
Dens invaginatus, also known as dens in dente, is an embryological anomaly that occurs during tooth formation. The condition results in invagination of the amelodental structure within the pulp that can look like a ‘tooth within a tooth’ on radiographic evaluation, hence the nomenclature.1 The reported prevalence of adult teeth affected with dens invaginatus is between 0.3 to 10% (2). These cases may present difficulties with respect to diagnosis and treatment due to canal morphology.2
The aetiology of dens invaginatus is controversial and remains unclear. Oehlers considered that distortion of the enamel organ during tooth development and subsequent protrusion of part of the enamel organ will lead to the formation of an enamel-lined channel ending at the cingulum or sometimes the incised edge.3 Invaginatus can be classified in several ways, with Oehlers classification being the most widely accepted.2 This system categories invagination into 3 classes based on how far they extend radiographically from the crown into the root.3
Type I:
Invagination is minimal and enamel lined. Confined within the crown of the tooth and does not extend beyond the level of the external amelocemental junction.
Type II:
Invagination is enamel-lined and extends into the pulp chamber, but remains within the root canal with no communication with the periodontal ligament.
Type IIIA:
Invagination extends through the root and communicate laterally with the PDL space though a pseudo-foramen. Usually no communication with the pulp in the root.
Type IIIB:
The invagination extends through the root and communicates with the PDL at the apical foramen. usually there is no communication with the pulp.
With type III lesions, usually there is an inflammatory response within the PDL which gives rise to peri-invagination periodontitis.3
Fig. 1

Diagnosis and classification of dens invaginatus is based on clinical and radiographic examination. The clinical appearance will vary considerably and may appear normal or associated with unusual crown forms. Normally, there is a palatal pit or groove present, but there can be cingulum bifurcation.5 Radiographs represent the main diagnostic resource. Limitations associated with conventional radiography may be overcome with the use of CBCT imaging.6 The main consequence of dens invaginatus is the accumulation of debris that can lead to the rapid onset and progression of caries, with subsequent pulp involvement.
Dens Invaginitis canals can show complex anatomy. Advanced photon-activated irrigation methods have been introduced to help clean, debride and disinfect dental root canals with complex anatomy. Previous agitation techniques such as passive ultrasonic activation are limited by canal morphology, and depth of penetration of the instrument tip.7 Photon-induced photo acoustic streaming (PIPS) places a laser fibre tip into the pulp chamber filled with irrigation fluid and emits a pulped laser light into the fluid.7,8 If the laser light is sufficiently absorbed, the fluid is heated over its boiling point, producing vapour bubbles that expand and collapse, creating turbulent photoacoustic agitation of the irrigant. This moves the fluid in three dimensions though the root-canal system increasing the efficacy of debridement.7,8 Research shows that in the root canal system, shock waves can’t always be generated in irrigate by a single laser pulp due to spacial constriction.9 To improve the cleaning efficacy of PIPS, a new Shock Wave Enhanced Emission Photoacoustic Streaming (SWEEPS) modality has been developed.9,10,11
SWEEPS replaces a single super-short pulse from the pips with two ultra-short micro pulses separated by an optimal time delay.11 With proper timing, the second pulse in the SWEEPS laser pulse will accelerate the collapse of the bubbles from the first pulse, resulting in shock wave emission and photo acoustic current improvement.9 This will transfer the waves into narrow canals, leading to higher shear forces between the canal surface and irritants, improving the cleaning function and disinfection of the irrigation.9,10,11
CASE STUDY:
A 13-year-old patient was referred due to fluctuant swelling and pain on the centre of the hard palate. (Fig. 2) The pain came on suddenly at night and woke the patient from sleep. Teeth #12, 11, 21 and 22 had been diagnosed as having dens invaginatus, and teeth #11 and #12 were subsequently root canal treated due to pulp necrosis and acute apical abscess in the summer of 2020. Clinical diagnosis was Tooth #12: Previous root canal/Normal apical tissues; Tooth #11: Previous root canal/Acute apical abscess. Teeth #21 and #22 had fissure sealants placed in the palatal pits which has protected the nerve from necrosis.
Fig. 2

Fig. 3

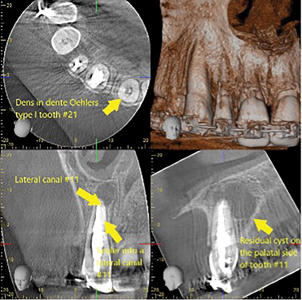
A CBCT was taken, and it was determined that tooth #11 had an Oehlers Type I configuration. The canal morphology likely led to an unfilled lateral canal the apical 1/3 and thus reinfection of the root canal system.(Fig. 4)
Fig. 4
Tooth #11 was re-treated on the same day to relieve the symptoms. The previous obturation material was removed, the canal cleaned using SWEEPS (Shock Wave Enhanced Emission Photoacoustic Streaming) modality for Er:YAG laser (Fotona 600, SWEEPS). Calcium hydroxide medicament was placed due to purulent discharge from the canal that we were unable to dry at this emergency appointment.
The patient returned four weeks later (after going to summer camp) with no pain or swelling from the tooth. Upon opening the tooth, no sign of purulence was noted. SWEEPS was again used to give the canal it’s final clean before obturation with warm gutta percha and BC Sealer (Angelus Bio-C Sealer). We will see the patient in a few months time for a follow-up; but presently, they remain symptoms free.
Fig. 5

CONCLUSION
In the past, conventional radiographic examination was often used to diagnose and classify Dens Invaginatus. It has, however, limitations in demonstrating the internal anatomy of the tooth with a complex root canal system such as in dens invaginatus cases. CBCT offers a more efficient way to diagnose and subsequently manage these cases. SWEEPS photo acoustic laser is also ideal in cleaning canals with complex anatomy. There is a very promising future for SWEEPS irrigation in endodontic treatment.
Oral Health welcomes this original article.
References
- Atkinson SE. The permanent maxillary lateral incisor. Am J Orthod. 1943; 29(12): 685-698
- Thaku S, Thakur N, Gupta M. Dents invagination: A review of literature and report fo two cases. J Nat Sci Biol Med. 2014 Jan-Jun; 5(1): 218-221
- Oehlers FA. Dens invaginatus I. Variations of the invagination process and associated anterior crown forms. Oral Surg Oral Med Oral Pathol. 1957; 10: 1204-18
- Gallacher, A., Ali, R. & Bhakta, S. Dens invaginatus: diagnosis and management strategies. Br Dent J 221, 383–387 (2016)
- Wang J, Fang Y ,Von den Hoff JW, Meng L. An update on the diagnosis and treatment of dens invaginatus. Aus Den J 62(3), 261-275
- Gomes de Oliveira N, da Silveira M, Batista SM, Veloso SR, Carvalho M, Travassos RM. Endodontic Treatment of Complex Dens Invaginatus Teeth with Long Term Follow-Up Periods. Iran Endod J. 2018 Spring; 13(2): 263-266
- Lukac N, Much BT, Jezersek M, Lukac M. Photoacoustic Endodontics Using the Novel SWEEPS Er:YAG Laser Modality. J LAHA 2017(1) ISSN 1855-9913
- DiVito E, Peters OA, Olivi G. Effectiveness of the erbium:YAG laser and new design radial and stripped tips in removing the smear layer after root canal instrumentation. Lasers Med Sci. 2012;27(2):273-80.
- Zhang C, Du J, Peng Z, Correlation between enterococcus faecalis and Persistent Intraradicular Infection Compared with Primary Intraradicular Infection; A Systematic Review. J Endod 2015; 41(8): 1207-13
- Jezersek M, Jereb T, Lukac N, Tenyi A, Lukac M, Fidler A. Evaluation of Apical Extrusion During Novel Er: YAG Laser-Activated Irrigation Modality. Phorobiomodulation, Photomedicine, Laser Surg. 2019; 37(9): 544-50
- Lei, Lishan and Wang, Fang and Wang, Yanhuang and Li, Yijun and Huang, Xiaojing, Laser Activated Irrigation with SWEEPS Modality Reduces Concentration of Sodium Hypochlorite in Root Canal Irrigation. Available at SSRN: https://ssrn.com/abstract=4047158 or http://dx.doi.org/10.2139/ssrn.4047158
About the Author

Dr Riley Lewis is a practicing endodontist in Toronto. He obtained his DDS from Trinity College, University of Dublin, Ireland, and obtained his MSc and certificate in Endodontics from the University of Minnesota. He is a part time instructor at University of Toronto.









