
Do you ever request your patients to close on the saliva ejector to evacuate fluids from their mouths? If so, when was the last time you effectively cleaned out the valve? When a patient closes on the saliva ejector or the tip becomes occluded, backflow may occur due to a temporary drop in vacuum pressure. Saliva ejector backflow has been proven to potentially occur in an estimated 21-25%, as studied by the University of Montreal in 1998. 1 These studies indicated water contamination containing bacterial levels ranging from 1 CFU to 300 CFU* per occurrence. [*CFU (cfu or cFu) is defined as colony forming units in microbiology used to estimate the number of viable bacteria or fungal cells in a sample.] More plainly stated, one in five patients may receive the backwash in their mouths from the last patient. Think of how many times you ask your patient to “close”? That is a lot of bacteria!
This backflow problem is not new. University of Alberta had published articles in 1993, documenting the backflow issue and the potential pathogens present in the water from the saliva ejector backflow. 2,3 Bacteria isolated from these samples include staphylococci, micrococci, Pseudomonas aeruginosa, Staphylococcus aureus, Legionella pneumophila and nonfermentive Gram-negative rods. 4,5,6 These bacteria are consistent with the bacteria found in dental unit waterline biofilm. 7,8
Biofilm in our waterlines has taken a front row seat in infection control. The concern is the biofilm growing in our water lines. The CDC has defined biofilm as: Biofilm is a thin, slimy film of bacteria that sticks to moist surfaces, such as those inside dental unit waterlines. Biofilm occurs in dental unit waterlines because of the long, small-diameter tubing and low flow rates used in dentistry, the frequent periods of stagnation, and the potential for retraction of oral fluids. As a result, high numbers of common water bacteria can be found in untreated dental unit water systems.
Regular disinfection of waterlines should be a component of infection control protocols for the office. Risk of infection, especially in immunocompromised patients, is a possibility. An 83-year-old woman in Italy died from the Legionnaires disease after being treated at a dental office. In February 2011, the woman was admitted to the hospital with a fever and respiratory distress, which quickly denigrated to septic shock and she passed away within two days. The Legionella strain found in the dental water lines matched what was found in the patient. 10,11
The possibility of cross contamination due to this backflow is a constant potential risk. The U.S. Centers for Disease Control and Prevention advises that dental patients not be instructed to close their lips around the SE tip when it is in use. 12 As with the dental waterlines, saliva ejector and HVE 13 tubing contain bacterial biofilms that may create an infection. Although these studies did not provide direct proof of cross-contamination, they suggested an infectious risk since a reservoir of pathogens may be given off from tubing biofilms.
The method to prevent this backwash of fluids from occurring is to have a backflow prevention valve in place. Manufacturers have anti-retraction devices placed on handpieces, so residual bacteria are prevented from going back down into the handpiece after each use. They also have specifications for cleaning and maintaining their evacuation equipment.
What do offices do to disinfect their evacuation devices? Some offices cover their HVE and saliva ejector with a plastic sheath (Figs. 1 & 2) Most wipe the used saliva ejector and HVE with a disinfectant after each patient encounter. Some use evacuation enzymatic cleaners to flush the lines 14 (Table 1). Instructions for use are included with each manufacturer’s product. Protocols are slightly different for each, but they should be followed to achieve optimal efficiency and outcomes. All standard HVE and Saliva Ejector Valves contain up to three O-rings (Fig. 3). When the O-rings are not lubricated, changed, and inspected, they result in leaking and or dripping (Fig. 4). Leakage frequently occurs when the parts stick and are not free moving due to all of the debris that is not routinely cleaned. All recommend daily flushing of the suction lines. These protocols assist in the free-flowing capabilities of the tubing, but do little to truly remove the biofilm risk and cross contamination. Though manufacturers’ recommendations should be followed, protocols vary on each office: some flush after each patient, at the end of the day or at the end of the week.
Table 1

Fig. 1

Fig. 2

Fig. 3
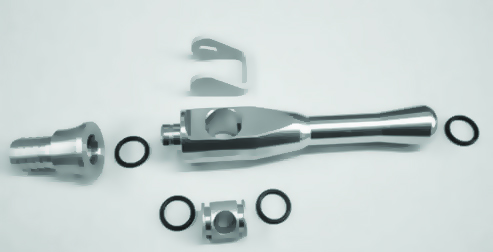
Fig. 4

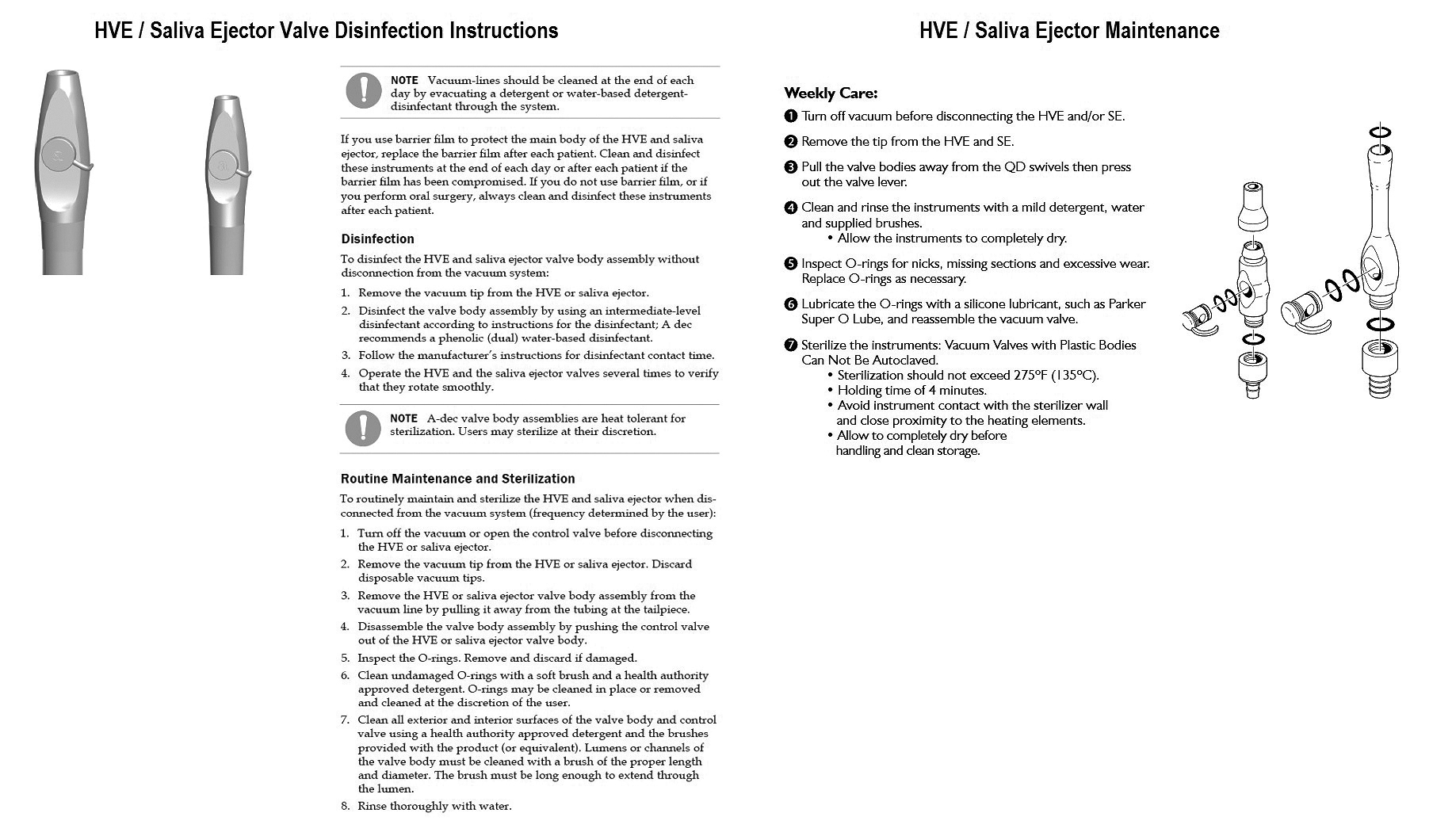
As we receive instructions for use (IFU) for any dental material or other product in our offices, these integral components of our operatory also have instructions for maintenance. Each suction and HVE component comes with an instruction sheet, detailing the precise method for disassembling the piece and cleaning it. O-rings need to be maintained, cleaned and lubricated for proper seal. Some of the valve bodies are autoclavable. Recommendations are offered for daily and weekly maintenance, including changing the screen inside the saliva ejector as well as the HVE. Please see a sample below of HVE maintenance, which is the A-Dec recommendation, provided with all new equipment (Fig. 4).
These are critical procedures, not only to improve the flow and operability of the saliva ejectors and HVE, but to decrease the potential of cross contamination from backflow and valve leakage. They are also time consuming. Another, simpler method of prevention is to use disposable products. As we have many single use products in our practices, these disposable valves and attachments would be an additional safeguard to break the link of potential cross contamination occurrences.
Currently, two companies manufacture disposables on the market that prevent backflow. One is a complete valve replacement system and one is a modification of existing saliva ejectors and HVE attachments.
Dove® is a single use product, available for both saliva ejectors and HVE, replacing the current metal valve on the tubing. The Dove® saliva ejector and HVE valves only allow for one-way flow or suction, and an internal flap prevents any opportunity for backflow of oral fluids. Dove® valves offer a complete valve replacement. The Dove® valves contain an on/off lever, which allows for the replacement of the current metal valves. Since no O-rings are used, there is no concern about leakage from the metal valves in the form of a bubble or leaky drip that often occurs when the valves have not been properly maintained. Each valve alleviates the multiple steps required to clean metal HVE and saliva ejector valves. Any saliva ejector, HVE or aspirator tip on the market can be inserted in the Dove® valve. Dove® valves address backflow and guarantee every valve is clean, safe and works perfectly for each patient. Once the procedure is complete, the entire unit, disposable saliva ejector or HVE valve, are disposed in the appropriate methods. These valves are time saving, as no maintenance is required for O-rings. Dove® makes their valves to fit almost 99% of all dental unit tubing.
Crosstex SAFE-FLO® Saliva Ejector products all contain unique one-way internal backflow prevention providing a barrier that prevents the fluids from the tubing to enter back into the patient’s mouths. The SAFE-FLO® HV internal valve closes when the suction is stopped or restricted and prevents backflow. The SafeFlo® saliva ejector and HVE functions as a single use saliva ejector or HVE and are inserted into current metal valves in your system. Both HVE and saliva ejector metal valves still require the multiple steps to clean. Only disassembling and reprocessing will guarantee the metal valve to be for every patient as per the instructions for use. The SafeFlo® products do not address leakage that often occurs between connections, as they are inserted into the metal valve. Crosstex SafeFlo® products include saliva ejectors that may be used with your existing metal valves, or a protection adapter device that connects into your existing metal saliva ejector or HVE valve. Crosstex SafeFlo® does not have an on/off switch, therefore the metal valves must be maintained, as per manufacturer recommendations.
With both systems, it is still important to follow manufacturers’ recommendation for flushing and maintaining the suction lines. Suction lines should be cleaned every day to remove bio burden. Just as with your waterlines, a shock treatment should be done periodically, along with the daily maintenance. Disposable saliva ejector screens should be changed weekly, or sooner if clogged with large chunks of calculus or restorative debris from a single patient (Fig. 6). Tubing should be replaced periodically. Examine tubing for breaks or tears. Unaesthetic, dirty or discolored tubing affects the clean visuals in your office.
Fig. 5
*Click to view larger image
Fig. 6

Our offices are so aware of the infection control standards, including disinfecting countertops, sterilizing instruments and discarding disposable items from our procedures, such as saliva ejectors and HVE, though we may have missed one area where cross contamination may occur. We believe every patient should be provided a clean safe valve. To do this, offices should either follow the instructions for use or consider disposables as they are the emerging trend to alleviate cross contamination risk, alleviate backflow, alleviate leakage and guarantee every patient has a safe clean valve while saving valuable time. By this method, we close off the potential backflow and cross contamination from bacteria and virus’ that build up in the valves and tubing. With these disposable valves, we eliminate the risk of backflow and ensure each patient received the cleanest possible dental visit.
Disclaimer
The author has received material support from Dove Dental Products.
References
- Mann GL, Campbell TL, Crawford JJ. Backflow in low-volume suction lines: the impact of pressure changes. J Am Dent Assoc. 1996;127:611-615.
- Watson CM, Whitehouse RL. Possibility of cross-contamination between dental patients by means of the saliva ejector. J Am Dent Assoc. 1993;124:77-80.
- Whitehouse RL. Danger of inter-patient cross-contamination from saliva ejector suck back. J Can Dent Assoc. 1996;62:499-500.
- Barbeau J, ten Bokum L, Gauthier C, Prévost AP. Cross-contamination potential of saliva ejectors used in dentistry. J Hosp Infect. 1998;40:303-311.
- Barbeau J, Gauthier C, Payment P. Biofilms, infectious agents, and dental unit waterlines: a review. Can J Microbiol. 1998;44:1019-1028.
- Meiller TF, Depaola LG, Kelley JI, Baqui AA, Turng BF, Falkler WA. Dental unit waterlines: biofilms, disin fection and recurrence. J Am Dent Assoc. 1999; 130:65-72.
- Costa, D., Mercier, A., Gravouil, K., Lesobre, J., Delafont, V., Bosseau, A., Verdon, J., Imbert, C. Pyrosequencing analysis of bacterial diversity in dental unit waterlines Water Research V81, September 2015, pp 223-231 https://doi.org/10.1016/j.watres.2015.05.065
- Singh, R. et al Microbial Diversity of Biofilms in Dental Unit Water Systems Appl Environ Microbiol. 2003 Jun; 69(6): 3412–3420
- Barbeau J, ten Bokum L, Gauthier C, Prévost AP. Ibid
- Ricci, ML. et al. Pneumonia associated with a dental unit waterline. Lancet. 2012 Feb 18
- Atlas R, Williams J, Huntington M. 1995. Legionella Contamination of Dental Unit Waters. Applied and Environmental Microbiology 61; 1208-1213.
- Guidelines for infection control in dental health-care settings, 2003. Centers for Disease Control and Prevention. https://www.cdc.gov/mmwr/preview/mmwrhtml/rr5217a1.htm. MMWR 2003;52(RR-17):1-61. Published December 19, 2003.
- Miller, Chris. Back flow in low-volume suction lines may lead to potential cross- contamination RDH January 1996
- Givoni, Mary Cleaning or disinfection: What’s right for the suction lines? Dental Economics March 2013 https://www.dentaleconomics.com/articles/print/volume-103/issue-3/practice/cleaning-or-disinfection-whats-right-for-the-suction-lines.html
About the Author
 Sheri practices clinical dentistry in Lincolnwood, IL. Her book, “Practical Practice Solutions in Dentistry” focuses on building practice success. She has served as an educator in several dental and dental hygiene programs, has been a consultant for a major dental benefits company, speaks internationally on a myriad of topics, and writes for several dental publications. She is a member of the American Dental Association, Illinois State Dental Association, Chicago Dental Society, a Fellow in the American College of Dentists, a Fellow in the International College of Dentists and a past president of the American Association of Women Dentists. You can reach her at donigerdental@aol.com.
Sheri practices clinical dentistry in Lincolnwood, IL. Her book, “Practical Practice Solutions in Dentistry” focuses on building practice success. She has served as an educator in several dental and dental hygiene programs, has been a consultant for a major dental benefits company, speaks internationally on a myriad of topics, and writes for several dental publications. She is a member of the American Dental Association, Illinois State Dental Association, Chicago Dental Society, a Fellow in the American College of Dentists, a Fellow in the International College of Dentists and a past president of the American Association of Women Dentists. You can reach her at donigerdental@aol.com.











