
Endodontics has changed considerably over the past 60 years, yet the core principles remain unchanged: Instruments are still sequentially used to shape canals, irrigation is still passively delivered into the canals, and canals are still obturated with gutta-percha (GP). As endodontics grew in popularity, manufacturers continued to refine the armamentaria. The trend was a big access and big shapes. The rationale was that It minimized a mishap like file separation, and a larger canal allowed for a larger volume of irrigant to be exchanged, for better disinfection. The dangers of over-prepared shapes was mostly overlooked because the thinking was that the tooth was going to have a crown placed for protection. This was definitely a lack of awareness up until a little more than a decade ago. It is now known that the region of the tooth most important in maintaining structural integrity is the Peri Cervical Dentin (PCD), a zone roughly 4 mm above the crestal bone and extending 4-6 mm apical to the crestal bone.1 This is the area of the tooth commonly obliterated by a traditional endodontic access and over-flaring the coronal third of the canal.2
Recent Innovative technologies in metallurgy (heat treated NITI), irrigation (chemistry and fluid dynamics), and sealers (calcium silicates) have stirred up established concepts in endodontics and a paradigm shift is now evident: the move away from active instrumentation with passive irrigation to passive instrumentation with active irrigation. The intersection between preserving the PCD and maintaining the core principles is the direction endodontics is headed. A few of these innovations are described below.
Clean (irrigation)
Irrigation has evolved on two parallel fronts over the last 20 years: 1. More advanced irrigation solutions have been developed that are much more effective than traditional sodium hypochlorite. 2. Ways to make the same solution be more effective by understanding the concepts of fluid dynamics.
Chlorxtra ( Vista Apex, Racine, WI) is a 6% sodium hypochlorite formulation with added surfactants, allowing it to penetrate deeper than standard sodium hypochlorite.
QMix 2 in 1 (Dentsply Sirona, Charlotte, NC) is a proprietary formulation that combines the smear layer removal of EDTA and an anti-microbial component for an effective final rinse after sodium hypochlorite.
The newest solution in endodontics is Triton (Brasseler USA, Savannah, GA), an all-in-one solution that replaces sodium hypochlorite and EDTA entirely.
Fluid dynamics is the study of the flow of liquids through various spaces and obstacles. In Endodontics, this is very important as all irrigation solutions have certain obstacles that prevent them from free-flowing throughout the canal spaces. There is a plethora of research supporting activation of irrigants by either sonic, ultrasonic, Multi-sonic, or laser energy for maximum penetration into deeper canal spaces.3,4,5
Due to the high surface tension of sodium hypochlorite, passive irrigation into a narrow canal space creates a vapor lock (VL), which prevents the free flow of the solution to the more apical regions of the canal space. It is shown that because of VL, irrigant reaches only 1-1.5mm beyond the tip of the needle delivering the solution.6 A surfactant added to the solution lowers the surface tension and lessens, but does not eliminate, VL. EndoVac (KavoKerr, CA) an apical negative pressure irrigation system addresses vapor lock by delivering a controlled flow of irrigant into the pulp chamber, with a much more effective debridement up to 1mm from working length, as compared to positive pressure irrigation.7
Lasers, such as Waterlase (Biolase, Foothill Ranch, CA) are another area where considerable research has been done to assess its influence on fluid dynamics. The laser energy creates cavitation effects and pressure waves, causing deeper irrigant penetration into the dentinal tubules.8
California start-up, Sonendo (Laguna Hills, CA), approached irrigation efficacy by developing the GentleWave console, based on multi-sonic energy. This closed system is highly automated and the clinician holds a hand piece in place for 8-10 minutes, while the system delivers a continuous flow of low concentration NaOCl and EDTA using a proprietary hand piece.

Fig. 1A

Fig. 1B

Fig. 1C

Fig. 2A
Fig. 2B

Fig. 2C

Fig. 2D

Fig. 3A

Fig. 3B

Shape (Access Design and canal instrumentation)
ProTaper Universal® file system (Dentsply Sirona) was introduced more than twenty years ago. The simplicity of the file system with its efficient cutting mechanism has proven to be very popular among clinicians. A decade later, with advancements made in metallurgy, SS White helped usher a new era of filing systems, designed to preserve the PCD. In addition, using a pre-operative CBCT volume, clinicians can design an appropriate access unique for each individual tooth, rather than the classical instruction of a singular access design for each tooth type. The ultimate goal is to remove as little tooth structure while not compromising the procedure end goals.
A recent addition to conservative Instrumentation is the ExactTaperH DC (ETHDC) file system (SS White, Lakewood, NJ; Clinical Research Dental, London, ON) This system has the following characteristics:
- Advanced heat treated alloy
- Smaller Maximum Flute Diameter (MFD)
- A 0.8mm metal core design
- Workflow that is similar to the most popular variable taper file system.
The proprietary heat-treating processes utilized in the ETHDC create a file system with superior controlled memory and flexibility. One of the benefits of the heat-treating process is that ExactTaperH DC (SS White, Lakewood, NJ; Clinical Research Dental, London ON) has a longer unwound state, i.e. plastic deformation. To put it more simply, clinicians have a higher chance to visually inspect and discard a defective file before it breaks.
The ETHDC file system has a 33% smaller MFD than most mainstream files systems, which is consistent with the goal of PCD preservation. In addition, the narrower taper of the instrument engages a smaller surface area of the root, which in turn produces less heat. Frictional heat generated during instrumentation has been shown to increase the incidence of crack formation in the canal.9,10
When creating a cutting file, manufacturers start with a block of metal and proceed to twist and grind the block in order to create the desired cutting flutes. The process of twisting and grinding of the metal inherently creates defects in the metal, which theoretically can affect its fatigue resistance. To overcome this, manufacturers, including SS White implement surface engineering techniques to the metal. However, an additional advantage of all SS White file systems is the original block is 0.8mm diameter, which is smaller than the block used to make most file systems. This, in turns, yields less defects created by the machining of the metal.
The best part of the ETHDC file system is there is no learning curve needed to use it optimally. The workflow is very similar to the familiar workflow of the popular ProTaper® file system.
Fig. 4A

Fig. 4B

Fig. 5A

Fig. 5B

Fig. 5C

Obturation
3D Obturation of the root canal system has generally been accepted as the gold standard, using thermoplasticized GP in a variety of techniques. The role of the sealer has traditionally been a lubricant and space filler. Obturation of thinly shaped canals poses a challenge to the clinician. The advent of calcium silicate based sealers such as BIO C Sealer (Angelus, Londrina, Brazil; Clinical Research Dental, London, ON) and EndoSequence BC Sealer (Brasseler USA, Savannah, GA) has enabled a shift from a GP based obturation to a sealer based obturation. The excellent properties of this class of sealer, such as biocompatibility (non-toxic), sustained high pH, and its hydrophilic nature, enables the sealer to play a larger role in the obturation of the root canal system as a filler, with a single cone of GP acting as a tool to disperse the sealer throughout the canal. This technique, called “hydraulic condensation”, requires a GP cone size that closely matches the Master Apical File (MAF) used during instrumentation. This allows the clinician to effectively generate the hydraulic forces to disperse the sealer as the cone is inserted into the canal. Calcium silicate based sealers address the challenges of obturation of minimally shaped canals.
In summary, we have the knowledge to understand the importance of PCD to the survival of a tooth. We have the technology to ensure optimal root canal treatment and preserving valuable tooth structure are not mutually exclusive of one another. The ETHDC file system is the perfect answer to clinicians looking to practice 21st century endodontics.
Fig. 6
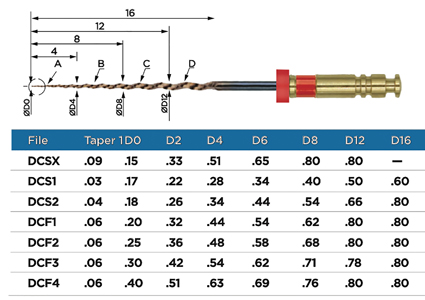
Fig. 7A

Fig. 7B

Fig. 7C

Fig. 7D

Fig. 7E

Fig. 8A

Fig. 8B

Fig. 8C

Oral Health welcomes this original article.
References
- Clark D, Khademi J. Modern molar endodontic access and directed dentin conservation. Dent Clin North Am. 2010 Apr;54(2):249-73.
- Pereira JR, McDonald A, Petrie A, Knowles JC. Effect of cavity design on tooth surface strain. J Prosthet Dent. 2013;110:369–75.
- Al-Jadaa A, Paque F, Zehnder M: Necrotic Pulp Tissue Dissolution by Passive Ultrasonic Irrigation in Simulated Accessory Canals, Int Endod J 42:59-65, 2009.
- Guneser M, Arslan D, Usumes A: Tissue Dissolution Ability of Sodium Hypochlorite Activated by Photon-initiated Photoacoustic Streaming Technique, J Endod 41:5, pp. 729-732, 2015.
- Gutarts R, Nusstein J, Reader A, Beck M: In vivo debride ment efficacy of ultrasonic irrigation following hand-rotary instrumentation in human mandibular molars, J Endod 31:3, pp. 166-170, 2005.
- Tay FR, Gu LS, Schoeffel GJ, Wimmer C, Susin L, Zhang K, et al. Effect of vapor lock on root canal debridement by using a side-vented needle for positive-pressure irrigant delivery. J Endod. 2010;36:745–50.
- Nielsen B, Baumgartner C: Comparison of the EndoVac System to Needle Irrigation of Root Canals, J Endod. 2007;33:611-615.
- DiVito E, Peters OA, Olivi G: Effectiveness of the erbium: YAG laser and new design radial and stripped tips in removing the smear layer after root canal instrumentation, Lasers Med Sci 27:2, pp. 273-280, 2012.
- Liu R, Hou BX, Wesselink PR, et al. The incidence of root microcracks caused by 3 different single-file systems versus the ProTaper system. J Endod 2013;39:1054–6.
- Karataş, Ertuğrul et al. Dentinal Crack Formation during Root Canal Preparations by the Twisted File Adaptive, ProTaper Next, ProTaper Universal, and WaveOne Instruments. J Endod 2014;41: 261–264.
About the Author
 Dr. Reza Farshey received his Bachelors degree in physics from McGill University, and his dental degree from Tufts University. He practised as a general dentist for seven years, and completed his endodontic training at Boston University in 2007. He is a full-time clinician and partner at Chevy Chase Endodontics, in Washington, DC. Dr. Farshey is a US board-certified endodontist and authored two chapters in the endodontic textbook, Current Therapy in Endodontics. He is the Founder and CEO of BubblesEndo, an AI-based tech start-up developing software to help dentists make accurate endodontic diagnoses (endogenie.ai). Email: dr.farshey@ccendo.net
Dr. Reza Farshey received his Bachelors degree in physics from McGill University, and his dental degree from Tufts University. He practised as a general dentist for seven years, and completed his endodontic training at Boston University in 2007. He is a full-time clinician and partner at Chevy Chase Endodontics, in Washington, DC. Dr. Farshey is a US board-certified endodontist and authored two chapters in the endodontic textbook, Current Therapy in Endodontics. He is the Founder and CEO of BubblesEndo, an AI-based tech start-up developing software to help dentists make accurate endodontic diagnoses (endogenie.ai). Email: dr.farshey@ccendo.net










