
Missing or impacted teeth can often accompany a patient throughout their lifetime. A maxillary lateral incisor is the third most common congenitally missing tooth in the dentition and affects nearly two percent of the population. Esthetics and function can easily become compromised due to the change or minimized spatial dynamics of the arch when this occurs. These patients present with a unique set of challenges in which careful diagnosis and thorough treatment options need to be developed to satisfy the patient’s expectations.
Selecting the proper treatment for a case like this is not simple and straightforward. Factors such as the patient’s age, occlusion, profile, tooth anatomy, smile line, bone quality and quantity become important guiding principles to restore the missing incisor. The over-riding goal of treatment options for a patient with such a presentation should be two fold–considering space creation as well as root position for future treatment. By orthodontically opening the space, especially if the patient is young, the clinician is allowed more flexibility with restorative options, especially over the patient’s lifetime. Another option would be to allow the space to close. This choice not only can dictate the occlusion due to the influence of a canine replacement, but also may reflect a difficult and more upredictable esthetic result due to tooth size and shape. Prosthetic choices narrow with this avenue and may create an obsolete restorative path.
If the chosen treatment is to open or create space representing the lateral incisor, the focus becomes on how much space to appropriate for the best esthetic outcome. Several methods can be utilized by the restoring dentist working in tandem with the multi-discipline team. Perhaps the easiest method is to compare the contralateral side and restore to that presentation. Secondly, clinicians may apply the golden proportions ratio–when moving distally, each tooth should present a 61.8 percent in comparison correlation of the previous tooth. Another theory is mathematically determing the arch comparisons using the Bolton analysis. And finally, the actual space itself may be dependent upon the concluding occlusal scheme.
Other aspects of the hypodontia pose influence and may introduce more clinical dilema. Clinicians must recognize how the adjacent and opposing teeth can possibly shift or re-position into a non-favorable esthetic and occlusal relationship. The teeth surrounding the lateral incisor space are affected and tooth wear can become another significant consequence of the arch length discrepancy. Severe or excessive tooth wear can become problematic, creating a disproportionate dental architecture. In particular, incisal attrition may result due to physiological wear and further influenced by parafunctional habits such as clenching or bruxism.
At the present time, the most common treatment recommendations to deal with a missing lateral incisor are canine substitution and a single tooth implant. Other restorative alternatives are a resin-bonded fixture (Maryland bridge), a fixed partial denture (bridge), or a removable partial denture. Regardless of what treatment considerations are made for the congenitally missing tooth, the clinician must also be mindful of the adjacent teeth, if they too become restoratively involved. Anatomic proportions and relationships must be used to ensure esthetics, functionality, and restoration longevity.
This case will examine how a multi-discipline approach of orthodontics and prosthetics were used to effectively reintroduce a congenitally missing lateral incisor into the maxillary arch, restoring esthetics and function.
Case Study
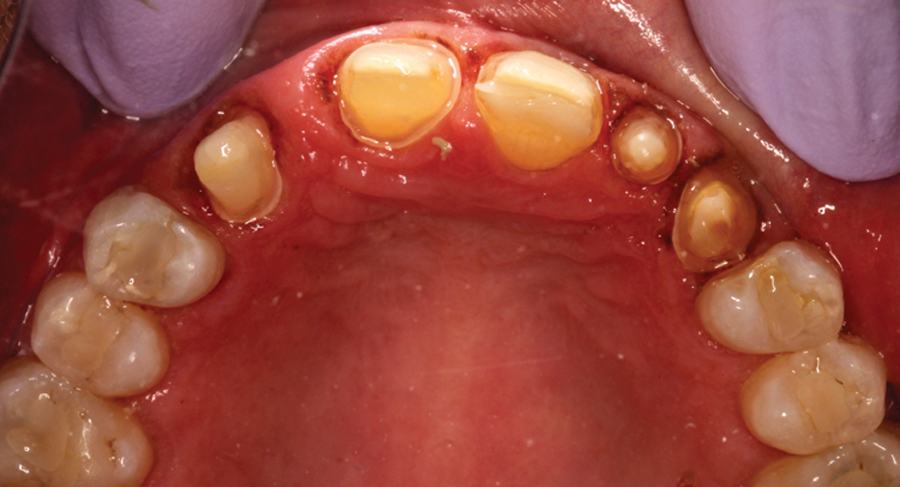
A 59-year-old patient initally presented to the office with porcelain crowns on two maxillary anterior teeth (Fig. 1), multiple composite restorations, anterior incisal wear, generalized abfraction in the maxillary arch, and a congenitally missing maxillary left lateral incisor. She stated her desire was to achieve “a younger looking smile”.
FIGURE 1. Initial presentation.

To gather appropriate information for treatment direction–photographs, study models, and a bite relationship were made. Careful measurements were made of both arches as seen in Figure 2 and 3. Due to the congenitally missing left lateral incisor, a significant arch length discrepancy was noted, the midline varied, and her esthetics were disproportional. Also, approxiamately a 1.5mm space existed mesial and distal to the left maxillary canine, tooth #11.
FIGURE 2. Initial Maxillary occlusal view.

FIGURE 3. Initial Mandibular occlusal view.

Treatment Plan
Several treatment options were discussed. After measuring tooth sizes and comparing contralateral esthetics, the size of the canine currently occupying the lateral position posed unpredictable esthetics. If the canine could be moved distally, improved esthetic symmetry was possible. The patient clearly understood that orthodontic correction could lay the foundation for a multi-faceted result–allowing for space to be established for the missing left lateral incisor, distalization of the canine, as well as control the final esthetic outcome. The ultimate restorative endpoint would allow for placement of a possible implant in the newly formed lateral incisor position in combination with anterior crowns or veneers.
Orthodontic Phase
The treatment goals were relayed to the orthodontist to begin phase I treatment–adult orthodontics. Orthodontic care was completed in approximately 14 months as shown in Figure 4 and 5. The ultimate goal to distalize the canine was achieved, however, only 5 mm of lateral tooth space was re-captured. Two hurdles were met at this treatment juncture. First, until the treatment plan could be finalized and a diagnostic wax-up completed, the arch and space required retention. An ACE Plastics aligner with a pontic in the lateral space, #10 was fabricated as shown in Figure 6. Next, due to the size of the regained space and contralateral esthetics, the decision was made not to go forward with placing an implant. Options would focus on fixed esthetics to restore the space.
FIGURE 4. Orthodontic completion.

FIGURE 5. Orthodontic completion – Maxillary view.

FIGURE 6. Essix aligner with #10 pontic.

Preparation
The final restorative decisions involved guiding principles of esthetics as previously mentioned as well as visual and functional direction from a diagnositc wax-up created by the ceramist. The patient approved the ultimate definitive treatment plan and wax-up. From the wax-up, a provisional shim was made using TempSpan Clear (Pentron) for the future provisionals.
After administering local anesthetic, crowns were prepared on teeth #6 and #7. To conserve tooth structure, the right maxillary central, #8 was prepped for a veneer. Bridge abutments were prepared on the maxillary left central and canine, spanning the newly resumed pontic space, #10. Retraction cord, Knit-Pak size 0 (Premier Dental) was carefully placed into each tooth’s sulcus, followed by placement of Traxodent (Premier Dental). Figure 7 displays the tooth preparations after the impression was made using Aquasil Ultra Rigid tray material and Aquasil Ultra LV wash material.(Dentsply.Caulk). A rigid bite registration caputured the intra-occlusal relationship and the final Shade B1 was selected.
FIGURE 7. Tooth preparations.
Provisionals were fabricated with the use of the earlier created shim filled with Integrity Multi-Cure, shade B1 (Dentsply.Caulk). The temporaries were made as one unit, finished with fine diamonds and discs, and then polished with Enhance discs (Dentsply.Caulk) as shown in Figure 8. This transitional unit was temporarily cemented with TempGrip (Dentsply.Caulk).
FIGURE 8. Provisionals.

Final Restorative Phase
Two weeks later, the patient returned for her final restorative appointment. She stated she was very “pleased” with her temporaries and “found herself smiling more”. The patient was made comfortable with a locally administered anesthetic. The transitionals were removed, each preparation was cleansed using a microbrush with two percent chlorhexidine, and all indirect restorations were tried-in. Final restorations were constructed of IPS e.max (Ivoclar Vivadent) for high esthetics, durability, and strength. After securing the fit of each restoration, each unit was cleansed with Ivoclean (Ivoclar Vivadent) for 20 seconds, rinsed and dried, and then finally readied with a ceramic primer application. Isolation was achieved using an OptraGate (Ivoclar Vivadent). The crowns and bridge abutments were cemented using a self-adhesive resin cement, Calibra Universal, Translucent shade (Dentsply.Caulk). The veneer on tooth #8 was placed using a total etch technique – 34 percent phosphoric etch for 15 seconds, rinsed for 5 seconds, lightly suctioned to allow the dentin to remain moist, and Elect Universal (Dentsply.Caulk) bond application of 20 seconds, followed by a 10 second light cure. Calibra Esthetic Veneer cement, Translucent shade (Dentsply.Caulk) was placed into the prepared veneer, seated and gingivally tack cured. All restorations were finalized with fine diamonds, polished, and occlusion re-verified (Figs. 9 & 10).
FIGURE 9. Final restorations.

FIGURE 10. Final restorations – Occlusal view.

The patient was extremely pleased with her final result. To address her clenching, a Kombiplast night guard (Dentsply, Raintree Essix) was fabricated for her maxillary arch.
Conclusion
Hypodontia can be present for a lifetime and can potentially lead to unfavorable esthetics and dental conditions. Since there is no absolute decisive treatment, an inter-disciplinary team combined with a comprehensive treatment approach using guiding principles can achieve the best possible esthetic and functional outcome for the patient. Congenitally missing teeth can be esthetically challenging, but by working in tandem with the patient, their expectations and compliance, lateral transformation is possible. OH
Acknowledgement: The author would like to thank Dan Becker at Becker Dental Laboratory for his ceramic expertise.
Lori Trost maintains a private practice in Columbia, IL, merging contemporary esthetic dentistry with a minimally invasive approach to patient care. She has authored a wide variety of articles found in numerous dental publications, is a clinical evaluator and consultant, and ad ADA Shils Foundation recipient for Leadership. Dr. Trost is an accomplished lecturer and presents on a regular basis throughout the United States and Canada, sharing her vision and approach to everyday dentistry that is informational, motivational, and refreshing. You may contact her at: trost@htc.net.
Oral Health welcomes this original article.











