
Abstract
Background: The classification system for periodontal diseases and conditions was revised in 2017. Evidence-based criteria were developed, and extensive revisions made, to reflect advancements regarding the etiology and progression of periodontal diseases. Among the many updates made to the previous classification system, a novel definition for periodontal health was introduced, along with a staging and grading scheme for periodontitis. The transition from health to disease is marked by the presence of acute inflammation, with subsequent destruction of periodontal hard and soft tissues as chronic inflammation ensues.
Objectives: Diagnosing periodontal conditions can be challenging as a result of some overlap between the clinical features of health, gingivitis, and periodontitis. Additionally, areas of ambiguity have been identified within the novel staging and grading system for periodontitis which may hinder clinicians from reaching an accurate diagnosis without a standardized approach. Therefore, the main goals of this work were to (a)foster proficiency in the clinical diagnosis of periodontal conditions and (b) emphasize practical understanding of the current classification guidelines.
Methodology: A stepwise platform was proposed in accordance with the revised system and will act as a clinical resource for dentists when diagnosing and classifying periodontal conditions. This stepwise approach provides the foundation required to reach an accurate diagnosis in a timely manner. Its use as a chairside diagnostic tool will facilitate the ongoing integration of the 2017 classification system into daily clinical practice.
Results & Discussion: The clinical application of this stepwise tool for the diagnosis of periodontal health and disease was demonstrated. Six case reports were diagnosed following the steps proposed, followed by the rationale which leads to an accurate diagnosis. Clinical attachment loss (CAL) is the first factor to be considered when diagnosing and classifying periodontal patients. Once the presence or absence of CAL is identified, the presence or absence of inflammation must be clinically investigated.
Conclusions: Practical understanding of the 2017 classification system is fundamental to reach accurate diagnoses for patients with periodontal health and disease and implement an appropriate treatment plan. Specifically, patients in advanced stages of periodontitis must be closely monitored due to their lack of predictability to benefit from standard periodontal therapies. Ultimately, this simplified diagnostic tool will aid in bridging the gap between research and development, and daily clinical practice.
Introduction
The diagnoses and classifications of periodontal and peri-implant diseases and conditions were revised in 2017 based on new knowledge and changes to the collective understanding of disease progression that have emerged over the past 20 years.1-5 With the goal of providing a standard framework that may be readily modified as new evidence emerges in clinical practice, research, and epidemiological surveillance, the updated guidelines offer clinicians a comprehensive system to aid in the diagnosis and classification of periodontitis and related gingival conditions.2,3,6
Multiple changes were made from the 1999 Periodontal Diseases and Conditions Classification System.7 (Table 1) Among these changes, a novel definition for periodontal health was introduced.8 Descriptions for gingival inflammatory diseases were also revamped to supplement the updated framework and maintain consistency with other diagnoses.6,9-11 An evidence-based framework was developed to diagnose and classify periodontitis, highlighted by a staging and grading system.3 The use of a staging and grading system was described as a more appropriate method to define periodontitis on an individual patient level. Furthermore, a staging and grading framework provided the evidence-based working foundation required for the eventual incorporation of biomarkers into the diagnosis and prognosis of periodontitis patients.2,3
Table 1

Periodontitis and gingival inflammatory diseases are highly prevalent, with approximately 50% of the population suffering from a form of periodontal disease.12 Therefore, it is paramount that clinicians are able to effectively recognize, diagnose, and classify disease based on the current classification scheme. This work strives to facilitate the continual transition of the 2017 classification system into clinical practice by providing clinicians an opportunity for self-assessment of knowledge and understanding. A step-by-step schematic to improve efficiency and consistency in the diagnosis and classification of periodontal conditions is proposed to foster chairside diagnoses. (Fig. 1) The diagnosis and classifications of clinical gingival health, gingivitis, and periodontitis are presented in a case report format and reviewed to aid in the application of this tool within the realm of the current diagnosis and classification system.
Fig. 1
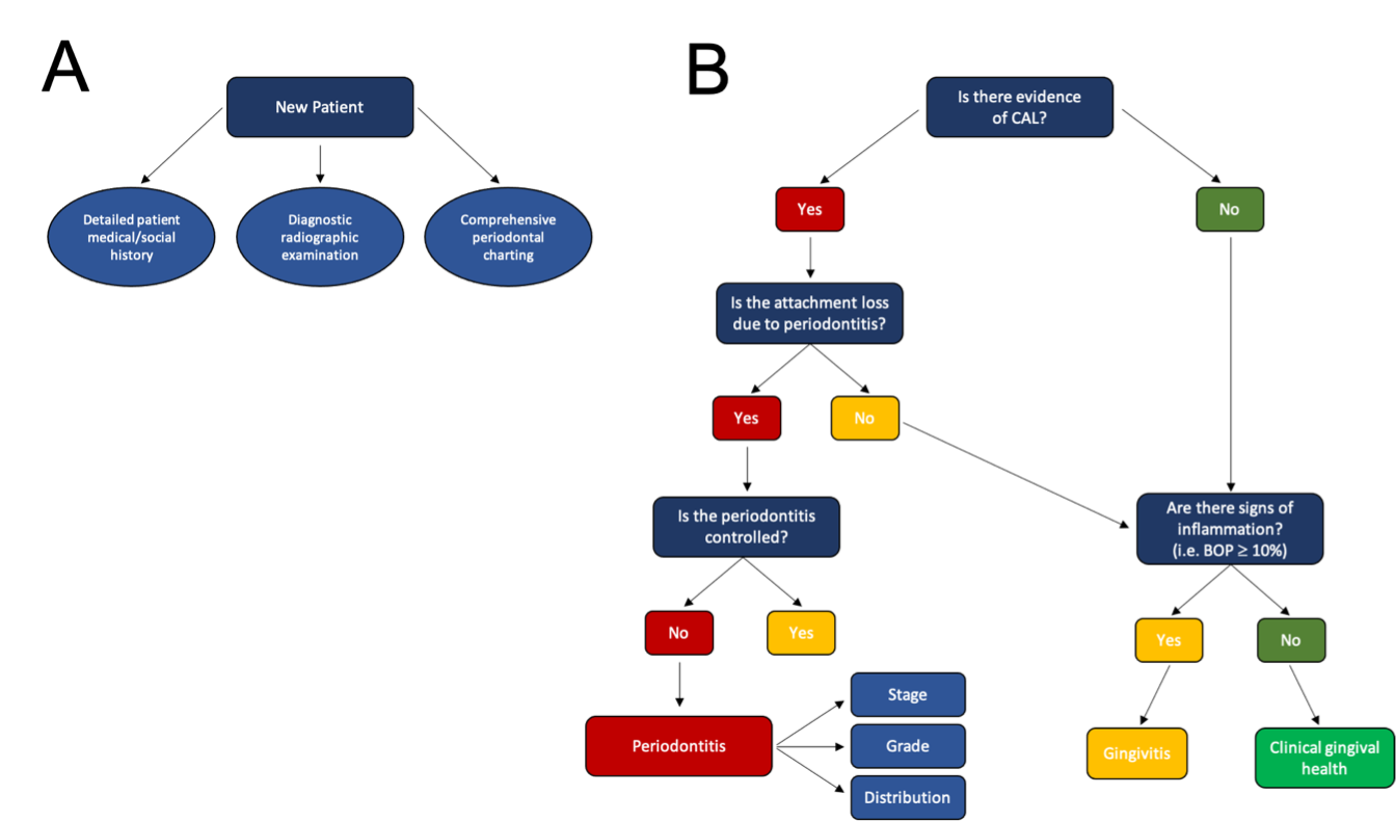
If the cause of attachment loss is due to periodontitis and there is a lack of evidence to support the control of etiologic factors and disease stability, proceed to staging and grading of periodontitis. If there is no loss of attachment, then it cannot be a periodontitis patient. Gingivitis and clinical gingival health may be considered as diagnoses in this case.
A Stepwise Tool for the Diagnosis of Periodontal Diseases and Conditions
Dental professionals should follow a practical diagnostic pathway to maximize efficiency and accuracy when using the new classification system. To aid in this, diagnostic flowcharts have been developed;13 however, there have been challenges while applying them clinically. Herein, a practical approach was proposed to incorporate the distinguishing features of periodontal diseases into a simplified diagnostic platform. (Fig. 1) The purpose for this reductionist model was to provide a basic understanding of how an accurate diagnosis may be reached utilizing the revised classification system. Additional nuances and details pertaining to specific diagnoses must be considered; therefore, this novel diagnostic platform should be used comprehensively to reach an accurate diagnosis.
The first step required to reach an accurate periodontal diagnosis is obtaining a complete medical and social history. Additionally, a comprehensive periodontal examination and diagnostic radiographs should be analyzed.13 Once these required diagnostic records have been reviewed, the presence and extent, or absence, of clinical attachment loss (CAL) must be determined.2,3 CAL represents the loss of periodontal tissue support which manifests in the forms of gingival recession and/or alveolar bone loss. Clinically, CAL is determined by the extent of gingival recession and periodontal probing depth; however, a quantifiable threshold does not necessarily exist for CAL due to the variability of clinical attachment level.14 Nonetheless, CAL is considered to be present where the CEJ is visible, or the periodontal probe terminates on the root surface. Therefore, PD cannot be used alone to determine whether CAL is present or not.
Where CAL is absent, the periodontium is considered intact. In these cases, other diagnoses such as clinical gingival health, biofilm-induced gingivitis, or non-biofilm-induced gingival pathologies (e.g., gingival candidosis) must be considered.6,9,15 When evidence of CAL is present, the etiologic factors responsible for the loss of attachment must be subsequently identified. There are cases in which CAL is a consequence of non-periodontitis factors. Non-periodontitis causes of CAL include, but are not limited to: traumatic toothbrushing, orthodontic-induced recession,16
surgical crown-lengthening,17 acute endo-periodontal lesions,15 impacted third molars,18 and restoration margins which violate the biologic width.19 In these cases, a diagnosis of periodontitis should not be considered.
Next, the presence, or absence, of inflammation must be determined clinically. This is primarily achieved by assessing the extent of bleeding on probing (BOP). BOP is often used as the main parameter in confirming the presence, or absence, of active disease.4,20 When BOP exists at ≥10% of periodontal probing sites, gingival inflammation is considered to be present; however, this number is a guideline rather than an absolute.3,6 For patients with an intact periodontium, determining the presence or absence of inflammation is the final step required to reach an appropriate diagnosis of health or gingivitis. For patients with periodontitis-related CAL, the severity, distribution, complexity, and risk of progression of the disease must be determined, in conjunction with the stage and grade of periodontitis, in order to develop an appropriate treatment plan.3
What is Periodontal Health?
Periodontal health was updated in the 2017 revision, and is now classified as one of three subtypes: clinical gingival health on an intact periodontium, clinical gingival health on a reduced periodontium (non-periodontitis patient), or clinical gingival health on a reduced periodontium (stable periodontitis patient).4,8 Clinical gingival health is characterized by a well-maintained and clinically intact periodontium with BOP at fewer than 10% of sites.8 For patients with a reduced periodontium, clinical gingival health may only exist if the CAL was attributed to an etiology other than periodontitis.4 Patients with a history of periodontitis may present with signs of clinical gingival health; however, the terms “stable” or “in remission” are reserved for these patients to indicate the irreversibility of CAL and a chronic increased risk for recurrence of disease.1
Transitioning from Health to Disease
The key distinction between clinical gingival health and gingivitis is the presence, or absence, of clinically detectable inflammation.1 The presence of inflammation is assessed by looking at the tissue colour, tone, and texture, as well as by measuring BOP. BOP is a clinical sign of active inflammation, but it does not influence the initial diagnosis, as defined by CAL.1,3,4 In general, a patient will transition from clinical gingival health to a state of gingival inflammation when BOP is present at ≥ 10% of periodontal probing sites. That is, the presence of some inflammation (i.e., < 10% of sites) does not automatically exclude a diagnosis of clinical gingival health.1
There is a bidirectional relationship between health and gingivitis, where the inflammation and associated effects in gingivitis are fully reversible.4 (Fig. 2) Therefore, a patient with gingivitis who is treated appropriately may re-establish clinical gingival health on an intact periodontium once the inflammation is resolved; however, a patient with treated periodontitis cannot return to a diagnosis of clinical health without the additional notation of being a stable periodontitis patient.4 Similarly, a patient with previous periodontitis may experience gingival inflammation at sites where probing depth (PD) is ≤ 3 mm. This may be termed gingival inflammation in a stable periodontitis patient, or more simply, gingivitis on a reduced periodontium in a successfully treated periodontitis patient.4
Fig. 2

Health may exist on a pristine, intact, or reduced periodontium in either a stable periodontitis patient or a non-periodontitis patient.
Gingivitis may exist on an intact, or reduced periodontium in a non-periodontitis patient. For periodontitis patients who are experiencing active periodontal inflammation, the accepted terminology to describe this state are gingival inflammation and/or gingivitis. The distinction between these terms is to signify that the progression from gingivitis to periodontitis is irreversible and associated with more complex treatment outcomes and prognoses.
Gingivitis
Gingival inflammation may exist on three distinct periodontal states: an intact periodontium, a reduced periodontium in a non-periodontitis patient, or a reduced periodontium in a periodontitis patient who is currently in remission.4,6,8 (Table 2) Gingivitis is a clinical diagnosis for a reversible inflammatory disease marked by common signs of inflammation, including erythema, edema, bleeding, tenderness, and enlargement.20 The term gingivitis may also be used to classify the presence of gingival inflammation on the already reduced periodontium of a previous periodontitis patient.4 Therefore, a diagnosis of gingivitis on a reduced periodontium in a patient with a history of periodontitis may be used to classify patients with CAL as a result of previous periodontitis.
Table 2

In essence, these two clinical diagnoses are not interchangeable, due to the fact that a patient with previous periodontitis who now displays gingival health or gingival inflammation remains at increased risk for recurrence of periodontitis and, therefore, must be closely monitored.4 Furthermore, for patients who cross the irreversible boundary between gingivitis and periodontitis, the prognosis and treatment options become increasingly complex. Therefore, a clear distinction must be made when diagnosing gingivitis on a reduced periodontium in a non-periodontitis patient versus gingivitis on a reduced periodontium in a patient with a history of periodontitis.
Biofilm-induced Gingival Diseases
Dental biofilm-induced gingivitis is one of the most highly prevalent inflammatory diseases of the body and considered to be the most common form of periodontal disease.6 In the absence of oral hygiene measures, biofilm-induced gingivitis will be clinically apparent after 10-21 days, and may be resolved within 5-10 days after oral hygiene is re-established.21 The acute inflammatory response observed in biofilm-induced gingivitis is initiated by the presence of bacterial plaque in the gingival sulcus.
The signs and symptoms of biofilm-induced gingivitis include pain, tenderness, edema, redness, and bleeding; however, initial changes from health to gingival disease may not be clinically discernible.22 Furthermore, the clinical appearance of gingivitis can be influenced by systemic and/or local risk factors. Systemic risk factors include, but are not limited to, smoking, hyperglycemia, nutritional factors, pharmacotherapies, hormonal fluctuations, and hematological conditions. Local risk factors may include xerostomia and dental biofilm retention factors, such as inadequate restorative margins or severe crowding.4,6
Non-biofilm-induced Gingival Diseases
Biofilm-independent gingival diseases are less common than dental plaque-induced gingival pathologies. Most of these conditions are manifestations of systemic disease, but other etiologies may include genetic disorders, infections, immune diseases, neoplasms, metabolic diseases, and traumatic lesions.9 Bacterial infections play a significant role in the initiation of both biofilm-induced and non-biofilm-induced gingival diseases; however, non-biofilm-induced diseases are usually the result of a specific bacterial infection.4,9 Furthermore, non-biofilm-induced gingival diseases may originate from viral or fungal infections, while biofilm-induced gingivitis has a bacterial etiology.6,9 Because of the wide array and complex etiologies of non-plaque-induced gingival diseases, their clinical presentations and prognoses may vary significantly. Nonetheless, some non-biofilm-induced gingival pathologies may present with similar clinical features, making it challenging to differentiate them from their biofilm-induced counterparts solely based on qualitative information.9
Gingival Inflammation vs. Gingival Enlargement
Both gingival inflammation and gingival enlargement may result in clinically inflated PDs without CAL, thereby potentially overestimating the extent of disease.4 (Table 2) Although they may share quantitative similarities, their clinical presentations are generally distinct. Gingival inflammation is characterized by edema, erythema, bleeding, tenderness, and enlargement; however, gingival enlargement alone may occur in the absence of these additional features.9,23 For example, hereditary gingival fibromatosis is a non-plaque-induced disease as a result of a genetic mutation, which presents as a generalized fibrotic gingival overgrowth, but does not necessarily include bleeding, erythema, and/or tenderness.24 Gingival enlargement may still present with classical signs of inflammation, due to difficulty with maintaining proper oral hygiene. As a result, gingivitis may ensue as biofilm accumulates in the gingival sulcus. The key difference, however, is “gingival inflammation” often presents with enlargement of the gingiva from swelling, while “gingival enlargement” is usually more fibrotic and not edematous.
Crossing the Line: Irreversible Progression from Gingivitis to Periodontitis
Gingivitis is confined to the soft tissues of the periodontium,4,6,20 while periodontitis features CAL in the form of alveolar bone loss, periodontal pocketing and/or gingival recession as a consequence of a disproportionate host immune response.4,6,25 This results in periodontal hard and soft tissue destruction, hence the irreversibility of periodontitis.22 According to the novel classification system for periodontal diseases and conditions, the loss of periodontal tissue support as a result of chronic inflammation is the defining clinical feature of periodontitis.2,3,26
To meet the case definition of a periodontitis patient, the etiology of the CAL must be due to periodontal inflammatory disease.2 Non-periodontitis forms of CAL include subgingival caries, malpositioned third molars, endo-periodontal lesions, systemic diseases or conditions affecting the periodontal supporting tissues, and gingival recession due to trauma.1,2 The presence of CAL on its own does not necessarily fulfill the criteria for a diagnosis of periodontitis. Instead, to clinically define a periodontitis patient, interdental CAL due to periodontitis must be evident at ≥ 2 non-adjacent teeth, or on the buccal aspect of ≥ 2 teeth.2
Staging & Grading System for Periodontitis
Under the 1999 classification system, periodontitis was broadly divided into “aggressive” and “chronic” forms.7 Although these diagnoses represented different clinical presentations of periodontitis, these terms did not provide any guidance with regard to treatment planning or disease management. Specifically, it was suggested that there was insufficient evidence to differentiate between aggressive and chronic periodontitis in terms of their pathophysiology.3 As a result, in 2014 the American Academy of Periodontology created a task force to address these concerns and develop a classification system that was more clinically relevant.1
Staging Periodontitis
The staging system has been developed to provide a relative measure of disease severity and complexity of management for periodontitis patients.3 Based on clinical and radiographic indicators, periodontitis may be given a Stage from I to IV.3 (Table 3) Stage I and II periodontitis represent mild forms of the disease and are normally treated in general practice. While, Stage III and IV periodontitis are more advanced forms and their management generally requires the expertise of a periodontist.2,3 To determine the stage of periodontitis for a patient, specific local factors, such as interdental CAL, radiographic bone loss (RBL), type of bone loss (e.g., horizontal or vertical), tooth loss, probing depth (PD), furcation involvement, and need for complex rehabilitation, must all be considered.1 Furthermore, when assigning a stage to a periodontitis patient, the most severe site(s) in the mouth should be considered to determine the appropriate stage; however, this should be done in conjunction with good clinical judgement.
Table 3

The identification of tooth loss due to a history of periodontal disease is a new criterion to be considered in the diagnostic process. This is clinically relevant when determining future prognoses because evidence of tooth loss due to periodontitis is associated with lower predictability to standard periodontal therapies.27 Thus, Stage III and IV periodontitis represent a higher level of complexity with a different disease trajectory than Stage I and II, and as such these diagnoses should be considered distinct.27 Teeth with a hopeless prognosis should be considered as “teeth lost” when differentiating between Stage III and Stage IV periodontitis.28
Extent & Distribution
Determination of the extent and distribution should be done after the completion of staging.28 It is important to emphasize that the extent of periodontitis is a descriptive factor and does not influence the assigned stage of periodontitis.4 Instead, the extent and distribution are evaluated based on the percentage of teeth at the stage-defining severity level (i.e., the most severe site(s)).17 Generally, three patterns exist for the extent and distribution of periodontitis, including localized, generalized, and molar/incisor. Periodontitis is considered localized if < 30% of teeth are involved, while generalized periodontitis describes a patient with ≥ 30% of teeth involved.
Grading Periodontitis
The grading scheme for periodontitis was designed to assess and predict the rate of disease progression. Grades of periodontitis range from A to C, where Grade A represents a slow rate of progression, Grade B refers to a moderate rate, and Grade C defines a rapid rate.3 (Table 4) There are two types of primary criteria which should be considered prior to assigning a grade to a periodontitis patient: direct and indirect evidence. For patients with previous records available, bone loss over time provides direct evidence of disease progression for determining the appropriate grade.3 However, for new patients and/or where previous records are not available, indirect evidence may be considered. This is most commonly assessed by determining the percentage of bone loss in a patient, dividing by their age, and assigning a grade based on that ratio. (Table 5)
Table 4
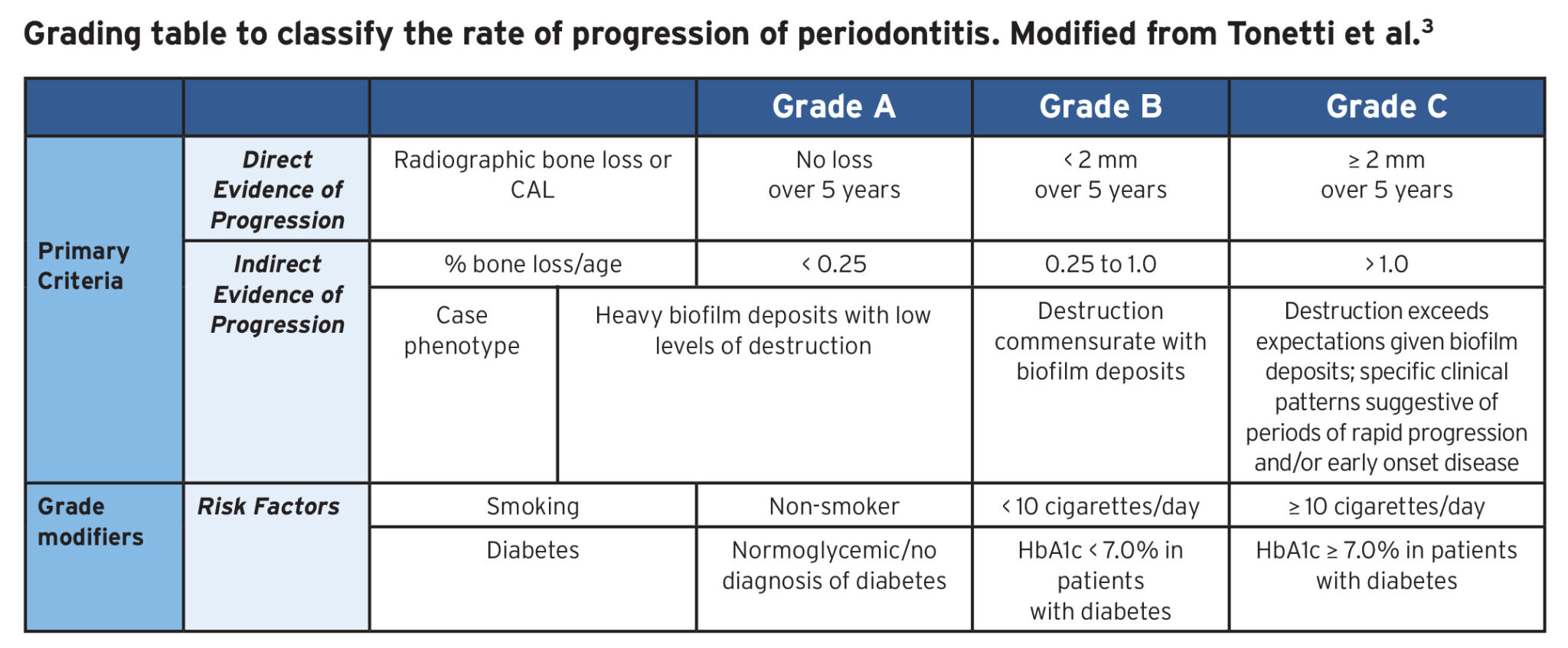
Table 5

It has been suggested that dentists may choose to assume Grade B as a starting point for all patients, in the absence of any evidence to suggest otherwise. In addition to the primary criteria, grade modifiers may be considered to alter the assigned grade.4,5,29 Grade modifiers include smoking history and diabetes status. The presence of either smoking or diabetes in periodontitis patients can only be used to indicate an increase in the likelihood of disease progression. Therefore, when the primary grading criteria indicates Grade A, a grade modifier may increase the Grade to B or C. This does not work conversely; that is, where the primary grading criteria indicates Grade C, a grade modifier cannot decrease the Grade to A or B.
Case 1
Patient A is a 16-year-old female who presented with a congenitally missing tooth #32. (Fig. 3) Her medical history is unremarkable. She does not smoke cigarettes. Her dental history includes previous orthodontic treatment to create and maintain space for a future implant at site #32. She is compliant with excellent home care and oral hygiene. On clinical examination, all periodontal PDs were 1-3 mm with two isolated 4 mm PDs at tooth #37 mesiobuccal and distolingual. Approximately 4% of sites had BOP. There was no significant recession, nor other mucogingival defects noted. Radiographically, her alveolar bone levels appeared to be consistently within 2 mm of the cementoenamel junction (CEJ).
Fig. 3

Discussion: Case 1
The correct diagnosis for Patient A is clinical gingival health on an intact periodontium. Following the step-by-step approach to diagnosing periodontal diseases and conditions, (Fig. 1) the first determination to be made is the presence or absence of CAL. There is no CAL because there is no evidence of recession and when probing, the probe tip does not rest on the root surface. Upon review of her clinical records, nearly all PDs are measured to be ≤ 3 mm with the exception of two sites around tooth #37. Given this patient’s excellent oral hygiene regimen, compliance, and non-contributory medical history, the localized 4 mm PDs are not considered to be periodontal pockets. Instead, these PDs may be pseudopockets, or gingival pockets, as a result of gingival enlargement creating a greater PD, as opposed to true periodontal pockets. This is corroborated by the absence of crestal bone loss, noted on the panoramic radiograph. (Fig. 3) This patient has had no CAL.
The next step is to assess the presence, or absence, of gingival inflammation. In this case, localized BOP is present, but accounts for less than 10% of sites. This is consistent with clinical gingival health. While having up to 10% of sites with BOP is the criterion for clinical gingival health, this number should be interpreted within an overall assessment of the patient’s periodontal state and clinical judgment. For example, a patient with 11% sites of BOP may still be considered “healthy” in the absence of true CAL and other gingival conditions. Ultimately, BOP is only one parameter to describe the extent of inflammation present.1,3 In essence, a more nuanced approach, including consideration of the appearance, texture, and colour of the gingiva should be utilized while assessing for the presence or absence of gingival inflammation.27 As is evident in , Fig. 3 the pink and stippled appearance of the gingiva and healthy levels of alveolar bone are characteristic of clinical gingival health. Therefore, taking into account the lack of CAL, healthy crestal bone levels, negligible gingival inflammation, and absence of erythema and edema, clinical gingival health on an intact periodontium is the most appropriate diagnosis for Patient A.
Case 2
Patient B is a 52-year-old female who presented with a chief complaint of “black triangles” between her teeth. (Fig. 4). Her dental history includes orthodontic treatment 30 years ago; however, her teeth have shifted, and she is now interested in clear aligner therapy. She reports no previous history of periodontal surgery or advanced periodontal therapy. Patient B has mild hypertension, controlled by diltiazem. She does not smoke cigarettes. Her oral hygiene is good, and she is compliant with dental care. On clinical examination, all periodontal PDs were 2-3 mm and approximately 7% of sites had BOP. Generalized recession was noted for all teeth and a decreased width of attached gingiva was recorded for teeth #31, 32, 34, 35, 36, 41, 42, 43, 45, 46. Grade 1 mobility was noted for teeth #15, 25, 31, 32, 41, 42. Radiographically, the alveolar bone level appeared to be normal, with the exception of mild horizontal bone loss at sites #15, 25, 31, 32, 41, 42.
Fig. 4

Discussion: Case 2
The correct diagnosis for Patient B is clinical gingival health on a reduced periodontium (non-periodontitis patient). The clinical features of gingival health on a reduced periodontium include the absence of BOP, erythema, edema and patient symptoms in the presence of reduced clinical attachment and/or alveolar bone levels.4 In contrast to Patient A in Case 1, Patient B demonstrates periodontal attachment loss. This is noted by the localized areas of alveolar bone loss on the panoramic radiograph, and the recession defects and loss of interproximal gingival papillae on the intraoral photograph. (Fig. 4)
The next step is to assess whether this attachment loss can be attributed to periodontitis, or some other factor(s). In certain cases, this is rather straightforward: for example, a patient who reports a history of periodontal disease. In other cases, it is less clear; therefore, we must rely on an overall assessment of clinical parameters that are generally associated with periodontitis to determine the etiology of the CAL. All PDs are ≤ 3 mm and there is no evidence of radiographic bone loss; therefore, it is unlikely that this patient had suffered from periodontitis. Instead, the attachment loss was likely the result of an alternate etiology. This patient has a thin gingival phenotype, which predisposes her to an increased risk for gingival recession.30 Based on this genetic predisposition, and the history provided by the patient, it is most probable that the gingival recession and open gingival embrasures are orthodontically-related (16). From this, Patient B is confirmed to be a non-periodontitis patient with a reduced periodontium.
Following the approach illustrated in Figure 1, the next step is to investigate the presence of inflammation. As evidenced by the pink and stippled appearance of the gingiva and BOP at < 10% of sites, Patient B shows characteristics of periodontal health.8 Therefore, considering that the CAL is unrelated to periodontitis and there is currently a lack of inflammation, the correct diagnosis for Patient B is clinical gingival health on a reduced periodontium in a non-periodontitis patient.
Case 3
Patient C is a 17-year-old female who presented with the chief complaint of “sore gums”. (Fig. 5) Her medical history is unremarkable. She does not smoke cigarettes. She brushes her teeth with a manual toothbrush once daily, flosses rarely, and visits her dentist every 12 months for recall examinations and scaling. She is interested in orthodontic treatment to correct her malocclusion and mild crowding. On clinical examination, all periodontal PDs were 2-4 mm and approximately 44% of sites had BOP. No gingival recession was evident. Buccal exostoses were noted, along with gingival erythema, edema, and tenderness. Radiographically, the alveolar bone level appeared to be within 2 mm of the cementoenamel junction (CEJ) for all teeth.
Fig. 5

Discussion: Case 3
The appropriate diagnosis for Patient C is gingivitis on an intact periodontium. Using a step-by-step approach to diagnosing periodontal diseases and conditions, (Fig. 1) the first step is to determine the presence and extent, or absence, of CAL. The periodontal parameters indicate there is no gingival recession, and the probe tip does not terminate on the root surface. Additionally, there is no evidence of radiographic bone loss despite the presence of localized 4 mm PDs. The gingiva is erythematous and demonstrates ≥ 10% BOP, indicating active gingival inflammation.
There are several reasons why a 4 mm PD may be measured on an inflamed periodontium. Firstly, when the gingiva is inflamed the periodontal probe is more likely to penetrate deeper or past the junctional epithelium and into the connective tissue attachment, leading to an overestimation of the actual sulcus.1,4,6,31 Furthermore, gingival swelling as a result of inflammation may lead to the formation of gingival pockets or pseudopockets.4 Given the presence of inflammation, these localized 4 mm PDs are pseudopockets and, therefore, are not truly indicative of CAL. Ultimately, upon recognizing the lack of CAL, but presence of gingival inflammation, the correct diagnosis for Patient C is gingivitis on an intact periodontium.4
Case 4
Patient D is a 22-year-old female who presented with a chief complaint of dentinal hypersensitivity on tooth #41. (Fig. 6) Her dental history includes previous orthodontic treatment, and her medical history is non-contributory. She does not smoke cigarettes. Patient D is compliant with good home care; however, she is unable to brush her mandibular anterior teeth due to severe sensitivity associated with gingival inflammation. On clinical examination, all periodontal PDs were 1-3 mm and approximately 14% of sites had BOP. Isolated recession was recorded at tooth #41 and a decreased width of attached gingiva was noted for teeth 31, 32, 33, 41, 42, 43. Radiographically, the alveolar bone levels appeared to be consistently within 2 mm of the CEJ of all teeth.
Fig. 6

Discussion: Case 4
The diagnosis for Patient D is gingivitis on a reduced periodontium (non-periodontitis patient). There is evidence of CAL in the form of recession at tooth #41 buccal, even though the interproximal attachment appears intact radiographically. (Fig. 6) Since there is evidence of attachment loss, this patient cannot be classified as having periodontal health, even though the attachment loss is isolated to a single tooth.1 Therefore, the diagnosis must include a “reduced periodontium” qualification. It is important to recognize that recession is a form of CAL, but simply a lack of keratinized tissue or a decreased width of attached gingiva, is not. Although a lack of keratinized tissue may influence the progression of CAL, alone it does not satisfy the criteria to diagnose a reduced periodontium.31
To determine whether the CAL was a result of periodontitis or an alternative etiology, the overall patient history and clinical presentation needs to be considered. Since all PDs are ≤ 3 mm and significant risk factors for periodontitis are absent, the etiology of CAL is likely not related to periodontitis. Based on this patient’s history of orthodontic treatment, this should be considered as a possible etiology for the recession.16 Specifically, a history of mandibular crowding and a non-extraction pattern of treatment would support this. To assess the presence of inflammation, the extent of BOP is considered. Nearly 44% of sites present with BOP and the clinical intraoral photograph depicts erythematous and edematous gingiva. Given the extent of BOP at ≥ 10% of probing sites, it is evident that gingival inflammation, in the form of gingivitis, is present. Ultimately, since the crestal bone levels are stable with these clinical signs of gingival inflammation, the correct diagnosis for Patient D is confirmed as gingivitis on a reduced periodontium in a non-periodontitis patient.
Case 5
Patient E is a 45-year-old male who presented with a chief complaint of “poor esthetics.” (Fig. 7) His dental history includes irregular dental care throughout his adult life. His medical history includes asthma controlled by salbutamol. Patient E is non-diabetic and does not smoke cigarettes. He brushes his teeth twice daily and does not floss. On clinical examination, all periodontal PDs ranged from 2-6 mm, with the majority of sites measuring 3-5 mm. Approximately 23% of sites had BOP. There were generalized mobilities. There was evidence of generalized recession. No other mucogingival defects were identified. Radiographically, Patient E presented with vertical bone loss at tooth #26 mesial and #35 distal.
Fig. 7
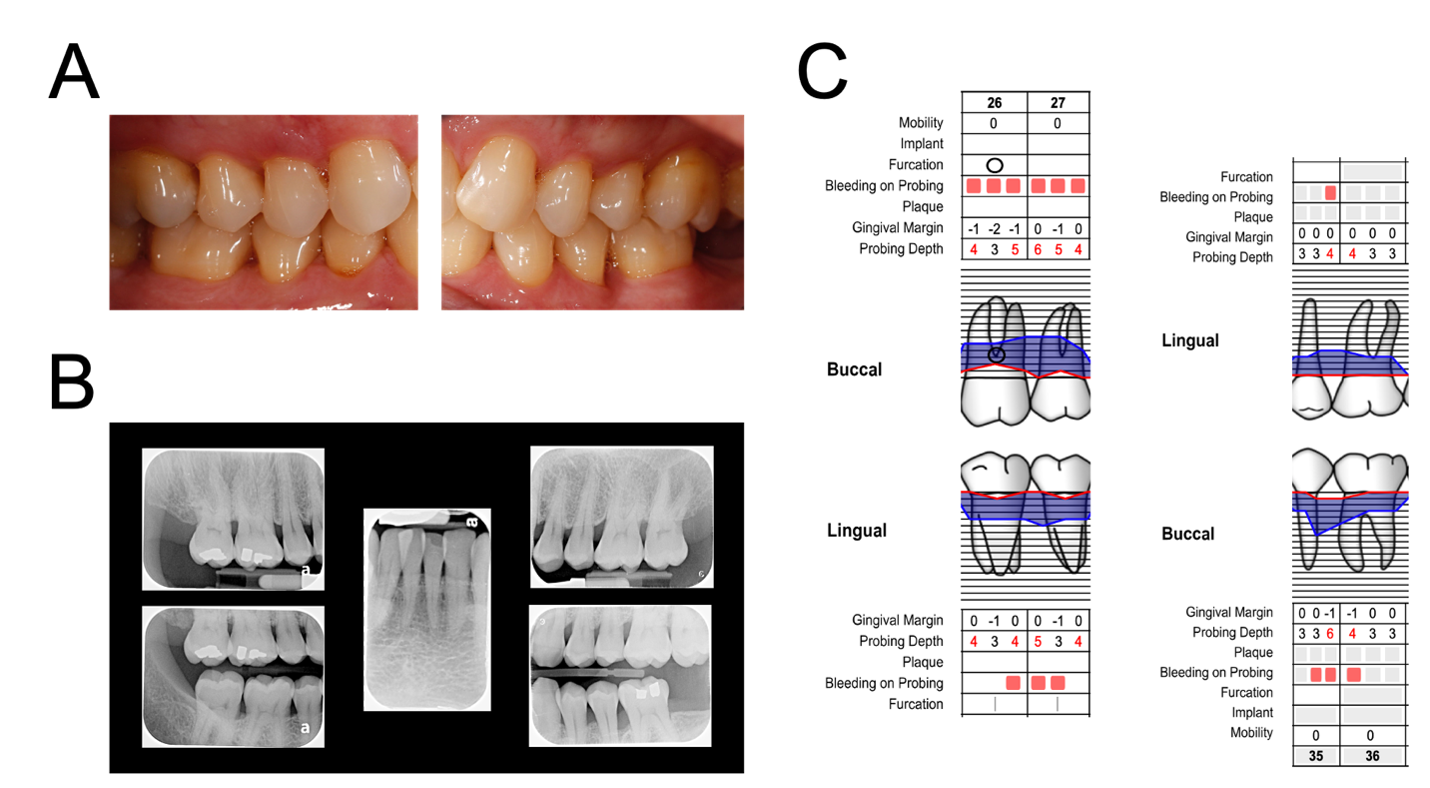
B. periapical radiograph maxillary left lateral incisor view (centre), periapical radiograph maxillary right 2nd molar view (upper left) and premolar/1st molar view (upper right), and bitewing radiograph right posterior view (bottom left) and
left premolar/1st molar view (bottom right), and
C. periodontal charting at teeth #26, 27, 35, and 36.
Discussion: Case 5
The appropriate diagnosis for Patient E is periodontitis (Stage II, Grade B, localized). Referring to the stepwise approach, (Fig. 1) the presence and extent, or absence, of CAL should first be evaluated. According to the periodontal parameters provided, there are several 4-5 mm PDs with two isolated 6 mm PDs. Given the fact that several PDs were beyond 3 mm, it is evident that this patient has experienced CAL. Additionally, based on the radiographic presence of generalized horizontal bone loss and vertical bone defects, the presence of CAL is confirmed. Considering that the sites with CAL also have BOP, it can be assumed that the CAL is a result of this chronic inflammatory periodontal disease. Since less than 30% of sites are affected with Stage II periodontitis, the extent and distribution of periodontitis are considered localized.
Once it is determined that Patient E is a periodontitis patient, the staging and grading system for periodontitis is applied.3 (Table 3) This patient meets criteria under both Stage II and Stage III: the vertical bone loss at teeth #26 mesial and #35 distal are in the range of 15-33%; however, a probing depth of 6 mm is present. (Fig. 7) According to Tonetti et al., “in general it only takes one complexity factor to shift the diagnosis to a higher stage. It should be emphasized that these case definitions are guidelines that should be applied using sound clinical judgement to arrive at the most appropriate clinical diagnosis.”3 Furthermore, there are “gray zones” that have been identified within the current classification system for cases which do not solely rely on simple decision guidelines.27 Therefore, based on this literature there is value in reviewing diagnoses that are not necessarily “clear-cut”, such as the case for Patient E. When classifying this patient, the entire clinical presentation must be taken into account using sound clinical reasoning and judgement. One may argue that the presence of an isolated 6 mm PD would indicate Stage III; however, many of the complexity factors for Stage III periodontitis are not satisfied. The patient is not missing any teeth due to periodontitis, and the extent of bone loss at the most severe site (tooth #35) remains within the coronal 33%.28 Also, there is no indication of furcation involvement and no evidence of ridge defects. Therefore, despite the fact that some complexity criteria for Stage III periodontitis are met, a diagnosis of Stage II is confidently applied using comprehensive clinical judgement.
To determine the rate of progression of the disease, the main factors to consider are the patient’s age, extent of bone loss, level of biofilm deposits, and history of smoking and diabetes. As a younger patient with a history of gingivitis and fair oral hygiene, it is expected that the level of biofilm deposits was commensurate with the extent of bone loss. This typically justifies Grade B in the absence of any grade modifiers. The presence of generalized horizontal bone loss with isolated vertical bone loss up to 33% supports the percent bone loss to age ratio for Grade B (0.25 to 1.0). (Table 5) Patient E is non-diabetic and does not smoke cigarettes, therefore, there are no grade modifiers present to influence the risk of disease progression. Taking the above information into account, the correct diagnosis for Patient E is periodontitis (Stage II, Grade B, localized).
Case 6
Patient F is a 42-year-old female who presented with a chief complaint of “loose teeth”. (Fig. 8) She is currently undergoing orthodontic treatment with clear aligners. She has a history of infrequent and irregular dental care due to financial limitations; however, she recently committed to regular dental appointments. Her medical history is unremarkable, and she does not smoke cigarettes. Her oral hygiene is fair. On clinical examination, periodontal PDs varied from 2-10 mm with several 6-7 mm measurements. Approximately 21% of sites had BOP. There were generalized mobilities. Severe, localized recession was noted at tooth #26 lingual and a lack of keratinized tissue was recorded at tooth #34. Her third molars were congenitally missing; tooth #16 was extracted 15 years ago after a fracture; tooth #27 was extracted 5 years ago due to periodontal disease; and tooth #37 was removed 3 years ago due to gross caries. Radiographically, there was generalized horizontal bone loss which varied between 25-70% and notable localized vertical defects at teeth #21 mesial, #26 mesial, #45 mesial and distal, and #47 distal.
Fig. 8

B. full-mouth series, and C. periodontal charting at teeth #12, 11, 21, 26, 44, 45, 46, 47.
Discussion: Case 6
The correct diagnosis for Patient F is periodontitis (Stage III, Grade C, generalized). As before, determining the presence or absence of CAL is the first step in reaching a definitive diagnosis. Based on the generalized horizontal bone loss and presence of numerous 6-7 mm PDs and beyond, it is evident that Patient F has experienced significant CAL. To determine whether the CAL was attributed to periodontitis, all of the presented information is taken into account. Firstly, the patient’s history of non-compliance and infrequent dental visits are a significant risk factor in the development of inflammatory periodontal diseases. The presence of inflammation, BOP, and mobility due to alveolar bone loss are sufficient to confirm that the CAL is attributed to active periodontitis. Nonetheless, this patient is currently undergoing orthodontic therapy with active periodontitis, so it is expected that their periodontal condition has been exacerbated.
Next, the staging and grading system for periodontitis is applied.3 With several PD’s equal to or greater than 6-7 mm (Fig. 8) and generalized alveolar bone loss extending into the middle third of the roots and beyond, this patient is confirmed as either a Stage III or Stage IV periodontitis patient. One distinguishing factor between Stage III and Stage IV periodontitis is the
number of teeth lost due to periodontitis and the need for complex rehabilitation. Although this patient has significant CAL, the stability and integrity of the masticatory complex is minimally affected. There was some minor drifting of teeth, however the overall vertical dimension is maintained. As previously mentioned, a standardized approach, such as the stepwise schematic illustrated in Figure 1, should be used in combination with sound clinical judgement to reach an appropriate diagnosis.27 After utilizing this comprehensive approach, the severity of disease in Patient F was determined to be Stage III periodontitis. Nevertheless, it is important to re-iterate that patients who are diagnosed with Stage III or Stage IV periodontitis will require extensive treatment and should be appropriately managed by a periodontist.27
To determine the extent and distribution of the disease, the overall number of sites affected by Stage III periodontitis must be evaluated. In this example, since > 30% of all sites are affected by active disease meeting the Stage III definition, “generalized” is the appropriate descriptor. It is important to reiterate that the extent and distribution of periodontitis is the least important diagnostic criteria. Staging is characterized by the severity and complexity of a case, while grading aims to capture the speed of the disease progression, responsiveness to therapy, and potential impact on systemic health.3 These latter criteria are the most important considerations for future treatment planning of periodontitis patients.2,3
While grading the disease, the initial assumption is to assume Grade B if there are no previous records. After reviewing the patients’ records, however, it becomes clear that Grade C is a better representation for this patient. The first criteria reviewed is the percent bone loss to age ratio, as listed in Table 5. There are several sites which demonstrate 50% alveolar bone loss or more, with the most severe site at tooth #26 with approximately 70% bone loss. At the worst site the % bone loss/age ratio in this case is > 1; therefore, Grade C is most appropriate. Given the above, the diagnosis for Patient F is periodontitis (Stage III, Grade C, generalized).
Conclusion
Clinical gingival health exists on a continuum. The periodontal status and clinical presentations may vary for patients with clinical gingival health on an intact vs. reduced periodontium. Likewise, the periodontal status and clinical presentations for patients with gingivitis may vary. Although the clinical spectrum of periodontal health and disease may be broad, determining the presence of CAL and, subsequently, the presence of inflammation, can be useful to organize patients into the correct diagnostic category. Periodontitis is an irreversible disease and the treatment strategies used to manage patients at different stages of this disease may be significantly different in terms of successful treatment outcomes. Therefore, an accurate diagnosis is essential to developing an appropriate treatment plan for patients with periodontal diseases.
Clinicians should follow a standardized and comprehensive approach, considering all information available prior to reaching a final diagnosis, to ensure appropriate periodontal therapies are proposed. We have devised a user-friendly, step-by-step schematic which can be utilized chairside to facilitate the continual transition of the updated classification into daily practice. This stepwise diagnostic tool should be used to gain familiarity with the new classification guidelines. Although gray areas have been identified within the updated classification system, our stepwise approach to diagnosis under the new classification system can be applied to aid in its application. As evidence continues to emerge, this may be further modified, to ensure the most appropriate guidelines are always in place.
Oral Health welcomes this original article.
The authors have no financial interests to disclose.
a Faculty of Dentistry, University of Toronto,
124 Edward Street, Toronto ON M5G 1G6
+ Corresponding Author
Corresponding Author Information:
Dr. Ryan Schure, Predoctoral Program Director of Periodontology, Faculty of Dentistry, University of Toronto. 124 Edward Street, Toronto, ON M5G 1G6. Email: ryan.schure@dentistry.utoronto.ca
Tel: 416-864-8210
References
- Caton JG, Armitage G, Berglundh T, Chapple ILC, Jepsen S, Kornman KS, et al. A new classification scheme for periodontal and peri-implant diseases and conditions – Introduction and key changes from the 1999 classification. J Periodontol. 2018;89(March):1–8.
- Papapanou PN, Sanz M, Buduneli N, Dietrich T, Feres M, Fine DH, et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Periodontol. 2018;89(December 2017):S173–82.
- Tonetti MS, Greenwell H, Kornman KS. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J Periodontol. 2018;89(February):S159–72.
- Chapple ILC, Mealey BL, Van Dyke TE, Bartold PM, Dommisch H, Eickholz P, et al. Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Periodontol. 2018;89(December 2017):S74–84.
- Jepsen S, Caton JG, Albandar JM, Bissada NF, Bouchard P, Cortellini P, et al. Periodontal manifestations of systemic diseases and developmental and acquired conditions: Consensus report of workgroup 3 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Periodontol. 2018;89(December 2017):S237–48.
- Murakami S, Mealey BL, Mariotti A, Chapple ILC. Dental plaque-induced gingival conditions. J Periodontol. 2018;89(February 2017):S17–27.
- Armitage GC. Development of a classification system for periodontal diseases and conditions. Ann Periodontol. 1999;4(1):1–6.
- Lang NP, Bartold PM. Periodontal health. J Periodontol. 2018;89(April):S9–16.
- Holmstrup P, Plemons J, Meyle J. Non-plaque-induced gingival diseases. J Periodontol. 2018;89(September 2017):S28–45.
- Heitz-Mayfield LJA, Salvi GE. Peri-implant mucositis. J Periodontol. 2018;89(September 2017):S257–66.
- Ravidà A, Galli M, Siqueira R, Saleh MHA, Galindo-Morenzo P, Wang HL. Diagnosis of peri-implant status after peri-implantitis surgical treatment: Proposal of a new classification.
J Periodontol. 2020;(April):1–9. - Eke PI, Dye BA, Wei L, Thornton-Evans GO, Genco RJ. Prevalence of periodontitis in adults in the united states: 2009 and 2010. J Dent Res. 2012;91(10):914–20.
- Dietrich T, Ower P, Tank M, West NX, Walter C, Needleman I, et al. Periodontal diagnosis in the context of the 2017 classification system of periodontal diseases and conditions – Implementation in clinical practice. Br Dent J. 2019;226(1):16–22.
- Haffajee AD, Socransky SS, Lindhe J, Kent RL, Okamoto H, Yoneyama T. Clinical risk indicators for periodontal attachment loss. J Clin Periodontol. 1991;18(2):117–25.
- Herrera D, Retamal-Valdes B, Alonso B, Feres M. Acute periodontal lesions (periodontal abscesses and necrotizing periodontal diseases) and endo-periodontal lesions. J Periodontol. 2018;89(June 2017):S85–102.
- Wishney M. Potential risks of orthodontic therapy: a critical review and conceptual framework. Aust Dent J. 2017;62:86–96.
- Planciunas L, Puriene A, Mackeviciene G. Surgical lengthening of the clinical tooth crown. Stomatologija. 2006;8(3):88–95.
- Arta SA, Pourabbas Kheyradin R, Mesgarzadeh AH, Hassanbaglu B. Comparison of the influence of two flap designs on periodontal healing after surgical extraction of impacted third molars. J Dent Res Dent Clin Dent Prospects. 2011;5(1):1–4.
- Ercoli C, Caton JG. Dental prostheses and tooth-related factors. J Periodontol. 2018;89(September 2017):S223–36.
- Trombelli L, Farina R, Silva CO, Tatakis DN. Plaque-induced gingivitis: Case definition and diagnostic considerations. J Clin Periodontol. 2018;45(September 2017):S44–67.
- Loe H, Theilade E, Jensen SB. Experimental Gingivitis in Man. J Periodontol. 1965;36(3):177–87.
- Page RC, Schroeder HE. Pathogenesis of Inflammatory Periodontal Disease: a Summary of Current Work. Lab Investig. 1976;34(3):235–49.
- Agrawal AA. Gingival enlargements: Differential diagnosis and review of literature. World J Clin Cases. 2015;3(9):779.
- Coletta RD, Graner E. Hereditary Gingival Fibromatosis: A Systematic Review. J Periodontol. 2006;77(5):753–64.
- Page RC, Offenbacher S, Schroeder HE, Seymour GJ, Kornman KS. Advances in the pathogenesis of periodontitis: Summary of developments, clinical implications and future directions. Periodontol 2000. 1997;14(1):216–48.
- Needleman I, Garcia R, Gkranias N, Kirkwood KL, Kocher T, Iorio A Di, et al. Mean annual attachment, bone level, and tooth loss: A systematic review. J Periodontol. 2018;89(April 2017):S120–39.
- Kornman KS, Papapanou PN. Clinical application of the new classification of periodontal diseases: Ground rules, clarifications and “gray zones.” J Periodontol. 2020;91(3):352–60.
- Sanz M, Papapanou PN, Tonetti MS, Greenwell H, Kornman K. Guest Editorial: Clarifications on the use of the new classification of periodontitis. J Periodontol. 2020;(March):2020.
- Chee B, Park B, Bartold PM. Periodontitis and type II diabetes: A two-way relationship. Int J Evid Based Healthc. 2013;11(4):317–29.
- Kim DM, Bassir SH, Nguyen TT. Effect of gingival phenotype on the maintenance of periodontal health: An American Academy of Periodontology best evidence review.
J Periodontol. 2020;91(3):311–38. - Cortellini P, Bissada NF. Mucogingival conditions in the natural dentition: Narrative review, case definitions, and diagnostic considerations. J Periodontol. 2018;89(January):S204–13.
About the Authors
 Braedan R.J. Prete is a third-year student in the Doctor of Dental Surgery (DDS) program at the Faculty of Dentistry, University of Toronto. He can be reached at braedan.prete@mail.utoronto.ca.
Braedan R.J. Prete is a third-year student in the Doctor of Dental Surgery (DDS) program at the Faculty of Dentistry, University of Toronto. He can be reached at braedan.prete@mail.utoronto.ca.
 Siavash Hassanpour is a periodontist practicing in the North York region of Toronto, ON. He is a Clinical Instructor in the Graduate and Undergraduate Periodontology programs at the Faculty of Dentistry, University of Toronto. He can be reached at drhassanpour@northyorkperio.com
Siavash Hassanpour is a periodontist practicing in the North York region of Toronto, ON. He is a Clinical Instructor in the Graduate and Undergraduate Periodontology programs at the Faculty of Dentistry, University of Toronto. He can be reached at drhassanpour@northyorkperio.com
 Jim Y. Lai is an Associate Professor, Teaching Stream and Vice Dean of Education at the Faculty of Dentistry, University of Toronto. He can be reached at jimyuan.lai@dentistry.utoronto.ca
Jim Y. Lai is an Associate Professor, Teaching Stream and Vice Dean of Education at the Faculty of Dentistry, University of Toronto. He can be reached at jimyuan.lai@dentistry.utoronto.ca
 Ryan Schure is a periodontist practicing in Toronto, ON. He is an Assistant Professor and Director of the Undergraduate Periodontology program at the Faculty of Dentistry, University of Toronto. He can be reached at ryan.schure@dentistry.utoronto.ca.
Ryan Schure is a periodontist practicing in Toronto, ON. He is an Assistant Professor and Director of the Undergraduate Periodontology program at the Faculty of Dentistry, University of Toronto. He can be reached at ryan.schure@dentistry.utoronto.ca.










