
These are exciting times in dentistry. We have technology available today which allows us to complete dental surgery with greater precision and more comfort for our patients than we ever could before. More and more general practitioners are performing what used to be considered complex surgeries, previously reserved only for the specialists, on a daily basis in their own clinics. This is not to say that we are not grateful for our specialists, but rather there is a new field within dentistry, though still in its infancy, and that is Dental Sleep Medicine (DSM).
Have you heard the quote by D.H. Lawrence, “What the eye doesn’t see and the mind doesn’t know, doesn’t exist”? How many patients did you see today, this week, this month or this year? And how many of those patients did you identify as having a potentially life-threatening condition that they were unaware of? Statistics consistently validate that somewhere within the range of 20 to 25% of patients have Obstructive Sleep Apnea (OSA). It is estimated that 85-90% of the patients with OSA remain undiagnosed1, and that it can take an average of 12 years off of one’s life expectancy, and causes more motor vehicle accidents than drunk driving.2 Furthermore, an even greater number of your patients are trying to get through their days while suffering from an unrecognized Sleep Disordered Breathing (SDB) issue, presenting as snoring and upper airway resistance syndrome (UARS) or OSA. The SDB issue is defined as fragmented sleep causing people to experience excessive daytime sleepiness, chronic fatigue, and lack of refreshing sleep even after being in bed for the recommended amount of time. The lack of quality dream sleep is now being recognized as important for one’s ability to process and store long term memory as well.3 Combine all of these with the number of known correlated health issues, including cardiovascular disease and cerebrovascular disease, and we can begin to understand the importance of getting a good night’s sleep.
Unfortunately, a majority of dentists are not well versed in sleep medicine and sleep-related disorders, and have yet to learn the systemic and oral risks of OSA, which they are encountering each day in their own patient population.1 Dentists, who are trained to screen for snoring and OSA, can provide a life-changing service for their patients. In addition to helping them identify an unknown problem, dentists can also provide a mandibular advancement device (MAD), for the management of SDB, and thus improve their patients’ overall health and longevity.
We are able to discover a medical condition that can have a dental solution, but the disconnect between physicians and dentists is creating numerous obstacles.1 We understand that PAP (positive airway pressure) machines, provided by our medical colleagues are an effective way to manage OSA, but we also can infer that many patients are far from compliant with this form of therapy. In the same breath, we know that MADs can be less effective than CPAP at reducing the Apnea-Hypopnea Index (AHI), the metric for grading the severity of OSA.
Public and private healthcare insurance providers separate their Dental and Medical funding, which makes getting paid for providing this service to your patient very challenging. Dentists are not typically proficient at communicating with physicians and, unintentionally or due to the lack of knowledge and training, fail to follow the recommended Sleep Medicine treatment protocols. The diagnosis of OSA must come from a board-certified sleep physician, whom are few and far between amongst all of the medical specialties. Only dentists trained in managing SDB are qualified to fabricate, deliver, titrate and follow-up with oral appliance therapy (OAT).
It is important for dentists, whom are new to the practice of DSM, to understand that they should not fabricate anti-snoring appliances for those patients exhibiting snoring symptoms, as 70% are likely to have OSA.1 Patients with significant snoring must be tested and diagnosed by a sleep physician. Only for those found not to have OSA, is a MAD truly just a “snoring appliance.”
In each and every day of practice, you look into someone’s mouth – but what was the first thing you examined? Most likely, it was the teeth or the periodontium, which was the exact same thing that I did before I focused on DSM. I challenge you to change the way you look into someone’s mouth, and know you will be shocked at what you begin to see. You will start to recognize things which have eluded you for way too long. I challenge you to look past the teeth and gums, and examine first the patient’s oropharynx, their throat, or call it their airway (Fig. 1). Is their tongue blocking it, and can you see the uvula, or are their palatine tonsils swollen? Is there redness of the soft tissues, and does the tongue rest in the floor of the mouth, functions correctly, and able to be elevated to the roof of the mouth from tip to base? Do the teeth exhibit wear from GERD (Fig. 2)? To me, it is more important to be able to address the patient’s ability to breathe, than it will ever be to fix another cavity, manage periodontal disease, or extract an impacted tooth.
Fig. 1

Fig. 2

It is well documented that we clench and grind our teeth when we are stressed4, however, have you ever considered that the stress may be caused by the inability to breathe easily? I call it physiologic stress, but never gave it much thought until within the last few years. My lightbulb moment happened when someone explained this to me at a dental conference and, all of a sudden, all those numerous broken teeth, failed restorations and severely worn dentition, which I had observed on a daily basis over the 25 years, began to make sense.
When we reach our deepest stages of sleep, we lose all control of our musculature. Imagine how limp a sleeping child is when carrying them to bed, and you will understand loss of muscle tone. Couple loss of tone with perhaps one or more of the following, such as a few extra pounds around the neck, narrowed maxilla, mandibular crowding, enlarged or scalloped tongue, blocked nasal passages, deviated septum, swollen tonsils, or adenoids, and soon you will see how easy it is for one to have obstructed airway.
Studies have shown that we clench and grind our teeth while sleeping in order to regain control of the muscles supporting the soft tissues around our airway, following an event that disturbs our respiration, and subsequent drops blood oxygen levels, which increases our heart rate and blood pressure.5 We subconsciously position our mandible into the most airway-favourable position to regain the necessary physiologic environment to sustain life, which typically is a protrusive one, forward of our maximum intercuspation. This position is often end-to-end, or even slightly beyond, which presents as anterior teeth wear and the appearance of craze lines (Fig. 3). This anterior position also results in an increased vertical dimension allowing more space (a larger box) for the tongue, aiding an increase in the potential airway volume.
Fig. 3

Historically, with this type of teeth wear, we were taught to make an occlusal guard to protect the teeth and our dental restorations, and have likely proceeded as such, and many times, without any respect for a potential underlying and undiagnosed medical condition of OSA. These occlusal guards, when made without proper diagnosis, can place our patients at greater risk of suffering the effects of a collapsed airway during their use. They eliminate the natural defense system of intercuspation and remove the interferences, thus allowing the mandible to drop back, and taking the tongue with it into the oropharynx, resulting in an obstructed airway.
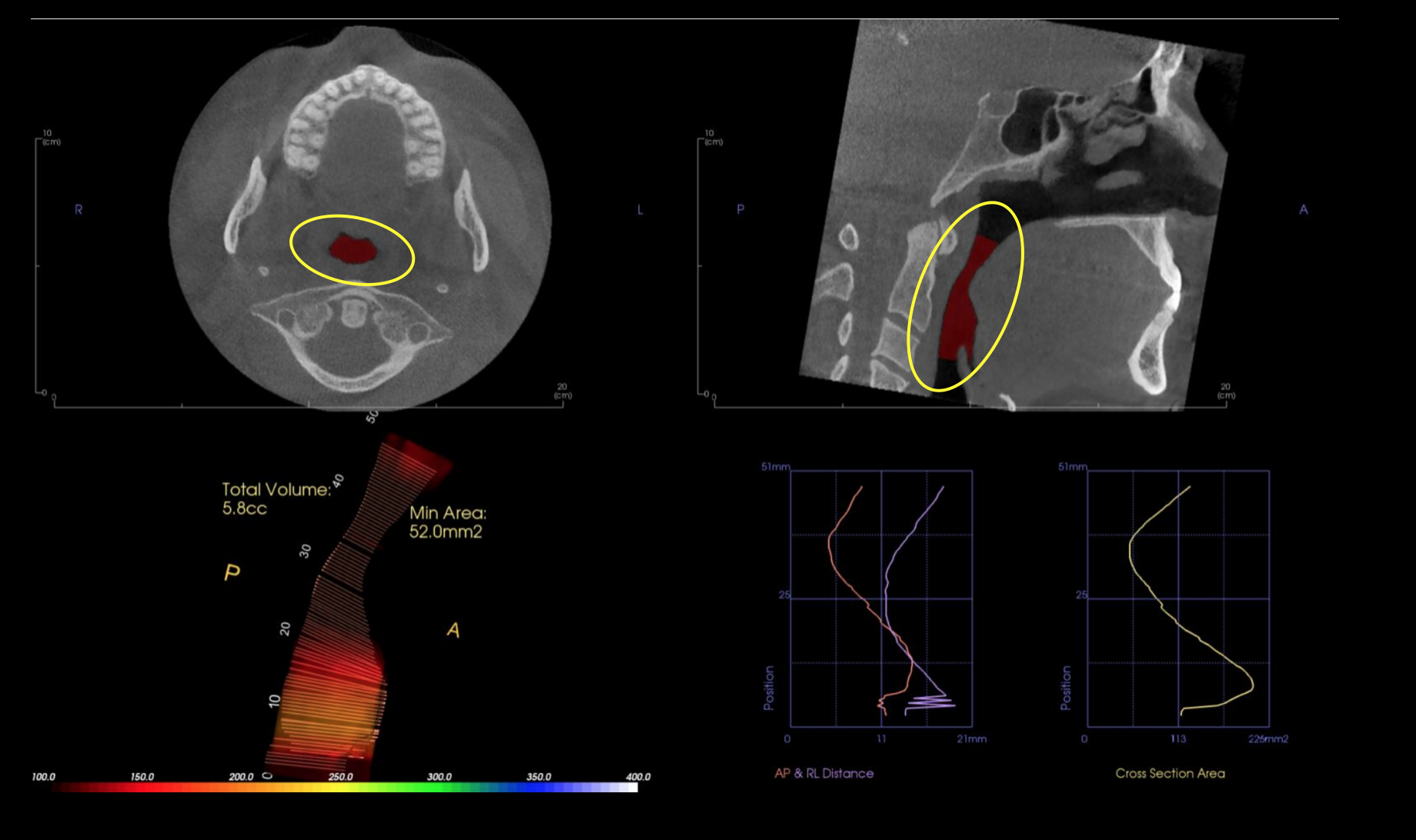
Today, many dentists have digital imaging capability in their clinics, such as CBCT imaging which, unlike panoramic radiography, gives us an accurate and undistorted image of the nasal passages and TMJ’s (Fig. 4). CBCT, while valuable in the management of SDB and TMJD, is not considered diagnostic for OSA because the patient is usually in an upright position and awake during the scan. However, these images, as presented on a screen, can be powerful adjuncts to patient communication and visualization of the problem being addressed. They help shed light on many undiagnosed issues with the TMJ’s, which can and will present themselves with mandibular advancement therapy.
Fig. 4
The easiest way to get started is to begin asking your patients if they know someone who snores, as those who do are obviously already asleep and usually unaware of its severity. Snoring is less of a relationship problem for the person who does snore, than for those trying to sleep next to them. You will get more referrals from disgruntled partners than any other source, I promise. Next, ask them if they feel tired or awaken unrefreshed in the morning, or if anyone has ever observed them stop breathing during sleep.
Begin to understand the clues from your patient’s medical history (Fig. 5), such as hypertension, stroke, diabetes, GERD, or awakening with headaches, and are they obese. Neck size measured at more than 17″ in males, and 15″ in females, increases the risk of having OSA; so, do those over 50 years of age. If you are a male, and over 50, then you have two strikes against you.
Fig. 5

These signs are referred to as a STOP-BANG assessment and, of course, like most of our teachings in dentistry, is an acronym to make it easy to remember:1
- Snores
- Tired
- Observed stopped breathing
- Pressure (HBP)
- BMI
- Age
- Neck size
- Gender
If I could only remember one point in this article, it should be that dentists are perhaps, at the same time, the best and the worst people to manage patients with SDB. Dentists see the signs of SDB daily, but they typically haven’t been educated as to the life-threatening root cause of what they are observing. These findings are so common, and have been ignored for so long, that they are often considered within normal limits. We also put too much emphasis on choosing the right dental device, making it fit precisely to the teeth with minimal discomfort, and fabricating it in the optimal condylar position right from the start of therapy. Too many dentists are attempting to make these devices without completing post-insertion titration visits, which are used to find the most medically beneficial jaw position. We are implementing OAT without providing minimal follow up and continuing care visits to assess the patient’s compliance and effectiveness of this therapy. Dentists tend to be super analytical, by nature, and take it personally when their device fails to achieve their intended goals.
Getting involved in DSM requires a shift in the dentist’s mindset, which in medical terminology, is referred to as utilizing “medical decision-making.” Patients must be assessed for their willingness to adhere to MAD therapy and allow the physiologic data acquired during therapy to guide their actions. Managing OSA may also involve nasal breathing instruction, positional therapy, weight loss, exercise, addressing side effects, and other issues which require collaboration with other healthcare professionals, in order to achieve a successful outcome.6 Management of a patient’s airway is critical for their overall long-term health, but also for the longevity of their dental health.
Oral Health welcomes this original article.
References
- Berley, K. and Carstensen, S. 2019. The Clinician’s Handbook for Dental Sleep Medicine. Quintessence Publishing.
- Wick, S. 2016. Kicking the Bear Out of the Bedroom. Published by Steve Wick.
- Walker, M. 2017. Why We Sleep. Unlocking the Power of Sleep and Dreams. Scribner.
- Park, S. 2008. Sleep Interupted. Jodev Press
- Klasser, G. Rei, N. Lavigne, G. 2015. Sleep Bruxism Etiology: The Evolution of a Changing Paradigm. J Can Dent Assoc, 81, f2.
- Gelb, M. Hindin, H. 2016. GASP: Airway Health, The Hidden Path to Wellness. Published by Michael Gelb and Howard Hindin.
About the Author
 Dr. Jeffrey Harrison is the Founder of Colorado Laser Dentistry and is currently the President of Sleeping Giant Sleep Solutions. He is a graduate of the University of Missouri–Kansas City, School of Dentistry, and currently practices in Steamboat Springs, Colorado, where he runs a private practice exclusively dedicated to identifying and managing Sleep Disordered Breathing issues for his patients.
Dr. Jeffrey Harrison is the Founder of Colorado Laser Dentistry and is currently the President of Sleeping Giant Sleep Solutions. He is a graduate of the University of Missouri–Kansas City, School of Dentistry, and currently practices in Steamboat Springs, Colorado, where he runs a private practice exclusively dedicated to identifying and managing Sleep Disordered Breathing issues for his patients.










