeth restored with a bonded indirect resin composite onlays. Int J Prosthodont 2007;20:609-16.
11. Krell K, Rivera EM. A six year Evaluation of Cracked Teeth Diagnosed with Reversible Pulpitis: Treatment and Prognosis. J Endod 2007;33:1405-7.
12. Cheung GS, Lai SC, Ng RP. Fate of vital pulps beneath a metal-ceramic crown or a bridge retainer. Int Endod J 2005;38:521-30.
13. Holm-Pederson P, Lang NP, Muller F. What are the longevities of teeth and oral implants? Clin Oral Implants Res 2007;18 (suppl 3):15-9.
14. Sim I. Lim TS, Krishnaswamy G, Chen N. Decision Making for Retention of Endodontically Treated Teeth: A 5-year Follow Up Study. JOE 2016;42:225-29.











