
Non-surgical endodontic therapy requires access preparations that uncover entrances to the labyrinthine tunnels of the root canal system. The era of bio-minimalism has altered the traditional configuration of endodontic access cavities. These bio-minimalistic trends are also transforming endodontic surgery. 1 The use of surgical operating microscopes (Global Surgical Corporation, St. Louis, MO) facilitates smaller crypt sizes and reduces the volume of bone removed. The wound architecture created by micro-surgical scalpels (Kerr Corporation, Orange CA) is more precise resulting in minimal damage to the soft tissues. 2 Enhanced visibility facilitates perpendicular resection of the apical segment to the long axis of the root. Monofilament sutures (Johnson & Johnson – Ethicon Cinncinnati OH) minimize post-treatment inflammation. Soft and hard tissue augmentation corrects deficits in biotype and buttressing bone. These are but a few of the new adjuncts in endodontic microsurgical techniques. 3-5
Ultrasonic Osteotomy
Used in both periodontal and implant surgery, piezo surgery in microsurgical endodontics produces micrometric cuts which diminish cortical bone loss and retain root length. Saline pumped through irrigation lines cools the piezotome tip (NSK America Corp IL, Brasseler USA, Savannah GA) (Fig. 1). In deep spaces, ultrasonic vibrations break down the irrigation into very small particles readily suctioned from the surgical field. Reduction of heme in the crypt minimizes the use of hemostatic agents and interference with the setting of retro-seal materials. The inclusion of piezo surgery in endodontic microsurgical protocols produces less morbidity during the healing phase.
Ultrasound consists of mechanical waves of frequencies greater than 20 kHz. Generated by transducers (Lead Zirconate Titante), electrical energy is converted to ultrasonic waves with minimal heat production. The clinician controls the pressure applied, cutting frequency, pulse frequency, rate of delivery of coolant fluid and power (3-90 W). Minimal heat generation on cutting creates lower pro-inflammatory cytokine levels, an earlier increase in BMP4 and TGF2 and more active neo-osteogenesis. 6-7
Traditional osteotomies require large instruments to remove cortical bone in order to access the apical segment of the root. These instruments can lead to delayed healing, increased post-operative pain and/or complications. With microscopes and piezotome surgical tips, smaller osteotomies (less than 5 mm) are big enough to accommodate ultrasonic tips (tip length of 3 mm).
Fig. 1
Piezotomes with fine-toothed saws tips of 8 and 10 mm length create smaller osteotomies and minimal osseous trauma (NSK America Corp IL, Brasseler USA, Savannah GA).

Fig. 2A
Cone beam tomography facilitates measurements of crypt dimension in sagittal, axial and coronal views (x, y, z axes).

Fig. 2B
Proximity to the inferior alveolar nerve can be calculated. This is a crucial measurement in all microsurgical procedures.

Cortical Window Technique
Dental radiographs are essential to all aspects of endodontics. Historically, they were two-dimensional images of three-dimensional structures; as such, data interpretation was subjective. The introduction of cone beam computed tomography (CBCT) and digital volume technology (DVT) provides images in sagittal, axial and coronal planes showing previously indeterminable views. 8,9 The three-dimensional data gathered from the CBCT scan allows a pre-planned window to be made to access the apical portion of the roots. The use of CBCT imaging in conjunction with piezo surgery provides a precise and less traumatic outline for the cortical bone window in contrast to traditional free-hand guided crypt creation. The cortical bone window is sectioned so that the facial or palatal wall converges from the external surface to the internal surface. This ensures accuracy of removal of the cortical bone plate and re-seating when the window is replaced.
Case Report
A female patient was seen for consultation regarding tooth #3.6. She reported that pain on biting had developed over the past week and intensified day to day. Her generalist took a periapical radiograph and advised the patient that “something” was amiss. A prescription for Amoxicillin (500 mg) was provided and she was referred to our office. Tooth #3.6 was percussion sensitive. A two-dimensional radiographic examination revealed a prior root canal procedure, a PFM crown and cast post core in the mesial-buccal and distal canals. The suggestion of a second distal canal was noted (Fig. 3).
A cone beam tomography scan was recommended as the tomographic volumes would elicit more accurate diagnostic information; the patient concurred, and was referred to a dental radiologist (www.canaray.com). The CBCT (Fig. 4) showed that the apex of the distal root demonstrated rarefying osteitis. In addition, the apical third of the distal root was under-instrumented and under-filled which contributed to persistent apical pathology. The mesial root appeared normal radiographically. Retreatment as an option was discussed, however the risk factors involved, removal of the crown/post core and retreatment of the root canal system, were deemed have an uncertain prognosis. Other options were discussed including consideration for extraction and implant replacement. The patient agreed to have microsurgical treatment using a cortical bone window access – a sagittal view (CBCT) was used to determine the width and height of the cortical window needed (Fig. 2A). The coronal view shows the facial lingual width and the position of the inferior alveolar nerve (Fig. 2B) – the relation of the lesion between facial and lingual cortical place determines depth of the surgical crypt and the its proximity to the inferior alveolar nerve. The clinical examination identified generalized recession and diminished attached gingiva about the facial aspect of #3.4 and the mesial root of #3.6 (Fig. 5A).
Anesthesia was obtained using Xylocaine 2% with epinephrine 1:100,000 (Dentsply Sirona Canada Ltd.) for the IAN (inferior alveolar nerve) and Xylocaine 2% with epinephrine 1:50,000 (Dentsply Sirona Canada Ltd.) was used for regional infiltration. A Surgical Operating Microscope was used, the principles of modern microsurgical endodontics6 were applied. A full thickness intra-sulcular flap was incised with a microsurgical blade, which minimizes trauma and loss of the interdental dental papilla especially in areas of recession and thin biotype (Fig. 5B). The piezotome was used to cut the cortical window. The cortical window was angled convergent from the external surface to the internal surface and wider at the base which prevents the plate from sinking internally when repositioned as discussed previously (Fig. 6).
Fig. 3
Tooth #3.6. All canals are under-instrumented and demonstrate obturation density deficit. Retreatment of the tooth would necessitate removal of the cast post core which could lead to fracture of the mesial and distal roots.

Fig. 4
The cbCT demonstrates a more definitive extent of the pathology. A sagittal view (CBCT) was used to determine the width height of the cortical window required. The window cut is angled convergent from the external to the internal cortical plate, the base larger apically than coronally thus preventing the bone segment from collapsing into the crypt when replaced.

Fig. 5A, 5B
The flap is designed to correct the areas of recession. Vertical and horizontal incisions present pressure of the flap on retraction, the roots were planed to ensure a clean surface enhancing improved adherence of flap to the root.


Fig. 6
The piezotome (NSK VarioSurg 3 1800 Global Parkway Hoffman Estates, IL 60192, USA) creates an osseous window that will be replaced after completion of the root end surgery.

The window was removed by luxation (Fig. 7) from a thin chisel and placed in sterile saline. The apices are resected preserving root length exposing the lingual anatomy, centering the canals, eliminating accessory canals and minimizing the number of exposed dentinal tubuli. The canal is retro-prepared (ProUlltra tips Dentsply-Sirona, York PA) retro-sealed using Super EBA™ (Keystone Dental, Inc, USA)10 (Fig. 8).
The crypt is filled with freeze dried allograft (0.5 cc Mineralized Cortical GC, Straumann Canada Ltd. Burlington, ON) (Fig. 9). The cortical window is replaced (Fig. 10) and the wound (flap) sutured using 6-0 prolene sutures (Ethicon) (Fig. 11). The post-operative radiograph is shown (Fig. 12). The reassessment radiograph taken six months later demonstrates almost complete osseous regeneration (Fig. 13). The patient is asymptomatic, the procedure has retained substantial root length and a long-term positive treatment outcome is expected (Fig. 14).
Fig. 7
The cortical window was removed with a fine chisel.

Fig. 8
A truss is retained between the two roots to expedite osseous regeneration. The retroseals (Super EBA) are burnished and the root face polished with a multi fluted carbide bur.

Fig. 9
Allograft is placed in the crypt.

Fig. 10
The cortical bone plate is replaced over the access window.
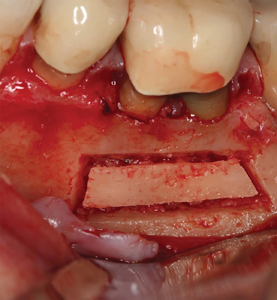
Fig. 11
The flap is co-apted and sutured to place. Note that the areas of recession are covered with tissue.

Fig. 12
Post treatment radiograph.

Fig. 13
Six-month recall appointment shows healing to be almost complete.

Fig. 14
Six month follow up showing clinical healing and healthy tissue response.

Conclusion
The basic framework of endodontic surgery by incorporation of interdisciplinary precepts has evolved into endodontic microsurgery. The benefits of this cortical window approach include greater access the roots for better visibility without greater risk for bone loss. The minimally invasive approach to access the roots by way of removal of a cortical bone plate has its greatest advantage simply due to the fact that the bone plate is conserved and then replaced, allowing maximum regenerative potential. Advances in the surgical armamentarium, based on biological concepts has enabled a microsurgical approach which ensures enhanced positive treatment outcomes. The past is not being rejected; the future is being embraced. It is the natural progression of all things. OH
Oral Health welcomes this original article.
References
- Wang N, Knight K, Dao T, Friedman S. Treatment outcome in endodontics: the Toronto Study. Phases I and II: apical surgery. J Endodon March 2004;30(11):751– 61
- Tsesis I, Rosen E, Taschieri S, et al. Outcomes of surgical endodontic treatment performed by a modern technique: an updated meta-analysis of the literature. J Endodon March 2013;39(3):332–9
- Tsesis I, Rosen E, Taschieri S, et al. Outcomes of surgical endodontic treatment performed by a modern technique: an updated meta-analysis of the literature. J Endodon March 2013;39(3):332–9
- Kim S, Kratchman S. Modern endodontic surgery concepts and practice: a review. J Endodon July 2006;32(7):601–23
- Setzer FC, Kohli MR, Shah SB, Karabucak B, Kim S. Outcome of endodontic surgery: a meta-analysis of the literature – Part 2: Comparison of endodontic microsurgical techniques with and without the use of higher magnification. J Endod. 2012 Jan;38(1):1-10
- Vercellotti T. A. Essentials in piezosurgery: Clinical advantages in dentistry. 1st edition Quintessence Publishing Co., December 2009
- Abella F, de Ribot J, Doria G, et al. Applications of piezoelectric surgery in endodontic surgery: a literature review. J Endodon March 2014;40(3):325–326
- Venskutonis T, Plotino G, Juodzbalys G, et al. The importance of cone-beam computed tomography in the management of endodontic problems: a review of the literature. J Endodon December 2014;40(12):1895–1901
- Leonardi Dutra K, Haas L, Porporatti AL, et al. Diagnostic accuracy of cone-beam computed tomography and conventional radiography on apical periodontitis: a systematic review and meta-analysis. J Endodon March 2016;42(3):356–64
- Sullivan JE, Di Fiore PM et al. Super-EBA as an Endodontic Apical Plug. J Endodon August 1999;25(8):559-561
About the Authors
 Naheed Mohamed DMD, MSD, Dip Perio, DABP, FRCD(c) is a board-certified periodontist and Diplomate of the American Academy of Periodontology. He is a partner in a group periodontal practice in Mississauga and maintains his own private practice in Oakville. He can be reached at naheedm@gmail.com.
Naheed Mohamed DMD, MSD, Dip Perio, DABP, FRCD(c) is a board-certified periodontist and Diplomate of the American Academy of Periodontology. He is a partner in a group periodontal practice in Mississauga and maintains his own private practice in Oakville. He can be reached at naheedm@gmail.com.

Dr. Yosef Nahmias was born and raised in Mexico City. After he graduated from the Universidad Tecnologica de Mexico, School of Dentistry, in 1980, he decided to advance his education and chose Endodontics as his specialty. Dr. Nahmias earned his Master’s of Science degree in Endodontics in 1983 at Marquette University in Milwaukee, Wisconsin. He has authored many articles and continues to lecture in Canada and internationally. Dr. Nahmias has been a practicing Endodontist in Oakville, Ontario since 1983. He can be reached at yosi@allianceds.com.

Ken Serota graduated from the University of Toronto Faculty of Dentistry in 1973 and received his Certificate in Endodontics and Master of Medical Sciences degree from the Harvard-Forsyth Dental Center in Boston, Massachusetts. Active in online education since 1998, he is the founder of the online forums ROOTS and NEXUS. Dr. Serota is a clinical instructor in the University of Toronto postdoctoral endodontics department.
RELATED ARTICLE: The Cortical Window: Part Two Computer Guided Endodontic Surgery (CGES)
Follow the Oral Health Group on Facebook, Instagram, Twitter and LinkedIn for the latest updates on news, clinical articles, practice management and more!










