
Abstract
Administration of an inferior alveolar nerve block is a routine technique in clinical practice. Despite mid-century advancements in armamentarium alloy properties, responsible for a significant decline in needle fracture incidence, cases of needle fracture upon local anesthesia administration continue to be reported. Techniques of prevention are paramount. Management of retrieval may pose a challenge to the oral and maxillofacial surgeon and interventions to aid in surgical localization of fragments prove useful.
Introduction
The complication of local anesthesia needle fracture is a rare occurrence; however, cases of such incidence continue to be reported in the literature.1 Often, needle fractures occur in the setting of pediatric patients who move abruptly as the clinician administers an inferior alveolar nerve block.1-3 The inferior alveolar nerve block is thought to predispose to needle fracture due to the relatively constricting anatomy in the locale of administration.1 Upon insertion, the medial border of the ramus and the lateral aspect of the medial pterygoid muscle flank the needle. The pterygomandibular space is the most common site for displacement following needle fracture.4 Furthermore, inappropriate administration techniques, as well as particular needle characteristics, have also been implicated in needle fracture at the time of insertion. The inferior alveolar nerve block technique of identifying the inferior oblique ridge of the mandible with the needle and proceeding to reposition the needle posteriorly to the level of the lingula may also increase the risk of fracture.1 Using a short and/or small diameter needle, bending the needle prior to use and inserting the needle to the hub have all been associated with reports of needle fracture.1-4 Technical modifications have been described for the prevention of needle fractures, including choosing the appropriate length and gauge, avoid needle strain or bending, not burying the needle to the hub, as well as good communication with the patient to avoid sudden unanticipated movements. Options following needle fracture include no treatment and monitoring, primary removal (removing immediately) or secondary removal (allowing a period of fibrosis prior to removal).
Indications for needle fragment primary removal include: close proximity to vital structures, prevention of infection, psychologic stress, pain, dysphagia, trismus and damage-causing migration toward vital structures.2,3 Often the fractured needle can be visualized. Other times it cannot and retrieval becomes a secondary surgical adventure. Retrieving needle fragments, once fractured and not visible in the oral cavity, remains a challenging role for the oral and maxillofacial surgeon. Techniques for needle localization and removal have been described, including reports of cases using 3D navigation and/or intra-operative fluoroscopy for fragment location.
We present a case where a 30 gauge, 25 mm needle was fractured during administration of a right inferior alveolar nerve block and became displaced adjacent the right carotid sheath.
Furthermore, we present our definitive management, involving the use of StealthStation® Navigation System (Medtronic 710 Medtronic Parkway Minneapolis, Minnesota 55432-5604 USA) and intra-operative fluoroscopy.
Case Report
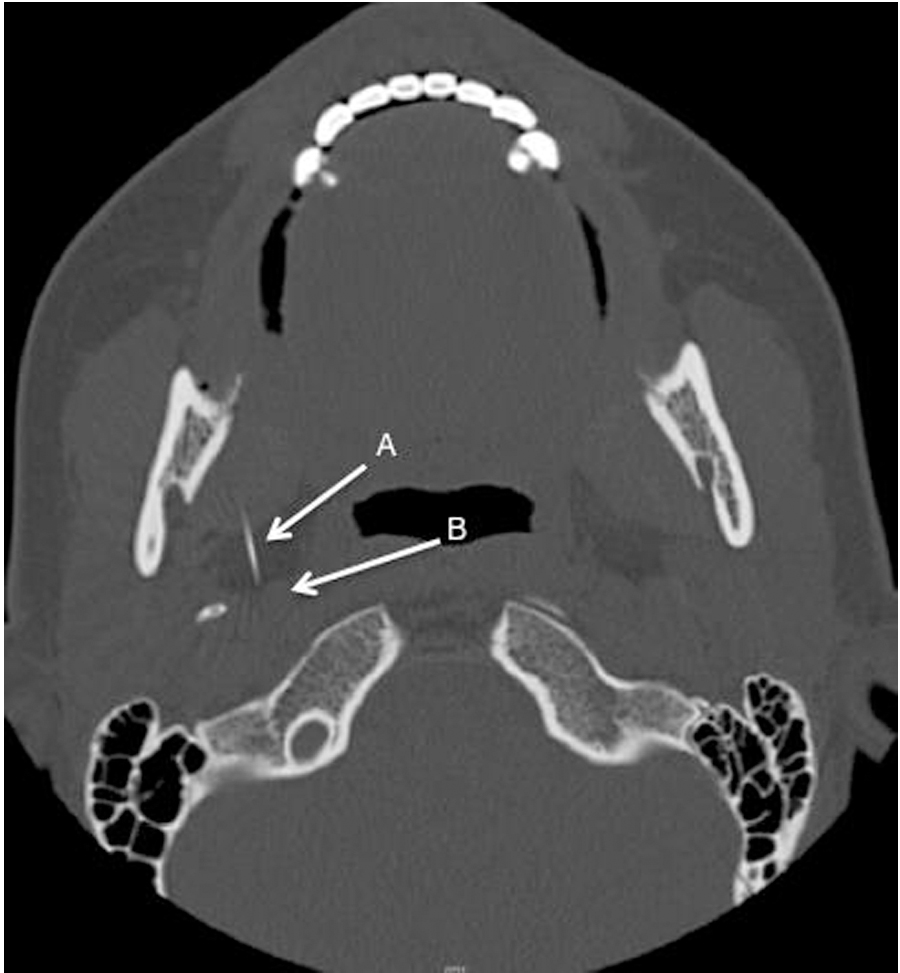
An 18-year-old female was referred to University Hospital, London Health Sciences Centre in London, Ontario, for an irretrievable needle fracture following the administration of an inferior alveolar nerve block. The patient had undergone general anesthesia for the extraction of her third molars, and upon administration of local anesthesia to the right mandible via inferior alveolar nerve block technique, the needle broke off at the level of the tissue. The armamentarium used was a 30 gauge, 25 mm needle and it was not bent prior to insertion; however, it was inserted to the hub, where it fractured. Once fractured, the needle was not visible or palpable. After a brief attempt at retrieval, imaging was completed (Figs. 1 & 2). Plain film and CT revealed the needle fragment was in the right parapharyngeal space on the medial aspect of the right mandibular ramus and the tip was in close proximity of the carotid sheath. The patient was then sent to the Oral and Maxillofacial Surgery Department at University Hospital, London Health Sciences Centre.
FIGURE 1. Lateral oblique view of the mandible exhibits displaced needle fragment. Arrow indicates needle fragment.

FIGURE 2. Computed Tomography, axial view. Needle fragment (A), shown in close proximity to carotid sheath (B).
On history and physical examination, the patient was an otherwise healthy 18-year-old female. There was bilateral edema within normal limits of her third molar extraction procedure. No clinical evidence of the fractured needle fragment was visualized, nor was it palpable. The patient was admitted to the hospital, and the neurosurgery service was consulted, specifically a neurointerventionalist, due to the proximity of the needle to the carotid sheath. A cervical collar was placed on the patient to stabilize the neck. The patient was then consented for the retrieval of the needle fragment under general anesthesia.
The pre-surgical plan was to use an intra-oral approach, guided by the StealthStation® Navigation System to remove the fractured needle fragment. In the event the navigation system alone failed to locate the needle, the plan was to use complementary intra-operative fluoroscopy. Pre-operatively, CT angiography (Fig. 3) was completed for surgical planning and to achieve synchrony with StealthStation® Navigation System.
FIGURE 3. Computed tomography angiogram, coronal section. A. Needle fragment B. Internal carotid artery C. Mandibular condylar head. D. Vertebral column.

The patient was taken to the operating room, anesthetized and placed on a Mayfield headrest. Fiducial markers were placed on the patient’s cranium and used as a point of anatomical reference. Anatomy was then confirmed using the SteathStation® Navigation System registered to the pre-operative CT angiogram. The 3D location of the needle fragment was identified. Transmucosal incision in the right retromolar region was carried out at the level of the coronoid, followed by blunt dissection in the supraperiosteal plane. Consistent verification of our clinical position relative to the fragment via the navigation system was performed. Fiber by fiber dissection through the body of the medial pterygoid continued for about three hours, unsuccessfully. The SteathStation® had its limitation secondary to the lack of real time application; the dissection was being guided by a pre-operative CT, not accounting for any soft tissue movement or alternative positioning of the patient. Since there was a lack of surgical progress, the decision was made to bring in real time imaging with intra-operative fluoroscopy (Fig. 4). This allowed for confirmation and triangulation to locate the fragment. Successful retrieval was achieved, and the 30 gauge, 25 mm needle was removed (Fig. 5). Additionally, fluoroscopy images were taken to confirm the complete removal of the foreign object. The lingual nerve was visualized and protected during the procedure; moreover, the carotid artery was not perforated. The patient tolerated the procedure well, her post-operative stay was uneventful, and she was discharged home the following day. Immediately post-operative cranial nerve V (lingual nerve) paresthesiae were noted. At the six-month follow-up, the
patient was doing well, and she reported her CNV paraesthesiae had resolved completely.
FIGURE 4. Intra-operative fluoroscopy image. A. Needle fragment B. Endotracheal tube C. Side-action mouth prop.

FIGURE 5. Needle fragment retrieved from the patients lateral parapharyngeal space. It should be noted the needle was bent at the time of retrieval.

Discussion
Despite advancements in needle materials, fractures are still reported. It has been roughly estimated that needle fractures occur at an incidence of 1/14000000 per year.1 This is thought to be a relatively rare event secondary to improved stainless steel alloys, one-time use needles, and careful, improved anesthetic techniques. The risk of leaving the needle in situ usually outweighs the risk of removal, when in proximity to vital structures, for migration and damage to vital structures can occur. Therefore, needle retrieval is indicated, and remains a challenge for the oral and maxillofacial surgeon. Intraoperative navigation systems, originally developed for complex neurosurgical procedures, have been described in oral and maxillofacial surgery for the removal of needle fragments and can provide improved accuracy during retrieval.3 While this 3D technology can aid in bridging the gap between pre-operative imaging and anatomical structures encountered during fragment removal, there are some limitations as illustrated in the case presented. The soft tissues that the needle fragment is embedded in are not static, and therefore, can move during the operation, which is not accounted for in the navigation system. This yields limited use for navigation systems in mobile soft tissue.3 Fluoroscopy has the benefit of intra-operative real time imaging, particularly the technique of triangulation, where perpendicular images are shot using a known point as a reference, in comparison to the unknown location of the foreign body. Limitations with 3D navigation were encountered in this case, and intra-operative fluoroscopy was implemented to obtain precise location of the needle fragment in real time. The use of both the SteathStation® Navigation System and fluoroscopy provided improved precision, accuracy and allowed for enhanced intra-operative landmarking. The results were a minimally invasive, intra-oral access and intact vital structures. The alternative treatment would have been a transcervical approach to the foreign body with exposure of the carotid sheath by the neurosurgery team.
Ultimately, prevention is the best treatment. Recommendations to avoid needle fractures have been well documented in the literature1-4 and include:
o Avoid 30 gauge needles for IAN blocks.
o Avoid bending the needle.
o Avoid inserting the needle to the hub.
o Avoid using a short needles for an IAN block (likely to go to hub).
o Avoid repositioning techniques which cause strain and bending of the needle.
o Communicate well with patients, particular children, to avoid sudden movements.
o Should fracture occur, and it is visible, retrieval with fine hemostats may be attempted. However, if it is not visible, place pt on ABx, take imaging if possible and refer the patient to an oral and maxillofacial surgeon.1,2
Conclusion
Needle retrieval secondary to fracture at the time of anesthetic administration remains a challenge for the oral and maxillofacial surgeon. Prevention is best, with recommendations to avoid needle breakage described in our discussion. Unfortunately, needle fracture and displacement can still occur, warranting removal of the foreign body. Surgical removal should be attempted under direct, guided visualization for achieving minimally invasive surgery. Inferior alveolar anesthetic injections are routine and complacency in technique leads to surgical misadventure. Periodic review of even the most elementary procedures is time well spent.OH
Jacqueline Cox, Oral and Maxillofacial Surgery Resident, Schulich School of Medicine and Dentistry, Western University and Department of Oral and Maxillofacial Surgery, London Health Sciences Centre, London, Ontario. E-mail: jacqueline.cox@londonhospitals.ca.
Jerrold E. Armstrong, Associate Professor, Schulich School of Medicine and Dentistry, Western University and Chief of Dentistry, London Health Sciences Centre, London, Ontario.
Stephen Lownie, Professor, Departments of Clinical Neurological Sciences (Neurosurgery), Medical Imaging (Neuroradiology) and Otolaryngology, Schulich School of Medicine and
Dentistry, Western University and London Health Sciences Centre University Hospital, London Health Sciences Centre. 339 Windermere Road P. O. Box 5339, London, ON Canada
N6A A5A. Tel: 519-663-3451. Fax: 519-663-3004.
Oral Health welcomes this original article.
References:
1. Pogrel MA. Broken local anesthetic needles: a case series of 16 patients, with recommendations. Journal of the American Dental Association. 2009;140(12):1517-22.
2. Ethunandan M, Tran AL, Anand R, Bowden J, Seal MT, Brennan PA. Needle breakage following inferior alveolar nerve block: implications and management. British Dental Journal. 2007;202(7):395-7.
3. Gerbino G, Zavattero E, Berrone M, Berrone S. Management of needle breakage using intraoperative navigation following inferior alveolar nerve block. Journal of oral and maxillofacial surgery: Official Journal of the American Association of Oral and Maxillofacial Surgeons. 2013;71(11):1819-24.
4. Thompson M, Wright S, Cheng LH, Starr D. Locating broken dental needles. International Journal of Oral and Maxillofacial Surgery. 2003;32(6):642-
Follow the Oral Health Group on Facebook, Instagram, Twitter and LinkedIn for the latest updates on news, clinical articles, practice management and more!











