
CASE REPORT
A 21-yr-old male initially presented to emergency department (ED) of the hospital with pericoronitis (pain, buccal and submandibular swelling) related to his impacted teeth. He was given antibiotics for a week until the wisdom teeth were removed in the office under IV sedation. The patient’s post-operative course was uneventful. The patient returned to the ED 10 months later with an progressively enlarging neck swelling and mild dysphagia. The patient had no breathing issues, however the patient did notice a slight difference with extreme exercise. The swelling was more apparent to his family members. The patient was otherwise healthy. The large submental swelling was soft, non-tender and non-pulsatile. Intraoral examination showed a large smooth floor of the mouth with mild displacement of the tongue. The MRI showed a 6cm x 4cm x 3cm “egg shaped” cystic lesion (Figs. 1a & b). The patient was taken to the operating room where the lesion was removed via a transcervical incision and removed ‘en bloc’ (Fig. 2) and submitted to pathology. The postoperative course was uneventful. Histopathology confirmed the diagnosis of a dermoid cyst (Fig. 3 a & b).
FIGURES 1A & 1B. MRI views of the ‘Egg shaped” lesion. Note: the superior displacement of the tongue and floor of the mouth.
FIGURE 1A. FIGURE 1B.


FIGURE 2. Specimen from the surgical enucleation via transcervical approach.

FIGURE 3A. Small adnexal structures were also seen in the cyst wall.
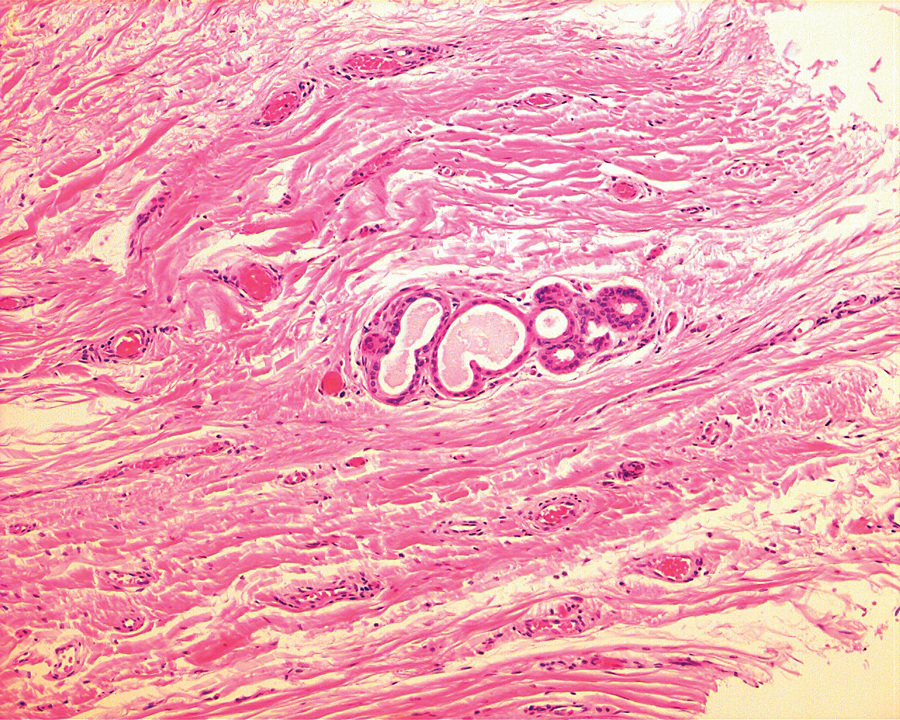
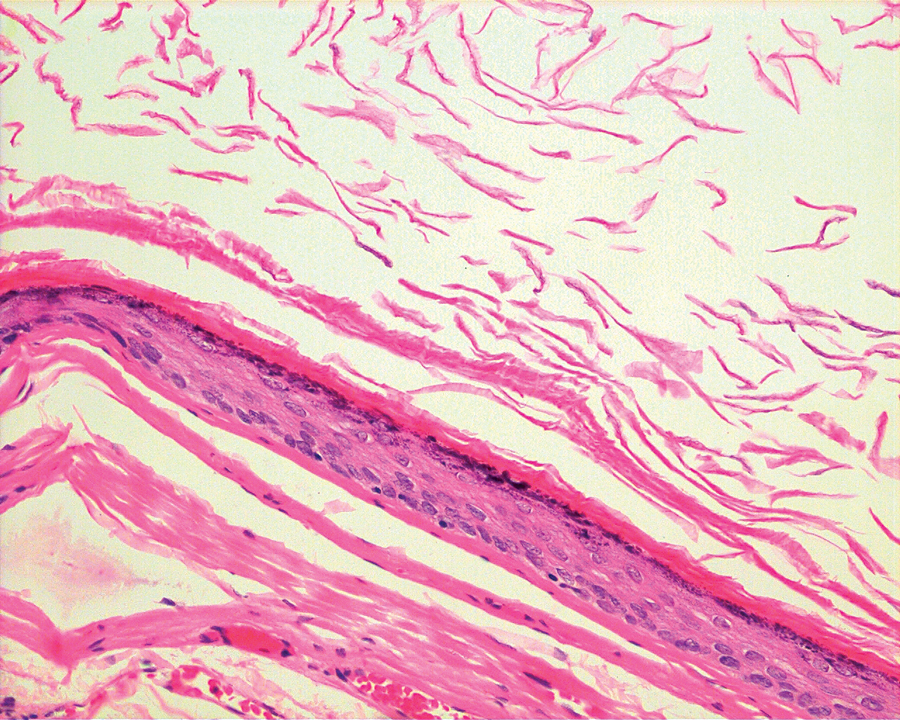
FIGURE 3B. The cyst was lined by keratinizing stratified squamous epithelium with granular cell layer.
Dermoid cysts of the head and neck are not common. It has been estimated that up to 6.9% of all body dermoid cysts occur at this site.1 They usually occur in the second or third decades of life.2 The most common location in the head and neck region is the lateral third of the eyebrow area, with 23% to 34% found in the floor of the mouth.3,4 The vast majority of dermoid cysts of the floor of the mouth are located in the midline (sublingual 53% and submental 26%), 16% involve more than one of the three anatomic spaces of the floor of the mouth (submental, sublingual and submandibular) and up to 6% are located only in the submandibular space, and clinically present as lateral neck cysts.5
Patients often present with a slow-growing, painless, doughy mass that may show pitting with finger pressure. However, these lesions can become secondarily infected and present as significant fascial space infections.6 The swelling involves one or more of the sublingual, submental and submandibular spaces and can develop to significant dimensions before producing symptoms. Cystic lesions developing superior to the mylohyoid muscle have the potential to displace the tongue toward the palate resulting in difficulty with mastication, dysphagia, speech difficulties and airway obstruction.7 For cystic lesions developing below the mylohyoid musculature, a submental or submandibular swelling is observed.
Diagnostic imaging modalities include CT, MRI and ultrasonography. On CT scans, dermoid cysts appear as well defined, unilocular, fluid filled hypodense lesions.2 On MRI scans, dermoid cysts typically generate low signal on T1 images and high signal on T2 images.8
The only effective treatment option is surgical enucleation. Various surgical approaches can be used depending on the position of the lesion relative to the geniohyoid and mylohyoid muscles. Floor of mouth lesions located superficial to these muscles often can be removed via a trans-oral approach. For larger lesions, and lesions mostly in the submental or submandibular region, a trans-cervical approach is favoured.1 The cyst wall is characteristically smooth and thick, allowing for easier dissection from the surrounding tissues.1 Cyst contents are variably keratinous, caseous, sebaceous or purulent with hair, nails, fat globules, and cholesterol clefts.1 Histologically, dermoid cysts are lined with a stratified squamous epithelium with adnexal tissues, such as hair follicles, sweat glands and sebaceous glands. In the absence of adnexae, the histologic diagnosis would be an epidermoid cyst. The diagnosis of a teratoma would be made if all three germinal layers were represented in the cyst wall.7
There are two theories involving the development of dermoid cysts. Most researchers believe that the midline floor of mouth dermoid cysts are as a result of entrapped ectodermal tissue of the first and second branchial arches, which fuse during the third and fourth weeks in utero.9 Another theory suggests that these cysts may be a variant of the thyroglossal duct cyst with ectodermal elements predominating.10
The differential diagnosis of this lesion broadly includes neoplasms, infections/inflammations, salivary gland mucous extravasation phenomena and developmental processes.7 Neoplastic lesions may include benign and malignant salivary gland tumours, lipomas, lymphangiomas, neurofibromas, lymphomas and metastatic lesions. Infections may include odontogenic and salivary gland etiologies as well as granulomatous infections such as mycobacterial disease, actinomycosis and histoplasmosis. Wegener’s granulomatosis and sarcoidosis are some examples of non-infectious granulomatous conditions. Plunging ranulae and mucoceles must also be considered. Developmental anomalies include thryoglossal duct cysts, cystic hygromas and branchial cleft cysts.2,7 OH
Dr. Green is an Oral and Maxillofacial Surgeon in private practice in Stoney Creek, ON and on staff at Hamilton Health Sciences.
Dr. Turner is an Otolaryngologist, Chief of Surgery, Thunder Bay Regional Health Sciences Center, Thunder Bay, ON.
Dr. Kennedy is a Pathologist, Thunder Bay Regional Health Sciences Center, Thunder Bay, ON.
Dr. Pynn is an Oral and Maxillofacial Surgeon, Thunder Bay Regional Health Sciences Center, Thunder Bay, ON.
Oral Health welcomes this original article.
REFERENCES
1. Pirgousis P, Fernandes R. Giant submental dermoid cysts with near total obstruction of the oral cavity: report of 2 cases. J Oral Maxillofac Surg 69: 532-535, 2011.
2. Teszier CB, El-Naaj IA, et al. dermoid cysts of the lateral floor of the mouth: a comprehensive anatomo-surgical classification of cysts of the oral floor. J Oral Maxillofac Surg 65: 327-332, 2007.
3. Taylor BW, Erich JB. Dermoids of the head and neck. Minn Med 49: 1535-1540, 1966.
4. Reddy VS, Radhakrishna K, Rao PL. Lingual dermoid. J Pediatr Surg 26: 1389-1390, 1991.
5. King RC, Smith BR, Burk JL. Dermoid cyst in the floor of the mouth. Review of the literature and case reports. Oral Surg Oral Med Oral Pathol 78(5): 567-576, 1994.
6. Seah TE, Sufyan W, Singh B. Case report of dermoid cyst at the floor of the mouth. Ann Acad Med Singapore 33(suppl): 77S-79S, 2004.
7. Louis PJ, Hudson C, Reddi, S. Lesions of the floor of the mouth. J Oral Maxillofac Surg 60: 804-807, 2002.
8. Turki IM, Kaddour AK, Wann AR, et al. Dermoid cyst of the submandibular space. Fr ORL 89: 167-169, 2005.
9. Walstad W, Soleman J, Schow S, et al. Midline cystic lesion of the floor of the mouth. J Oral Maxillofac Surg 56: 70-74, 1998.
10. Demello D, Lima J, Liapis H. Midline cervical cyst in children: thyroglossal anomalies. Arch Otolaryngol Head Neck Surg 113: 418-420, 1987.











