
Patients often avoid dental care due to the fear of pain that they perceive they will feel either related to the local anesthetic injection or during drilling to remove caries. This can be especially traumatic for pediatric patients who can be uncooperative following the sensation of the injection.1 Frequently; the hard tissue laser allows treatment without the need for local anesthetic. Additionally, the vibration and sound associated with the dental handpiece during caries removal increases patient stress while in the chair for needed treatment. This may lead to treatment avoidance until the actual intraoral pain surpasses the feared pain of treatment. Providing a more comfortable experience for the patient aids in patients accepting and following through on dental care at an earlier stage. This can also be a significant practice builder.
A hard tissue laser allows the practitioner to remove carious tooth structure while preserving healthy enamel and dentin for truly minimal invasive dentistry. The more of the native tooth structure that can be preserved, the better the long-term prognosis.
Given the larger pulps of deciduous teeth, there has been a concern that use of hard tissue laser energy may cause pulpal changes that can ultimately require endodontic treatment. However, several recent studies have demonstrated that the Er:YAG hard tissue laser was appropriate for caries removal in primary teeth.2 As lower energy is required for the photo-ablation of primary enamel and dentin (compared to permanent enamel and dentin) due to a higher presence of water and lower presence of minerals, adverse pulpal changes have not been reported.3
Ceballos reported that the Er:YAG laser irradiation resulted in a 56% reduction in primary enamel surface lesion depth (vs the acid-etched group) and a 39% decrease in root surface lesion depth.4 This appears to be related to the laser’s bactericidal effects in the caries-affected dentin and beyond.5 There is also less post-treatment sensitivity in teeth treated with the Er:YAG laser (vs traditional cavity preparation methods). Lasers can also treat hypersensitive root surfaces with minimum invasiveness, demonstrating effective results.6,7
Laser Usage in the Modern Dental Practice
Lasers have become a standard feature in the dental practice, enhancing treatment in both hard and soft tissue applications. Diode lasers (i.e. Picasso, AMD LASERS, Indianapolis, IN) are designed for soft tissue applications. These allow the practitioner to remove gingival tissue to expose root caries, esthetically recontour gingival tissues, to treat periodontal pockets and a range of other applications that present daily in the typical practice. Er:YAG lasers are suited for use in hard tissue treatment as their wavelength (2940 nm) has an affinity for hydroxyapatite and water. Diodes at 810nm have an affinity for hemoglobin and melanin, making them ideal for soft tissue applications. Although, Er:YAG lasers will cut soft tissues and diodes faster with superior coagulation benefits (Fig. 1).
FIGURE 1. Lasers used in dentistry and their affinity to oral materials.

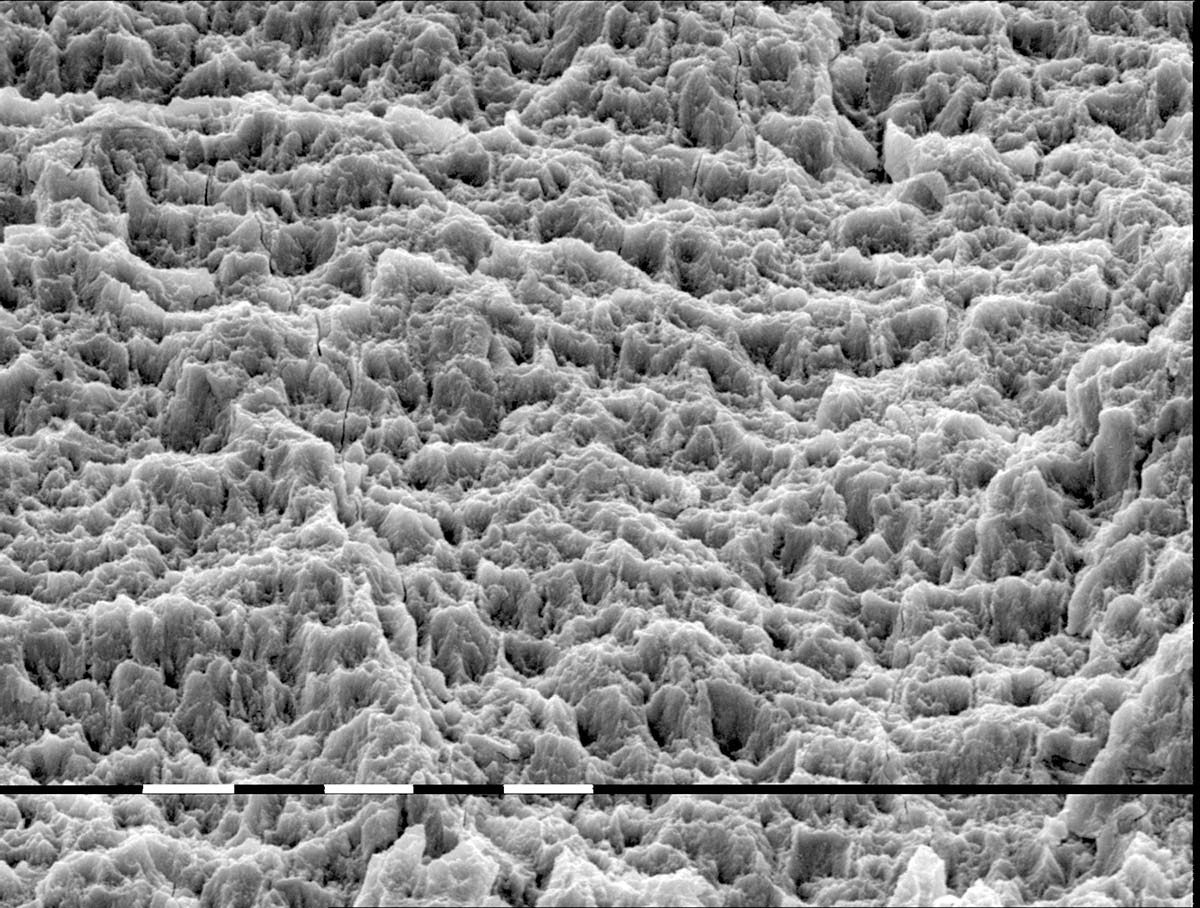
Er:YAG hard tissue lasers, such as the LiteTouch™ (Syneron, distributed by AMD LASERS), (Fig. 2) are utilized for caries removal, frequently without the need for local anesthesia; the laser is used in a non-contact mode and desensitizes the odontoblastic processes in the dentin. Both the vibration and the sound of the dental drill are completely eliminated. The laser preparation has no bur vibration; hence there is no micro-fracturing of the surrounding enamel. Unlike the smear layer left by rotary burs on the treated dentin surface, the laser ablates both dentin and enamel without leaving a carbonized surface behind8 (Fig. 3).
FIGURE 2. LiteTouch Er:YAG laser (AMD LASERS).

FIGURE 3. Dentin surface following caries removal with the LiteTouch Er:YAG laser demonstrating a lack of smear layer. (Courtesy of Prof. Georgi Tomov, Plovdiv University- Bulgaria).

Enamel and dentin have different water contents. Thus, the energy used to ablate (remove) dentin with its higher water content is different from that of enamel. Typically, 25 Hz is optimal for enamel and 30 Hz for dentin.9 Additionally, lasers have a bactericidal effect on dentin, leaving a sterile surface for the bonded restoration. This decreases the pulpal flare-ups that can cause tooth sensitivity and the possible need for endodontic treatment.
Treatment of the enamel margins with the LiteTouch laser yields a surface with an enhanced bonding surface (no need for acid etching). The Er:YAG removes the prismatic substance around the rods (Fig. 4) Increased retention has been found when demineralized enamel was prepared with laser compared to acid etching.10 Er:YAG lasers are effective for ablation of hard tissues, creating an irregular and microretentive morphological pattern without hard tissue damage.11
FIGURE 4. Enamel surface following treatment with the LiteTouch Er:YAG laser showing an enhanced bondable surface with a uniform roughen surface. (Courtesy of Prof. Georgi Tomov, Plovdiv University- Bulgaria).
Prior to sealants, the laser conditions the enamel for better bonding and eliminates the less-than-pleasant taste of the etching gel.12 This facilitates pediatric patient management by eliminating the child’s major objections. The laser eliminates bacteria within the pits and fissures, decreasing the potential for recurrent decay under the sealant. Laser enamel conditioning before sealant application appears to reduce sealant fracture and loss. This is possibly related to the micro-morphological changes that the laser leaves on the enamel surface.13
FIGURE 5. Caries noted in the distal pit of a first molar. (Courtesy of Makoto Kamiya, DDS Matsumoto City, Japan).

FIGURE 6. Preparation following caries removal with the LiteTouch Er:YAG hard tissue laser demonstrating a minimally invasive preparation performed without the need for local anesthetic ready for restoration placement. (Courtesy of Makoto Kamiya, DDS, Matsumoto City, Japan).

The hard tissue laser is more conservative than a traditional bur in developing cavity access (Figs. 5 & 6) In clinical situations where soft tissue has invaded the cavity, or needs to be excised to expose the decay, the Er:YAG removes the tissue, coagulating the bleeding margin that often interferes with the placement of an adhesive restoration (Figs. 7 & 8).
FIGURE 7. Significant caries noted on the mesial of a deciduous molar with soft tissue ingrowth into the area. (Courtesy of Makoto Kamiya, DDS, Matsumoto City, Japan).

FIGURE 8. Caries and soft tissue removal with the LiteTouch Er:YAG laser without application of local anesthetic ready for restoration placement. Note an absence of bleeding at the altered soft tissue margin. (Courtesy of Makoto Kamiya, DDS, Matsumoto City, Japan).

The hard tissue laser removes old composite restorations as effectively as it removes tooth structure.14 A failing amalgam is better addressed by a handpiece and bur. The laser then cleanses the preparation surface, sterilizing the dentin, and conditioning both the enamel and dentin for the adhesive restoration. Lasers are effective in debonding orthodontic brackets and the removal of the remaining luting resin on the teeth.16
Dentin hypersensitivity can cause discomfort and even severe pain. A two-minute Er:YAG laser application to the exposed cervical root areas has been found to provide lasting desensitization of the hypersensitive dentin, with no detrimental pulpal effects. Laser treatment has been shown to be efficacious and typically demonstrates relief at the first appointment.15
FIGURE 9. LiteTouch Er:YAG handpiece held in a similar manner to a traditional dental handpiece.

Conclusion
Hard tissue lasers such as the LiteTouch Er:YAG have many clinical applications. These include anesthetic-free caries removal and the conservative removal of old composites or orthodontic resin. This preserves more natural tooth structure, increasing the long-term prognosis of the tooth. As the laser handpiece is similar to a traditional dental handpiece, its incorporation into the practice has a short and easy learning curve (Fig. 9). OH
Dr. Kurtzman is in private general practice in Silver Spring, Maryland and is a former Assistant Clinical Professor at the University of Maryland, Baltimore School of Dentistry, Department of Endodontics, Prosthetics and Operative Dentistry. He is a consultant for multiple dental companies and has earned Fellowship in the AGD, AAIP, ACD, ICOI, Pierre Fauchard, Academy of Dentistry International, Mastership in the AGD and ICOI and Diplomat status in the ICOI and American Dental Implant Association (ADIA). He can be contacted at dr_kurtzman@maryland-implants.com.
Oral Health welcomes this original article.
References:
1. Prathima GS, Bhadrashetty D, et al: Microdentistry with Lasers. J Int Oral Health. 2015 Sep;7(9):134-7.
2. Valério RA, Borsatto MC, et al.: Caries removal in deciduous teeth using an Er:YAG laser: a randomized split-mouth clinical trial. Clin Oral Investig. 2016 Jan;20(1):65-73. doi: 10.1007/s00784-015-1470-z. Epub 2015 Apr 17.
3. Zhegova G, Rashkova M, Rocca JP: Minimally invasive treatment of dental caries in primary teeth using an Er:YAG Laser. Laser Ther. 2014 Dec 27;23(4):249-54. doi: 10.5978/islsm.14-OR-18.
4. Ceballos L, Toledano M, et al.: ER-YAG laser pretreatment effect on in vitro secondary caries formation around composite restorations. Am J Dent. 2001 Feb;14(1):46-9.
5. Folwaczny M, Aggstaller H. et al.: Removal of bacterial endotoxin from root surface with Er:YAG laser. Am J Dent. 2003 Feb;16(1):3-5.
6. Yu CH, Chang YC: Clinical efficacy of the Er:YAG laser treatment on hypersensitive dentin. J Formos Med Assoc. 2014 Jun;113(6):388-91. doi: 10.1016/j.jfma.2013.02.013. Epub 2013 Apr 18.
7. Sgolastra F, Petrucci A, et al.: Lasers for the treatment of dentin hypersensitivity: a meta-analysis. J Dent Res. 2013 Jun;92(6):492-9. doi: 10.1177/0022034513487212. Epub 2013 Apr 22.
8. Lima DM, Tonetto MR, et al.: Human dental enamel and dentin structural effects after Er:YAG laser irradiation. J Contemp Dent Pract. 2014 May 1;15(3):283-7.
9. Rizcalla N, Bader C, et al.: Improving the efficiency of an Er:YAG laser on enamel and dentin. Quintessence Int. 2012 Feb;43(2):153-60.
10. Guedes SF, Melo MA, et al.: Acid etching concentration as a strategy to improve the adhesive performance on Er:YAG laser and bur-prepared demineralized enamel. Photomed Laser Surg. 2014 Jul;32(7):379-85. doi: 10.1089/pho.2013.3655.
11. Freitas PM, Navarro RS, et al.: The use of Er:YAG laser for cavity preparation: an SEM evaluation. Microsc Res Tech. 2007 Sep;70(9):803-8.
12. Unal M, Hubbezoglu I, et al.: The effect of Er:YAG laser and different surface conditioning procedures on microtensile bond strength of the fissure sealant containing amorphous calcium phosphate after artificial aging. Dent Mater J. 2014;33(1):21-6.
13. Maddalone M, Ferrari M, et al.: Enamel laser conditioning before sealant application. Stomatologiia (Mosk). 2012;91(6):25-7.
14. Correa-Afonso AM, Pécora JD, Palma-Dibb RG.: Influence of pulse repetition rate on temperature rise and working time during composite filling removal with the Er:YAG laser. Photomed Laser Surg. 2008 Jun;26(3):221-5. doi: 10.1089/pho.2007.2120.
15. Sgolastra F, Petrucci A, et al.: Lasers for the treatment of dentin hypersensitivity: a meta-analysis. J Dent Res. 2013 Jun;92(6):492-9. doi: 10.1177/0022034513487212. Epub 2013 Apr 22.
16. Almeida HC, Vedovello Filho M, et al.: ER: YAG laser for composite removal after bracket debonding: a qualitative SEM analysis. Int J Orthod Milwaukee. 2009 Spring;20(1):9-13.
Follow the Oral Health Group on Facebook, Instagram, Twitter and LinkedIn for the latest updates on news, clinical articles, practice management and more!











