
Many psychotropic drugs cause dry mouth, most commonly due to anticholinergic effects. Xerostomia a common issue in dental practice, affecting about 1 in 4-5 adults.1 It can cause a range of signs and symptoms, from a mild sensation of dryness and stickiness to more serious effects such as difficulties with chewing, swallowing, and speaking.2 If prolonged, xerostomia can lead to tooth decay, periodontal disease, and tooth loss, as well as an increased risk of mouth sores, recurrent oral candidiasis and angular cheilitis. Dentures can be uncomfortable or impossible to wear, as well as cause painful mouth sores by rubbing against the gums.3
Xerostomia is associated with many medical conditions, radiation therapy for head and neck cancers, and medications. Many psychotropic drugs cause dry mouth as a side effect (see Table 1). These medications are used not just for mental health conditions (such as depression, anxiety, schizophrenia, bipolar affective disorder, and attention deficit hyperactivity disorder (ADHD)) but also for non-psychiatric reasons such as neuropathic pain, insomnia, and migraine prophylaxis.
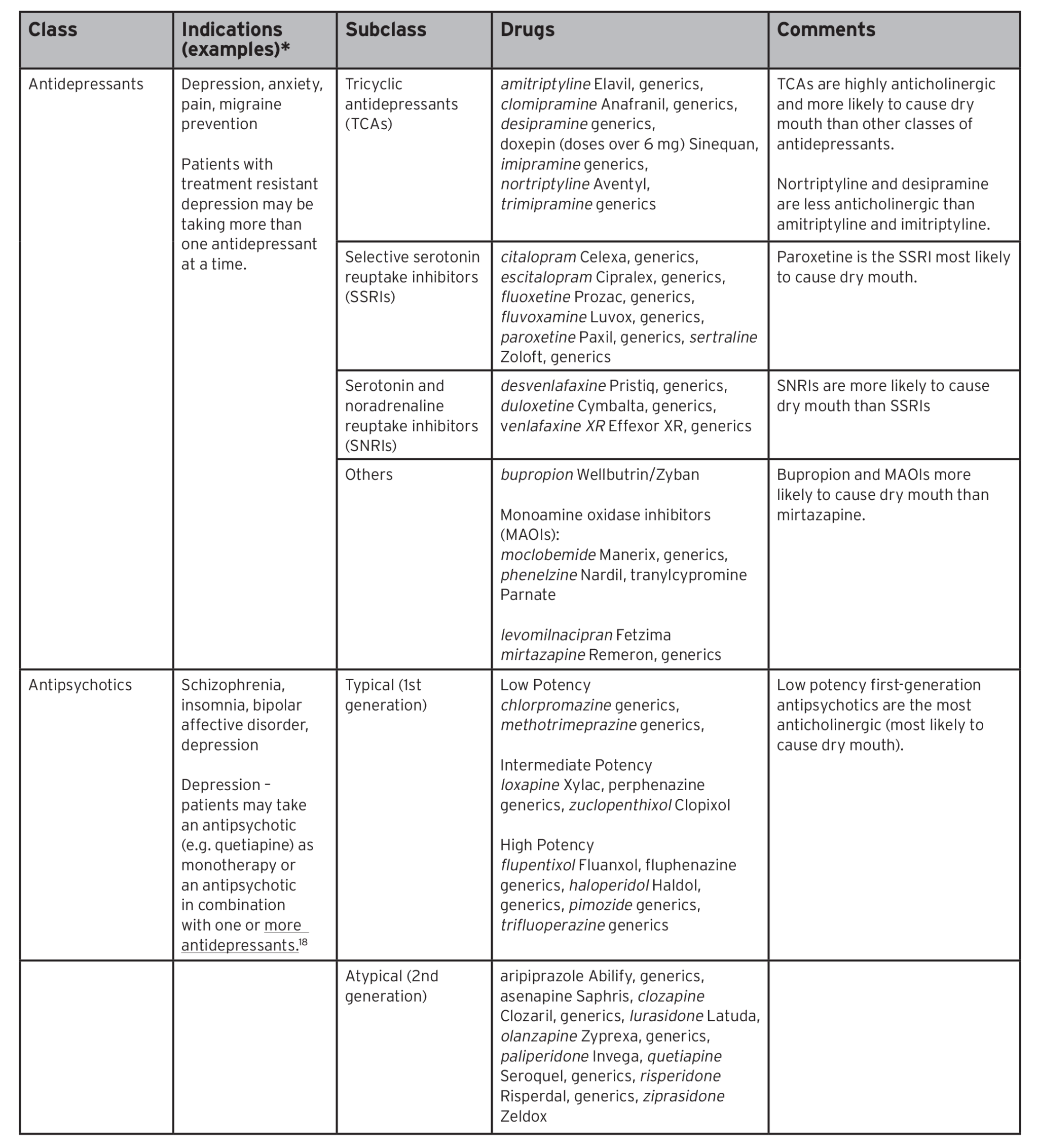
Table 1: Psychotropic drugs with dry mouth as a side effect1,16,18,19,20,21,22,23,24,25, 26,28


Saliva production is controlled by the autonomic nervous system (ANS). Parasympathetic nerves release acetylcholine, leading to the production of copious amounts of watery saliva. Sympathetic activation of salivary glands also produces saliva, but in smaller amounts and more viscous in quality. The parasympathetic division tends to predominate under resting conditions. When stressed or anxious, the sympathetic nervous system predominates, leading to a change in the composition of saliva, leading to the sensation of dry mouth. Drugs with sympathomimetic activity act in the same way (e.g. amphetamine-like drugs for ADHD and bupropion used for depression or smoking cessation).
However, most psychotropic drugs cause dry mouth by interfering with the parasympathetic nervous system. Antimuscarinic drugs bind to, and block, muscarinic cholinergic receptors in the salivary glands, leading to reduced saliva output and dry mouth. Other anticholinergic side effects include dry eyes, dry skin, flushing, urinary retention, constipation, blurred vision, photophobia, dizziness and cognitive impairment.
Dry mouth is one of the first anticholinergic side effects to occur, along with dry eyes and dry skin. Unfortunately, anticholinergic symptoms do not go away with time. The frequency and severity of dry mouth depends on the anticholinergic activity of the specific drug, the dose, and the number of drugs being taken. Hundreds of drugs have anticholinergic side effects. Among the most highly anticholinergic are tricyclic antidepressants, drugs for overactive bladder, and first-generation antihistamines.
There are various scales which can help to quantify the “anticholinergic burden,” such as the Anticholinergic Drug Scale, the Anticholinergic Cognitive Burden Scale, and the Anticholinergic Risk Scale.4 There is also an online calculator, which can be found at abcbcalc.com. Another useful resource can be found at rxfiles.ca/rxfiles/uploads/documents/Psyc-anticholinergic-Ref%20List%20SPDP-complete.pdf).5
While drug-induced dry mouth can occur at any age, it most commonly affects the elderly. Compared to younger people, they tend to take multiple medications, have more medical conditions (some of which can be associated with dry mouth, such as diabetes), have decreased drug metabolizing ability, and possibly age-related salivary hypofunction,6,7 all of which can contribute to dry mouth.
Older people are also more likely to experience the more severe, potentially dangerous effects secondary to anticholinergic medications. Preexisting cognitive issues, such as Alzheimer’s disease and Lewy body dementia, make the elderly even more sensitive to anticholinergic-induced confusion, memory impairment, and delirium. Dizziness and blurred vision can increase the risk of falls.
Dentists might be the first health care professionals to detect signs of anticholinergic toxicity, especially since, because of COVID, many patients have put off seeing their physician. Signs of toxicity which may require urgent medical referral include:5
- Dilated pupils causing blurred vision (which can increase the risk of falls and accidents)
- Decreased sweating which can lead to heat stroke and heat exhaustion in hot environments (risk is increased if also taking a diuretic)
- Constipation
- Urinary retention (and worsening of benign prostatic hyperplasia (BPH))
- Increased heart rate (over 100 bpm)
- Restlessness, disorientation, agitation
- Confusion, memory impairment
- Worsened cognition in patients with dementia
- Ataxia, muscle twitching, hyperreflexia, seizures
- Hypertension or hypotension
- Excessive sedation
Perform a comprehensive medication assessment at each appointment
Patients should be asked at every appointment about dry mouth. In addition to an oral exam, the patient can be asked a few questions to help with the diagnosis:8
- Does your mouth usually feel dry?
- Does your mouth feel dry when eating a meal?
- Do you have difficulty swallowing dry foods?
- Do you need to sip liquids to swallow dry food?
- Is the amount of saliva in your mouth inadequate most of the time?
Patients may have a dry mouth but are not bothered by it. They might not realize it can cause problems, so this is an important education point. Other patients have no sensation of dry mouth, and it is the dentist who diagnoses the consequences such as caries, missing teeth or periodontal disease.
At each visit, the dentist should also collect information about prescriptions, including doses, directions, indications, and duration of use. If the regimen is complex, or the patient has trouble remembering what they are taking, a list can be requested from the patient’s pharmacy.
Include over-the-counter (OTC) drugs when gathering information. Drugs for cough, cold, allergy, sleep, nausea, diarrhea, and muscle pain are common causes of dry mouth. Often, these drugs come in various combinations with each other and/or with other ingredients, all with similar brand names. Try to find out the exact brand name of the product they are using, then either check with a pharmacist or look it up on Health Canada’s Drug Product Database to find its ingredients (canada.ca/en/health-canada/services/drugs-health-products/drug-products/drug-product-database.html).
Review each medication with the patient and ask if and how they are taking it. Patients might have stopped taking their medication if dry mouth or other side effects became too bothersome. If they report dry mouth, ask the patient if they can identify the drug(s) they think could be the cause. They might have noticed dry mouth starting after a change was made. Anticholinergic-induced dry mouth tends to develop quickly after starting a new drug or increasing the dose.
Also, ask about recreational drug use, including alcohol, tobacco, e-cigarettes (vaping), cannabis and caffeine, as these can contribute to dry mouth. Other drugs associated with dry mouth include MDMA (ecstasy), cocaine, and methamphetamine.9,10
Once a list is created, check to see if the patient is taking any medications that could be causing dry mouth. A pharmacist can help with this. While Table 1 focuses on psychotropic medications, the drugs below are examples of other drugs reported to cause dry mouth in more than 10% of patients:1,5
Anticholinergics
e.g. atropine, glycopyrrolate, scopolamine
Drugs for overactive bladder
e.g. darifenacin, fesoterodine, flavoxate, oxybutynin, solifenacin, tolterodine, trospium.
Opioids
e.g. codeine, meperidine, tramadol
Skeletal Muscle relaxants
e.g. baclofen, cyclobenzaprine, methocarbamol, orphenadrine, tizanidine
Drugs for gastrointestinal conditions
e.g. dimenhydrinate (Gravol), loperamide, (Imodium), nabilone, prochlorperazine, ranitidine (Zantac)
Decongestants
e.g. pseudoephedrine
Antihypertensives
e.g. alpha blockers, beta blockers, calcium channel blockers, diuretics, ACE inhibitors
Antiarrythmics
-disopyramide, propafenone
Biologic response modulators
e.g. interferon alfa-2a, interferon alfa-2b
Ergot alkaloids
e.g. ergotamine
NSAIDs
Retinoic acid derivatives
e.g. isotretinoin
Avoid adding a drug to treat dry mouth
Pilocarpine is a cholinergic agonist which has shown benefits in alleviating anticholinergic-induced dry mouth in patients with functioning salivary glands. It is approved for use in patients with Sjögren’s syndrome or radiotherapy-induced xerostomia. Yet there is a lack of evidence supporting its effectiveness in treating dry mouth associated with psychiatric medication (9). Pilocarpine also has side effects, such as sweating, nausea, diarrhea, palpitations and urinary urgency, which in turn might require drug treatment. In general, it is recommended to avoid adding a drug to treat the side effect of another unless absolutely necessary because it can lead to a prescribing cascade and contribute to the perils of polypharmacy.11
Identify opportunities to target the root cause
Instead of adding a medication, it is best to try to reduce or eliminate the patient’s exposure to a drug causing dry mouth. Consider whether it can be stopped, decreased or changed as described below.
Stopping the drug
Many drugs are continued for longer than needed and should be reviewed at least annually. Stopping might be possible if the drug is no longer required or if the condition can be adequately managed without medication. Antipsychotics such as quetiapine (prescribed off-label to help with sleep) can cause dry mouth even at the low doses used for insomnia (25-200 mg) as well as the higher doses used to treat schizophrenia (600 mg-1,000 mg).12 Because of this and other adverse effects (such as metabolic syndrome), guidelines suggest avoiding quetiapine as a first-line treatment for insomnia. There are safer alternatives, such as practicing good sleep hygiene and interventions such as cognitive behavioural therapy for insomnia (CBT-i).13
The Canadian Deprescribing Network has resources for both patients and prescribers about potentially inappropriate drugs and how to discontinue them safely. (deprescribingnetwork.ca).14 If the patient and prescriber decide to stop a medication, the dose may need to be
tapered downwards over a period of time to avoid withdrawal reactions such as cholinergic rebound (e.g. sweating, nausea, increased urinary frequency, insomnia).
If multiple drugs are candidates for deprescribing, tools such as medstopper.com can help physicians choose which one to target first.15
Decreasing the dose
If stopping a drug is not an option, the dose might be able to be decreased to resolve dry mouth. Sometimes, drug doses are tapered up too quickly when they would have been just as effective at a lower dose. Antidepressant doses can sometimes be increased before enough time has passed to assess their effectiveness.
The dose of a drug might also be too high after adding a second agent that impairs its metabolism. As well, as people get older, they may need lower doses of their chronic medications because of age-related changes to kidney and liver function and because older people can be more sensitive to the drug’s effect. A patient may have tolerated a certain dose but find as they age that dry mouth starts to be a problem.
Other dose changes that may help reduce dry mouth include dividing a once-daily dose into smaller amounts taken more frequently. And if dry mouth is bothersome at night, it might help to give the dose in the morning.16
Switching the drug
The third option is to consider whether there is an equally effective drug with less risk of dry mouth. Fortunately, within each class of psychotropic medication, there are often drugs less likely to cause dry mouth (see Table 1). Switching to a different drug within the same class could be an option. Paroxetine, an SSRI used for depression, is more likely than other drugs in the same class to cause dry mouth.5 Switching should always be done cautiously, monitoring the patient closely for worsening of their condition or development of adverse effects. The Canadian website switchrx.com (registration required) can provide information about how to make the change safely.17
Educate patients about dry mouth: its causes, consequences and management
If one or more medications have been identified as possibly causing or contributing to dry mouth, provide this information to the patient so that they can discuss it with their physician. Be sure to tell them not to make changes independently without first speaking with their prescriber.
Provide patients with advice and/or referrals to community supports if they are looking for information or assistance with nicotine dependence, or reducing/stopping cannabis, alcohol, or other substances.
Advise patients to speak with their pharmacist before taking over-the-counter medications or natural health products. The pharmacist can review the ingredient(s) to see whether dry mouth could be a side effect.
Make sure patients know that even if they are not experiencing a sensation of dry mouth, drugs can still contribute to problems in the future, such as caries and gum disease. Encourage patients to visit the dentist every 3 to 6 months for regular assessment and preventative care. Consider applying a topical fluoride product at their appointments. Ideally, patients should also visit the dentist before starting a new medication which has the potential to cause dry mouth, to get a baseline assessment.
Finally, instruction on excellent oral hygiene is important. Also, provide patients with self-management tips to prevent and manage dry mouth, such as those in Table 2. Ideally, follow up with patients a week or so after each visit to see if they have any questions and to ask whether they have noticed an improvement of dry mouth symptoms.
Table 2: Advice for managing dry mouth3,27

Oral Health welcomes this original article.
References
- Kletas, V. Dry Mouth. In: Compendium of Therapeutics for Minor Ailments [Internet]. Ottawa (ON): Canadian Pharmacists Association; updated Nov 2020; cited 2021 Aug 25. Available from: http://www.myrxtx.ca. Also available in paper copy from the publisher.
- Daly C. (2016). Oral and dental effects of antidepressants. Australian prescriber, 39(3): 84. https://doi.org/10.18773/austprescr.2016.035
- Tappuni, A.R., Wilson N. (2018). Dry mouth: advice and management. The Pharmaceutical Journal, 300(7911). https://doi.org/10.1211/PJ.2018.20204481
- Salahudeen, M. S., Duffull, S. B., & Nishtala, P. S. (2015). Anticholinergic burden quantified by anticholinergic risk scales and adverse outcomes in older people: a systematic review. BMC Geriatrics, 15(1), 31–31. https://doi.org/10.1186/s12877-015-0029-9
- “Anticholinergics: Reference List of Drugs with Potential Anticholinergic Effects,” published by RxFiles (https://www.rxfiles.ca/rxfiles/uploads/documents/Psyc-anticholinergic-Ref%20List%20SPDP-complete.pdf).
- Patel, P. S., Ghezzi, E. M., Ship, J. A. (2001). Xerostomic complaints induced by an anti-sialogogue in healthy young vs. older adults. Special Care in Dentistry, 21(5):176–181. https://doi.org/10.1111/j.1754-4505.2001.tb00251.x
- Tan, E. C., Lexomboon, D., Sandborgh‐Englund, G., Haasum, Y., & Johnell, K. (2017). Medications that cause dry mouth as an adverse effect in older people: A systematic review and metaanalysis. Journal of the American Geriatrics Society, 66(1): 76-84. https://doi.org/10.1111/jgs.15151
- Goldstep F. (2011). Dry mouth: Simplified. Oral Health Group. Retrieved August 25, 2021, from https://www.oralhealthgroup.com/features/dry-mouth-simplified/
- Taylor, D.M., et al. (2020). The Maudsley Practice Guidelines for Physical Health Conditions in Psychiatry. John Wiley & Sons, Incorporated.
- Methamphetamine. American Dental Association. (2021). Retrieved August 25, 2021, from https://www.ada.org/resources/research/science-and-research-institute/oral-health-topics/methamphetamine
- Canadian Pharmacists Association. (2020). Pharmacist: Six Tests and Treatments to Question. Retrieved August 25, 2021, from https://choosingwiselycanada.org/recommendation/pharmacist/
- Coe, H. V., & Hong, I. S. (2012). Safety of low doses of quetiapine when used for insomnia. 46(5): 718–722. https://doi.org/10.1345/aph.1q697
- Canadian Pharmacists Association. (2020). Pharmacist: Six Tests and Treatments to Question. Retrieved August 25, 2021, from https://choosingwiselycanada.org/recommendation/pharmacist/
- Canadian Deprescribing Network. Do I still need this medication? Retrieved August 25, 2021, from
https://www.deprescribingnetwork.ca - University of British Columbia. Medstopper Beta. Retrieved August 25, 2021, from: medstopper.com
- American Dental Association. (2021). Xerostomia (Dry Mouth). Retrieved August 25, 2021, from https://www.ada.org/resources/research/science-and-research-institute/oral-health-topics/xerostomia
- SwitchRx: The Online Medication Switching Tool. Retrieved August 25, 2021, from: switchrx.com
- Waite, R. (2014). Use of second generation antipsychotics for treatment-resistant major depressive disorder. Mental Health Clinician, 4(5): 246–256. doi: https://doi.org/10.9740/mhc.n207192
- Cappetta, K., Beyer, C.E., Johnson, J.A., & Bloch, M.H. (2018). Meta-analysis: Risk of dry mouth with second generation antidepressants. Progress in Neuro-Psychopharmacology and Biological Psychiatry, 84, 282-293.
- ABIM Foundation (2018). Choosing Wisely: Sleeping pills for insomnia and anxiety in older people. Retrieved August 25, 2021, from https://www.choosingwisely.org/patient-resources/treating-insomnia-and-anxiety-in-older-people/?highlight=%22dry+mouth%22
- Busto U.E., Sproule B.A., Knight K., Herrmann N. (2001). Use of prescription and nonprescription hypnotics in a Canadian elderly population. Can J Clin Pharmacol 8(4): 213–221.
- Hunter K.D., Wilson W.S. (1995). The effects of antidepressant drugs on salivary flow and content of sodium and potassium ions in human parotid saliva. Arch Oral Biol. 40:983-9. http://dx.doi.org/10.1016/0003-9969(95)00079-5
- Rudolph J.L., Salow M.J., Angelini M.C., McGlinchey R.E. (2008). The Anticholinergic Risk Scale and Anticholinergic Adverse Effects in Older Persons. Arch Intern Med. 168(5):508–513. http://doi.org/10.1001/archinternmed.
2007.106 - Franck, H., Potter, J. Caballero, J. (2013). Venlafaxine and duloxetine: A comparison of efficacy and tolerability for the treatment of depression in elderly patients. Mental Health Clinician. 3 (5): 258–265. https://doi.org/10.9740/mhc.n178920
- Baltenberger E.P., Buterbaugh W.M., Martin B.S., Thomas C.J. (2015). Review of antidepressants in the treatment of neuropathic pain. Mental Health Clinician. 5 (3): 123–133. https://doi.org/10.9740/mhc.2015.05.123
- Ross C. (2014). Levomilnacipran (Fetzima™) for the treatment of major depressive disorder. I. 4 (1): 27–30. https://doi.org/10.9740/mhc.n186963
- Tips to Deal with Anticholinergic Side-Effects RxFiles. Saskatoon, SK. 2020. https://www.rxfiles.ca/rxfiles/uploads/documents/Psyc-anticholinergic-Ref%20List%20SPDP-complete.pdf
- Gormley, L., Turner, A., Freeland, K. (2014). Clonidine and guanfacine IR vs ER: Old drugs with “new” formulations. Mental Health Clinician 4 (1): 22–26. doi: https://doi.org/10.9740/mhc.n186955
About the Author
 Caroline Warnock has worked as a pharmacist at the Centre for Addiction and Mental in Toronto for over 20 years. She is currently the Medication Safety Pharmacist and she also provides clinical coverage on an inpatient unit. She has a Doctor of Pharmacy degree from the University of Colorado and a Postgraduate Certificate in Psychiatric Pharmacy from Aston University in the UK.
Caroline Warnock has worked as a pharmacist at the Centre for Addiction and Mental in Toronto for over 20 years. She is currently the Medication Safety Pharmacist and she also provides clinical coverage on an inpatient unit. She has a Doctor of Pharmacy degree from the University of Colorado and a Postgraduate Certificate in Psychiatric Pharmacy from Aston University in the UK.










