
As a child growing up in the sixties, I was a great fan of the famous “Star Trek” television show starring William Shatner. The original series debuted on September 8, 1966. The show tells the tale of the crew of the starship Enterprise and its five-year mission “to boldly go where no man has gone before”. Having practiced Endodontics since 1983, my journey in this specialty has been as equally exciting as the voyages of the Enterprise. I have seen and witnessed many changes. Such as; the use of warm Gutta-Percha techniques, the introduction of Apex Locators, Ultrasonics for conventional and surgical Endodontics, the use of the Operating Surgical Microscope, the NiTi revolution for shaping canals, and most recently the use of CBCT technology for endodontic diagnosis and treatment planning. I not only have been fortunate to see so many changes, but privileged to participate by lecturing and publishing on most of these exciting innovations.
Recently a new device has been introduced in the field of Implantology. This new technology is known as The Dynamic Dental Navigation System.1 Prior to the introduction of this technology, a static guide (CAD/CAM), using a prefabricated stent based on a CBCT scan was manufactured to guide the surgeon in the safe placement of the implant.2 These guides in addition to being expensive, need to be fabricated ahead of time and cannot be altered after fabrication. We published an article on the use of these guides for the creation of a window for apical surgery.3 In contrast however, Dynamic Navigation uses a stereoscopic tracking camera to dynamically guide the operator’s instruments to the correct location for the implant placement in real time.
With the introduction of the Navigation System for the placement of dental implants, it has been claimed that the dentist can then place the implant both accurately and precisely.4 In addition, a clear advantage of the Dynamic Navigation System is the considerable cost saving to the patient as the static guides do not have to be fabricated. The cost of these guides can range from $300 to over $1,200 depending on the complexity of the case.
Furthermore, Dynamic Navigation has been reported to be more accurate than free-hand placement of Implants.5
Dr. David Burgess describes this technique as “just like a GPS guides drivers”. He lists several advantages such as accuracy in placing the implants, improved safety and aesthetics, minimally invasive, less patient discomfort and faster recovery time.6
It was only a matter of time before this technology came to the attention of the endodontist and could be uniquely suited for the treatment of complex cases both conventional and surgical. When faced with calcified canals, multiple canals, difficult to locate canals and unusual canal anatomy on a daily basis this system could be used for finding and successfully treating these canals in a safe and predictable manner. In addition, this technology potentially can be used to make smaller, less invasive access preparations as well as a safer option for apical surgery.
In an article published in January, 2018, Dr. Stephen Buchannan7,8 describes the use of a Dynamic Guidance System, the X-Guide (X-Nav Technologies, LLC, Lansdale, PA) in a case report. He attributes the use of this technique to Dr. Charles Maupin, an endodontist from Texas, USA. The X-Guide works by referencing two scanning drums, one secured to the patient’s jaw before CT imaging and the second secured to a latch-grip handpiece attachment. Two overhead cameras then trace these reference points allowing the computer processor to generate an avatar of the tooth and the drill in real time allowing the clinician to look at the computer screen while drilling into the tooth. Three cases were reported. He found the technique to be very effective in locating canals and in creating smaller less invasive access preparations.
ClaroNav (ClaroNav Inc, Toronto, ON, Canada, www.claronav.com) has been working at creating a similar application of their own. Their Dynamic Navigation for Implants (Navident) (Fig. 1) offers dental surgeons an easy to use, accurate, highly portable and affordable way to plan the desired restoration and implant placement on a virtual patient and then execute the plan on the patient’s jaw in real time. With their latest software release (Navident 2.1) this system offers:
• No need for a Fiducial, hence no need for a special (sometimes second) CBCT scan
• Works with a small Volume CBCT
• Works with any DICOM file from any CBCT machine
• No need for a second scan
• Head-Tracker for Maxillary area
• New Calibrator tool that enables the calibration and use of low and high-speed handpieces as well as piezotome saws
Navident has also been conducting “in vitro” testing of this software for its use in endodontics.
Fig. 1

As an eager to learn clinician with more than 35 years experience in endodontics and more than 25 years in the use of the Surgical Operating Microscope (Global Surgical Corp, Saint Louis, MO, USA) (Fig. 2), I decided to look at this technology myself and was invited to their company headquarters and was shown how the technology works on extracted and plastic teeth. The commonly used analogy for surgical navigation is the GPS device, showing the car’s location on the map.
Fig. 2

Therefore, I decided to try this technology while performing a case under the microscope without relying on the Navident Unit.
My objectives were as follows:
1. How well do I perform in locating a calcified canal when compared to the Navident Unit?
2. Shoot simultaneous videos (one through my microscope, the other with the Navident unit) and compare results
3. How accurate is Navident when compared to traditional access techniques?
4. How easy is it to use?
Case Report
A 63-year-old healthy female was referred to our practice for root canal treatment of tooth 1.2. She reported some swelling in the buccal area and very slight discomfort to biting emanating from this tooth. Clinical examination revealed slight buccal swelling and palpation sensitivity at the apex of 1.2. Percussion testing was positive. Ceramic crowns were noted on all 6 anteriors. Probing was within normal limits. No mobility was noted. The patient did not complain of thermal sensitivity. Two periapical radiographs were taken that revealed a large radiolucency associated with tooth 1.2 and the mesial aspect of 1.3 that had been previously root canal treated (Figs. 3A & B). The radiographs also revealed a very calcified canal on tooth 1.2. In addition, the orientation of the Ceramic crown was not parallel to the inclination of the root and of the canal. The diagnosis was necrotic pulp with a chronic apical periodontitis. Small volume CBCT was recommended in order to determine if 1.3 was involved and also to visualize and determine the location of the canal in 1.2. Options for treatment were discussed with a recommendation to proceed with RCT through the ceramic crown. The patient was also advised about the level of difficulty due to the calcified canal, the possibility of the crown breaking during access preparation, the difference in inclination of the crown with respect to the position of the root canal system and the possibility that apical surgery might have to be considered as a future option.
Fig. 3A

Fig. 3B

A small volume CBCT was requested for the patient with slice thickness to be no more than 0.4mm and the export format to include DICOM files in a standard multi file configuration.
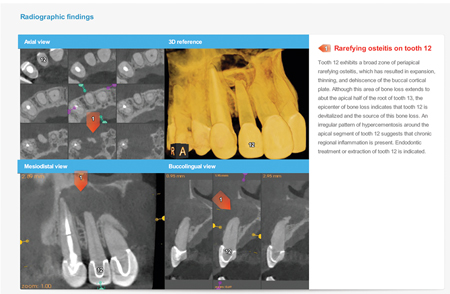
The results of the CBCT revealed that tooth 1.2 was the epicenter of the infection and that 1.3 appeared to be secondarily affected (Fig. 4).
Fig. 4
We then imported the DICOM files from the CBCT to the Navident software and proceeded to develop our digital planning for the best path to take in order to locate the calcified canal (Fig. 5). The software indicated that we would have to drill approximately 14 mm to find this canal (Figs. 6A & B).
Fig. 5

Fig. 6A

Fig. 6B

The patient was brought back for treatment. Local anesthetic was given in the usual manner. To enable the Navident system to track the patient’s maxilla, an optical tracking tag (“Head-Tracker”) was secured on the patient’s head (Fig. 7). The black and white pattern on the tag is recognized and being constantly tracked by the system’s optical tracking sensor, providing the system with the accurate position of the patient’s jaw at any time during the procedure. The patient’s Jaw is represented on the Navident’s screen by it’s CBCT image, functioning as a map, with the operator’s instrument, such as a drill, superimposed on it.
Fig. 7
Prior to starting the navigated access, the patient’s CBCT scan has to be mapped to the actual jaw. This process is called Registration. Traditionally, registration is achieved via a metallic fiducial-marker that has to be attached to the patient’s jaw during the acquisition of the CBCT scan, and its radiographic image is later recognized by the software in the CBCT scan. Registration using Navident can be performed using such a fiducial marker, but Navident provides an alternative registration method, called Trace Registration. This method does not require the use of an artificial fiducial marker. Instead it utilizes the already existing, radiographically distinct anatomical structures in the jaw, such as teeth, abutments and even bone.
In the Navident software, three maxillary teeth were marked on the CBCT scan. These teeth surfaces were then traced with a tracer tool (Fig. 8) that is also tracked by the Navident’s optical positioning sensor. During the tracing, the system continuously samples and records points on the traced teeth, which are then matched with the CBCT data, to register it with the physical patient’s jaw. The whole process takes no more than one minute.
Fig. 8

Following this step, the high-speed handpiece, also tracked by the system, is calibrated in a short two-step process: the axis is calibrated first, followed by calibration of the drill’s tip. This lets the system continuously track the bur’s direction and position, and to report it to the user on the Navident screen (Figs. 9A & B).
Fig. 9A
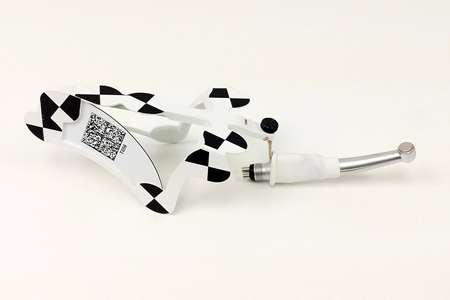
Fig. 9B

At this point an accuracy check was done by placing the tip of the bur on the tooth to be accessed to make sure that it corresponded to the exact point on the tooth to be treated on the computer screen (Fig. 10). Once this was confirmed, the rubber dam was placed and access into the tooth was started with a small diamond bur. After initial access through the ceramic crown, we then proceeded to use a white 31 mm Munce Discovery bur (CJM Engineering Tech, CA, USA), which its tip had been calibrated and tracked, was then used to attempt to locate the calcified canal. Changes in dentinal coloration could be seen via the microscope and these served as landmarks for us to be able to locate the canal. Drilling with considerable care and following the landmarks the canal was finally located at a depth of 13 mm and negotiated with #08K endodontic file (Figs. 11A & B). It is important to mention, that at no time during the procedure was the Navident unit used to help locate the canal. The procedure was done following conventional access techniques under the microscope and personal experience in locating severely calcified canals. The point of this exercise was to determine clinical accuracy compared to the Navident unit and vice versa. The canal was then negotiated and the working length was determined with the use of an apex locator. Shaping was completed with the use of the WaveOne Gold reciprocating file (Dentsply Sirona, York, PA, USA) and Calcium Hydroxide placed as an interim dressing as the canal could not be dried. The access opening was sealed with a composite and the patient returned two weeks later to have the treatment completed. The canal was then disinfected, dried and sealed with Gutta-Percha and BC Bioceramic sealer (Brasseler USA, Savannah, GA, USA). A composite restoration was then placed to seal the access cavity (Fig. 12). The patient is scheduled for a recall in six months to asses healing. The need for apical surgery was reviewed.
Fig. 10
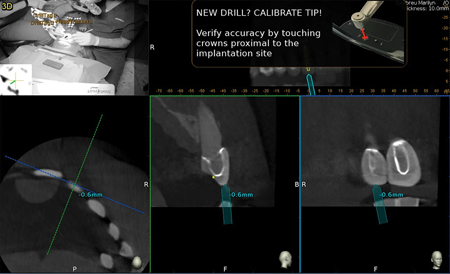
Fig. 11A

Fig. 11B
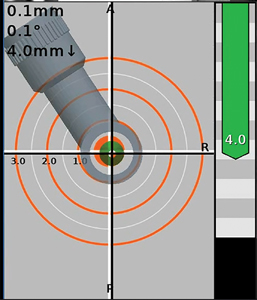
Fig. 12

Advantages of Dynamic Navigation
Navident can calibrate and track both high-speed and low-speed driven burs, piezotome saws and other rigid instruments such as osteotomes or even a dental or an endodontic probe, enabling the clinician with the use of any such device for access opening and surgical procedures.
The Trace Registration method (commercially known as “TaP” = “Trace and Place”) allows the dentist to register the CBCT scan to the patient by selecting three to six radiographically distinct, accessible landmarks on the screen, then tracing them in the patient’s mouth. This method eliminates the need for a special second scan to be taken with a metallic fiducial-marker affixed to the jaw with a thermoplastic stent. Aside of reducing the exposure to radiation, it reduces the chance for errors caused by stent dislocation during the scan and allows for the use of a small volume CBCT. As a consequence, it also minimizes time and cost to the procedure.
Once the handpiece and the bur are calibrated, Navident dynamically presents on the screen the actual place and position where to initiate the access. It also shows where the tip of the bur is in real time, guiding the operator to the predetermined place to locate the canal making the location of calcified and multiple canals a faster and more accurate procedure.
With the aid of this technology, smaller and more accurate accesses can be made. Preservation of valuable dentin is one of the main objectives when preforming any dental procedure. In addition, this technology will allow for the location of canals that otherwise could not be detected and negotiated with more traditional techniques. Dynamic Navigation has also the potential for assisting the surgeon in cases where apical surgery is indicated.
Conclusion
Comparing the Navident performance with the use of the microscope was very impressive. The computer navigation software preformed very accurately. At all times the software was on the exact path as the clinician when trying to locate the calcified canal. This case illustrates how accurate this technology is with tremendous potential in helping us in our day to day endodontic treatment. In my opinion this will positively impact the way we carry out root canal treatment by helping to locate very calcified canals with much smaller access cavities preserving more tooth structure. Like any new technology it has a learning curve. It has been said that the better you are at video games the faster you will learn using it. In the meantime, “Live Long and Prosper”.
A three-minute edited video can be viewed on YouTube of the procedure (https://youtu.be/SfQ9-09xjEo). This video shows simultaneously both the computer screen of the Navident unit and a video recorded through the microscope.
Oral Health welcomes this original article.
References
- Stefanelli LV, DeGroot BS, Lipton DI, Mandelaris GA; Accuracy of a Dynamic Dental Implant Navigation System in a Private Practice; Int J Oral Max Implants; Jan/Feb 2019.
- Emery RW, Progebin K; The use of Dynamic Navigation to Prevent Implant Complications- Every Patient, Every Time; Implant Practice; April 2017.
- Mohamed N, Nahmias Y, Serota K; The Cortical Window: Part Two Computer Guided Endodontic Surgery (CGES); Oral Health; May 2018.
- Block MS, Emery RW; Static or Dynamic Navigation for Implant Placement- Choosing the Method of Guidance. J Oral Max Surg ; Feb 2016.
- Norkin FJ, Ganeles F, Zfaz S, Modares A; Assessing image-guided Implant Surgery in Today’s Clinical Practice; Comp Conti Ed Dent; Nov 2013.
- Burgess D; Dynamic Navigation for Precise Implantation in Cases of Critical Anatomy; Implants; Jan 2017.
- Buchanan LS; Dynamic CT-Guided Endodontic Access Procedures; Dent Edu Lab; Jan 2018.
- Buchanan LS, Maupin C, Khademi J; A Preliminary Study of the Accuracy of Dynamic CT-Guidance for Endodontic Access Procedures done in 3D Printed Jaws modeled to have Simulated Calcified Pulp Chambers; to be Submitted for Publication.
About The Author
 Dr. Yosef Nahmias, was born and raised in Mexico City. After he graduated from the Universidad Tecnologica de Mexico, School of Dentistry, in 1980, he decided to advance his education and chose Endodontics as his specialty. Dr. Nahmias earned his Masters of Science degree in Endodontics in 1983 at Marquette University in Milwaukee, Wisconsin. The University of Toronto, Faculty of Dentistry has involved him in teaching their postgraduate level students in endodontics. Dr. Nahmias has authored many articles and continues to lecture in Canada and internationally. He has been a practicing Endodontist in Oakville, Ontario since 1983. He can be reached at yosi@allianceds.com.
Dr. Yosef Nahmias, was born and raised in Mexico City. After he graduated from the Universidad Tecnologica de Mexico, School of Dentistry, in 1980, he decided to advance his education and chose Endodontics as his specialty. Dr. Nahmias earned his Masters of Science degree in Endodontics in 1983 at Marquette University in Milwaukee, Wisconsin. The University of Toronto, Faculty of Dentistry has involved him in teaching their postgraduate level students in endodontics. Dr. Nahmias has authored many articles and continues to lecture in Canada and internationally. He has been a practicing Endodontist in Oakville, Ontario since 1983. He can be reached at yosi@allianceds.com.
RELATED ARTICLE: Dynamic Navigation For Orthograde And Retrograde Endodontics










