
For the last six years, I have been successfully using Biodentine® Dentine Replacement Material (by Septodont®) for direct and indirect pulp caps. I have developed some insights and techniques on its use that I believe would be helpful for my peers. In an effort to share and build on my experiences I am presenting this article. I am not a researcher or professor. My laboratory has been my busy 28-year-old dental practice.
Background on Tricalcium Silicate (TS)
The release of calcium hydroxide is so important to the understanding of why tricalcium silicates work. Dentists are familiar with ProRoot ®MTA by Tulsa Dental, which was the first available form of tricalcium silicate (TS). MTA was introduced in 1993 by Dr. Torabinejad.
MTA is a powder consisting of tricalcium silicate, tricalcium aluminate, tricalcium oxide and silicate oxide. It also contains small amounts of other mineral oxides, which may modify its chemical and physical properties. Bismuth oxide is added to make the material radiopaque.
Biodentine is an engineered form of TS; it lacks some of the trace elements and has improved physical properties. With that being said, in my personal opinion, I am not sure that it makes any difference to its efficacy on pulp caps. I think of TS as a way of delivering calcium hydroxide to the pulp that is superior to Dycal®, Life™, Ultracal® and TheraCal LC®.
There is over 90 years of research on the effects of calcium hydroxide on the pulp. We know that the presence of resin or glass ionomer on pulpal tissue causes an inflammatory response. We know that calcium hydroxide can heal pulpal tissues. The reasons that I believe that TS is superior to other forms of calcium hydroxide are:
1) It is hydrophillic
2) It is highly alkaline (bacteriostatic)
It has low marginal leakage (forms a physiochemical bond to dentin)
It has low solubility
It has high biocompatibility
![]()
My Clinical History with Biodentine
When I first received Biodentine as a sample in 2009, I used it as directed by the manufacturer. For the first two years, I would place the Biodentine and wait 12 minutes or longer for the material to set prior to carving. I got great results both on direct and indirect pulp caps. As long as the teeth were asymptomatic, having normal cold and normal percussion test, these teeth would maintain vitality with little or no sensitivity. These cases, some of which are over five years old, would certainly have ended up as root canals in my practice, prior to my using Biodentine (Figs. 1a,1b,1c,1d).
Although Biodentine sets much faster than MTA, it was still longer than most practitioners, including me, were willing to wait before carving. I then started filling half of the prep with Biodentine and filling the rest of the prep with glass ionomer. My technique evolved into pushing the Biodentine into the prep with a cotton pellet and wiping excess Biodentine away from exposed margins; then I would fill the remainder of the prep with glass ionomer. This technique eliminated delicate carving of marginal ridges, some fractured marginal ridges and open contacts. As this was a temporary restoration, these problems could have been addressed at a later appointment. However, the use of glass ionomer over Biodentine improved my temporary restoration, making it a more ideal and predictable restoration.
FIGURE 1A. Caries removed showing the exposed pulp.

FIGURE 1B. Pre-optive radiograpgh prior to caries removal.
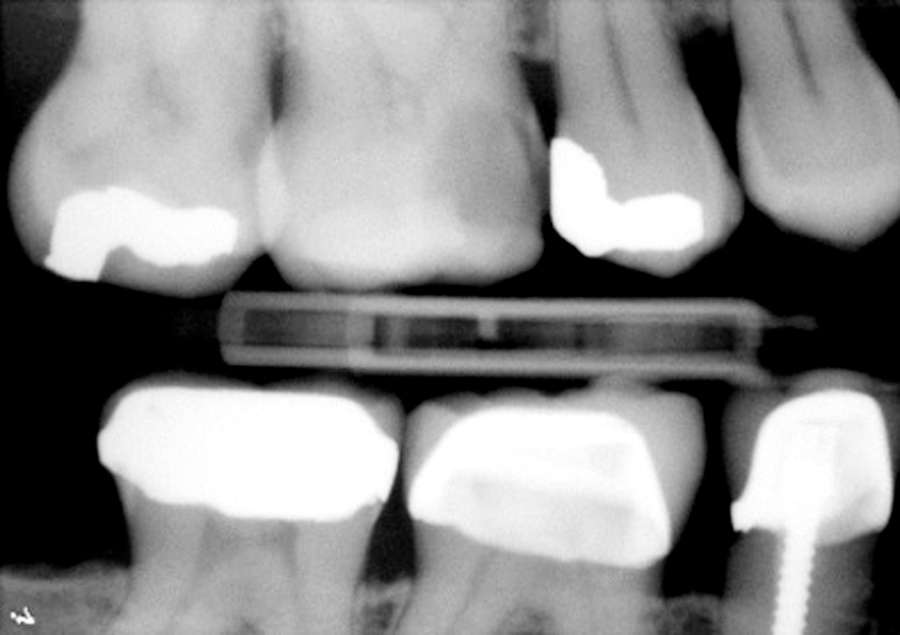
FIGURE 1C. Radiograph after placement of Biodentine.

FIGURE 1D. Tooth with Interim Biodentine restoration.

In the case of direct pulp caps, I would always do an interim restoration and wait two to four weeks. I waited the two to four weeks not because I wasn’t sure the Biodentine would work, but to be prudent and to emphasize to the patient that I just saved the tooth from a root canal (Figs. 2a, 2b, 2c).
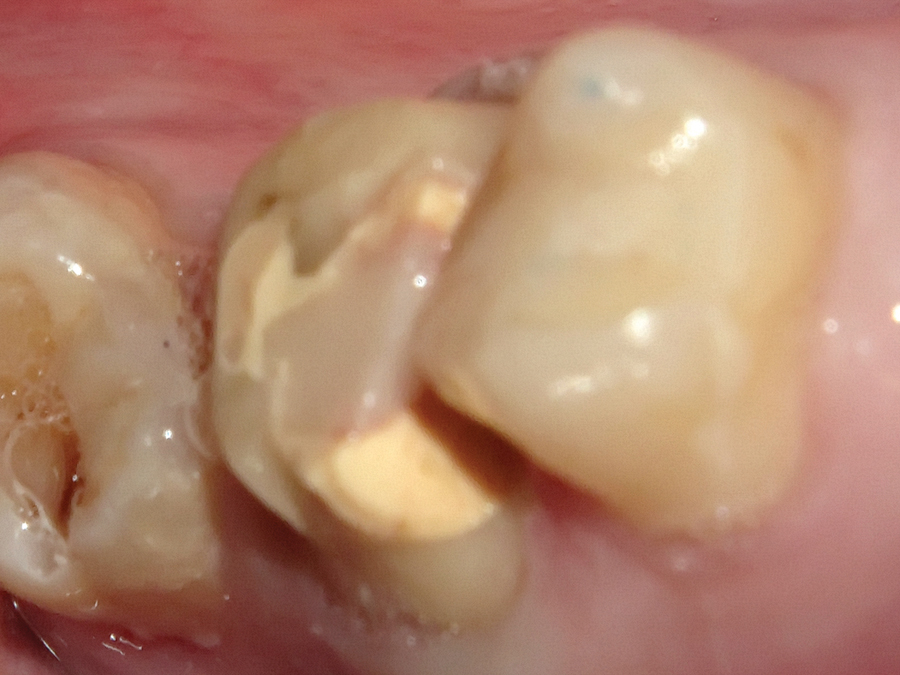
FIGURE 2A. Hybird glass ionomer/Biodentine restoration.

FIGURE 2B. Hybird glass ionomer/Biodentine preparation for a crown. Note the bond between Biodentine and the glass ionomer base.
I use a similar technique with indirect pulp caps. I open a capsule of Biodentine and mix a small amount of the powder with a small amount of the liquid. This mixture is applied with a Dycal instrument. Then, as above, a cotton pellet is used to dry the excess. Instead of glass ionomer I use a self-etching flowable by Kerr (Vertise™Flow) over the top of the Biodentine and light cure. I then proceed normally to my final restoration (Fig. 3).
FIGURE 3. Biodentine is used like Dycal on an indirect pulp cap.

As with any technique one would expect failures. I have had a small percentage of failures. Patients with a history of pain that tested normal for cold and percussion tended to fail whether it was direct or indirect exposure of the nerve. There was one failure on a bicuspid where I was able to save the nerve but I didn’t have adequate tooth structure for a restoration. This case ended up with an intentional endo/post/build up (Figs. 4a, 4b).
FIGURE 4A. Extensive decay which required intentional endodontics to place post and build-up.

FIGURE 4B. Biodentine build-up shows the success of saving the nerve.

In another case, there was a history of pain and the patient wanted an extraction due to finances. I placed Biodentine and was able to keep the patient out of pain for a year. She was then in a better financial position and was able to have the root canal/crown. In the six year of placing Biodentine as a base/liner, I have had less than ten failures from hundreds of cases. Case selection has been the biggest factor with respect to avoiding failures.
Tricalcium Silicate Use in Endodontics
MTA has been used extensively by endodontists since the early 90s. Its ability to seal and repair damaged root surfaces has been its main use. I know of one endodontist who uses MTA to fill canals on his retreats. The main fear of using TS alone for obturation is that in the event of failure, retreatment would be impossible.
Let’s discuss the reasons for failure with root canals and sealers. Here are some of the normal reasons for failure:
1. Missed canals
2. Branched (lateral) canals
3. Deterioration of seal
4. Inadequate or leaking final restoration
5. Cracked tooth
I have been using BioRoot™ RCS (root canal sealer) by Septodont for a little over a year. It is pure TS, which has been formulated to be used with gutta percha. I will try to make a case for using a TS based sealer over other types of sealers:
1. BioRoot RCS is truly hydrophilic. I rinse the canal with ethanol and use many paper points. Does anyone really believe that we can totally dry the canal? Will a resin-based sealer really get into any accessory canals? TS is water seeking. It needs water to set.
2. Retreatment when used with gutta percha is possible. It is probably more difficult. However, a missed canal could still be treated easily (once identified) since no TS is in the canal.
3. Branched canals would probably be difficult, if not impossible, to treat even in a retreatment scenario. I would think that if a tooth was cleaned well, you would have a better chance of getting TS into those impossible accessory canals.
4. Lack of deterioration of the seal is probably TS’ best asset. It also is the one aspect that keeps endodontists from using it. Should we always be thinking that retreatment is inevitable? Or should we try to achieve the best possible seal with the best possible material?
5. TS resists recontamination of the canal system from failing restorations. TS’ antibacterial properties come into play when it sets, releasing calcium hydroxide; after setting, it is bacteriostatic, because of its alkalinity.
6. Cracked teeth–This may be a stretch, but there is some evidence that TS may strengthen the root through a physiochemical bond to the dentinal tubules. There are many factors that contribute to root fracture, making retreatment impossible.
Within the first year of using BioRoot RCS, I have not had any failures. With that being said, I know that it takes years to really know the efficacy of the seal and even then, there is always doubt. My dad used to say that if you cleaned a tooth well, you could fill it with “sterilized bird S*#!”. I hopefully have made a case for using a TS sealer over bird poop, or other sealers for that matter.
Discussion
I use some form of TS in my practice if not daily, at least weekly. I use TS in lieu of Dycal routinely now, and do pulp caps on teeth that I used to think were destined for endo. All of my endo is done with a TS sealer. When MTA first came out, it was fairly expensive and was used mostly by specialists. The price of TS has dropped considerably and should be part of every general dentist’s toolbox to provide the best possible treatment for our patients. OH
Dr. Levin has been a clinical instructor in Practice Dynamics and Community Dentistry and our faculty for the Mobile Dental Clinic within the University of Southern California School of Dentistry since 1985. He is in private practice in Huntington Beach, California. Dr. Levin was among the first evaluators of Biodentine in the US.
Oral Health welcomes this original article.
References:
1. ® Biodentine is a registered trademark of Septodont, Saint-Maur-des Fosses, France
2. ® ProRoot MTA is a registered trademark of Dentsply, Tulsa Division,York, PA USA
3. ® Dycal is a registered trademark of Dentsply, York, PA USA
4. ™Life is a trademark of Kerr Corporation, West Orange, CA USA
5. ® Ultracal XS is a registered trademark of Ultradent, South Jordan, UT USA
6. ® TheraCal LC is a registered trademark of Bisco Dental, Schaumburg, IL USA
7. ™BioRoot RCS is a trademark of Septodont, Saint-Maur-des Fosses, France











