
ABSTRACT
Gum disease starts between the teeth. The interdental space is the most vulnerable yet most neglected area of the mouth because of its anatomy and the fact that most people hate to floss. There are many floss alternatives that are currently available that are much easier to use than floss, which would not only encourage more compliance, but may even clean more efficiently. A new innovative interdental cleaner and delivery device called a “PerioTwist”™ is also introduced.
The interdental space is the most neglected area of the mouth, yet the most vulnerable. Its anatomy provides the perfectly inaccessible environment for dental plaque to accumulate and fester, thereby causing great harm to both teeth and periodontium. In fact, the most difficult, complicated, and expensive therapy that a dentist performs daily is caused by the pathology of the interdental space. Neither the bristles of the toothbrush nor mouthwash can effectively access and clean this area; an alternate device must be used to clean the interdental space.
Dental floss, invented by Dr. Levi Spear Parmly in 1815, is the benchmark interdental cleaning device. The first dental floss patent was granted to J&J in 1898. The drawback of dental floss, however, is that most people dislike the process. According to the ADA, only 12-40% of Americans floss daily; 20% never floss.1,2 More than a third of people surveyed would rather be doing unpleasant chores than flossing their teeth daily: 14% would rather clean the toilet; 9% would rather sit in gridlock traffic for an hour, and 7% would rather listen to small children crying on a plane.
Alternatives to dental floss have recently been introduced to address problems and limitations of dental floss (non-compliance, shedding, tearing, complicated instructions for using both, preferably clean, hands, and inefficient cleaning of larger embrasures and deeper pockets, indentations and furcations).
As individuals age, they are perceived to “get longer in the tooth”. Teeth typically do NOT erupt but the receding gingiva gives that impression. Embrasures and interdental spaces become larger and a thin dental floss can no longer adequately clean this space. Furthermore, salivary flow decreases, allowing for more food and plaque accumulation. Dexterity also diminishes with age, necessitating a floss alternative.
The floss alternatives used to clean the interdental space have both benefits and limitations. The PerioTwist interdental cleaner and delivery device has been developed to address the shortcomings of floss and the existing floss alternatives.
Anatomy of the Interdental Space
In order to better evaluate interdental cleaners, the anatomical characteristics that make this area difficult for patients to clean and for professionals to treat must be highlighted (Figs. 1-3).
1. Embrasure sizes: tight, moderate, wide / long, short
2. Root proximity: tight, spaced
3. Contact Area: large, small/wide, narrow
4. Papillae: large, small/thick, thin
5. Col: un-keratinized
6. Furcations, root and pocket concavities: hardest areas to clean
FIGURE 1. Interdental gingiva.

FIGURE 2. Un-keratinized gingival col.

FIGURE 3. Interdental “peaks”.
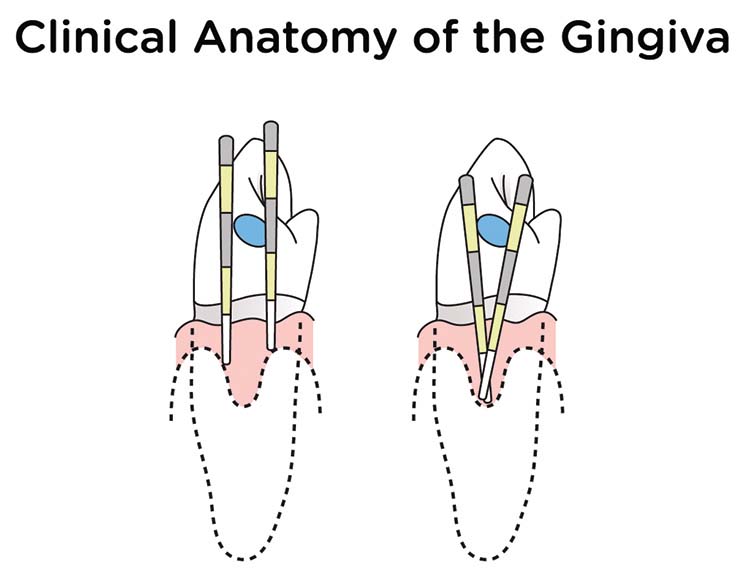
The interdental area is the part of gingiva which extends in between two teeth up to the contact point. The interdental gingiva occupies the gingival embrasure, which is the interproximal space between the teeth, apical to the tooth contact. The interdental embrasure can be pyramidal or have a “col” shape. Attached gingiva is resistant to masticatory forces and is always keratinized but the col varies in depth and width, depending on the size and form of the contacting tooth surfaces and is not keratinized. The epithelial covering of the col consists of the marginal gingiva of the adjacent teeth, and because it is not keratinized, this area is much more fragile and vulnerable to periodontal breakdown. The col is more pronounced in the broad interdental gingiva of the posterior teeth, a possible reason for periodontal disease often starting between the posterior teeth.
Root proximity, embrasure size, furcations and root concavities are anatomical considerations in the selection of appropriate floss alternatives (Figs. 4, 5).
FIGURE 4. Root indentations and furcations.

FIGURE 5. Multiple sizes.

Floss entry into the col valley is limited by the gingival interdental “peaks”. Numerous studies have shown that interdental brushes clean furcations and root indentations much more effectively; but it is important to choose the appropriately sized brush. The patient must remember which colour-coded size fits where, and must carry various brush sizes. Furthermore, the supporting central wire may scratch, break and be inappropriate for sensitive roots and implants.
The PerioTwist is an innovative “one-size-fits-all” floss alternative that simply and effectively cleans the interdental space of all teeth regardless of size and anatomy.
It can be used with prophylaxis paste to clean the interdental space and to deliver topical medicaments such as chlorhexidine, varnish, bleaching gels, re-mineralization pastes, etc. PerioTwist will not remove these medicaments when disengaged in a clockwise direction.

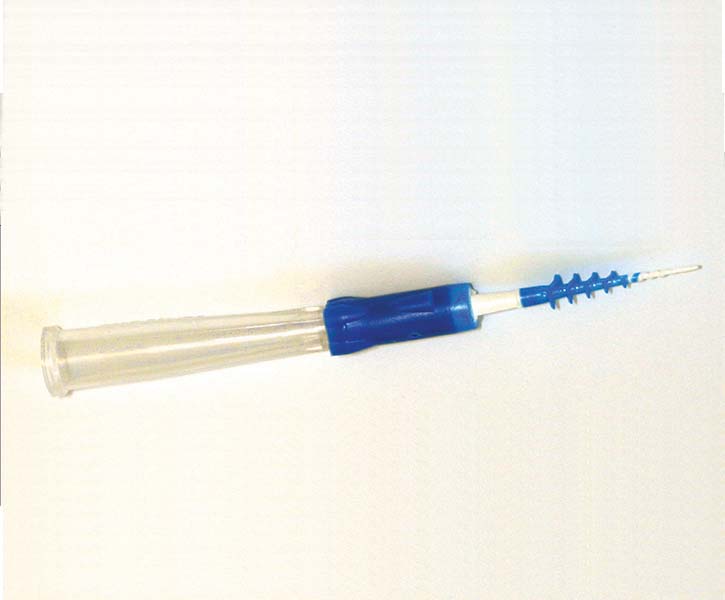
It is inserted and manipulated with only two fingers (versus both hands for floss) and can snap on to a prophy angle. The cover may snap into the handle extending the length if desired (Figs. 6-8).
FIGURE 6. PerioTwist with cover.
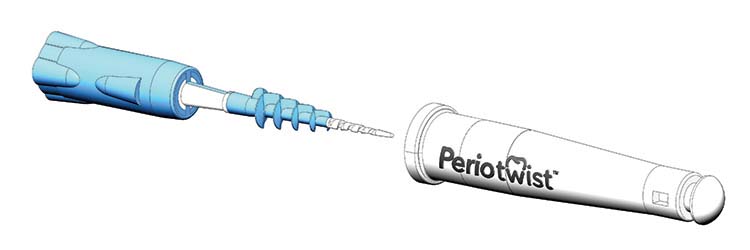
FIGURE 7. PerioTwist and cover.
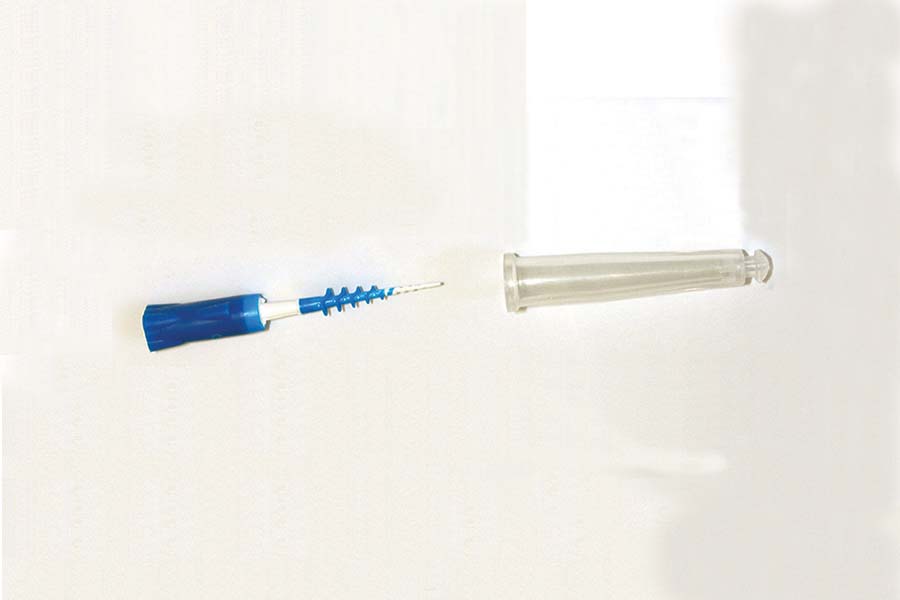
FIGURE 8. Cover snaps into handle.
1. Manual Cleaning (Figs. 9, 10).
FIGURE 9. PerioTwist cleaning between teeth.

FIGURE 10. Occlusal view.

2. Medicating Dip it – Twist it! (Figs. 11-14)
FIGURE 11. Dip the PerioTwist in paste, gel or solution.

FIGURE 12. Insert PerioTwist between teeth twisting “clockwise”.

FIGURE 13. Medicament twisted between teeth.

FIGURE 14. Medicament remaining.

3. Motorized (Figs.15-17)
FIGURE 15. Snap PerioTwist onto prophy angle.

FIGURE 16. Dip or apply prophy paste or medicament onto PerioTwist.

FIGURE 17. First – Insert PerioTwist between the teeth.

FIGURE 18. Then “slowly” rotate ”clockwise”.

Discussion
For over forty years, the author, his associates and hygienists have been educating and motivating their patients to floss. Until recently, dental floss was the benchmark device for interdental cleaning. Floss is effective but most people dislike flossing. It is technique sensitive, difficult to teach and learn. It involves two clean hands, manual dexterity, coordination, and often, a mirror and bathroom. Patients are uncomfortable when the floss shreds, tears, or snaps through the contact area, causing pain and bleeding. The “blue finger syndrome” is also a major drawback. The dental team, both dentists and hygienists, continue to be frustrated when patients are advised to floss – with the certain knowledge that most will not. Dental practitioners are tired of repeating the flossing “spiel” and patients are tired of the same old hectoring. According to the recent research, one quarter of patients routinely lie to their dentist or hygienist that they floss.8
The evidence-based research overwhelmingly demonstrates the deleterious effects of dental plaque on the periodontium and teeth, as well as on overall patient health. According to recent findings from the Centers for Disease Control and Prevention (CDC), half of Americans aged 30 or older have periodontitis, the more advanced form of periodontal disease. This equals approximately 64.7 million Americans.
In 2012, JoAnn Gurenlian investigated the importance of plaque, and its relationship to oral diseases such as gingivitis, periodontitis, and caries, as well as the growing links to systemic health.11 A number of referenced studies demonstrated the relationship of dental plaque and diseases such as diabetes, cardiovascular and respiratory diseases, Alzheimer’s, and
negative pregnancy outcomes.8
Much of the research relating to interdental cleaning is ambiguous, uncontrolled, and all too often, manufacturer-sponsored.13 A recent study presented an excellent systematic review evaluating interdental brushes and floss effectiveness for control, bias, objectivity, and significance.13 After an exhaustive review of the data, the conclusions were (a) motivation was a key element, and (b) ease of use of a product would affect the user’s motivation.3
1. The majority of the test study individuals preferred interdental brushes as they found them simpler to handle
2. Test subjects favored using only one hand.
3. They felt that interdental brushes were more time efficient.2
4. Smukler noted that proximal sides of teeth usually have some curvature or concavity.10
5. Interdental brushes were most effective as some of the bristles cleansed the outer areas while other bristles extended into the concavities as they were drawn back and forth against the surfaces of adjoining teeth.3,8
6. Although research is limited, it is fair to assume that inter dental picks with projections will clean concavities and furcations more effectively than floss.
7. Inter dental picks are much easier to use leading to better compliance.
8. Softer picks tend to break easily and require various sizes
9. Harder picks may scratch hard and soft tissues and clean in only two dimensions.
Conclusion
The interdental space, relatively inaccessible to the toothbrush or mouthwash is very fragile and vulnerable. It provides a perfect accumulation spot for bacteria and debris, hiding plaque that can cause destruction of both hard and soft dental tissues, malodor, and increased risk of cardiovascular and other systemic diseases.7 Because most people do not floss for all of the reasons already mentioned, the interdental space is the most vulnerable, yet most neglected area of the mouth.
The time has come for the dental profession to accept that it is not enough to continue advocating flossing to the majority of patients who consistently refuse to floss, no matter how many times they are instructed, re-instructed, and motivated. It is the time to recognize and advocate floss alternatives that clean the interdental space of patients who refuse to floss and/or have large interdental spaces, which may be more effectively cleaned with floss alternatives. OH
Dr. Allan Coopersmith has been practicing dentistry for 40 years in Montreal Canada and is deeply passionate about preventing oral disease. He has been awarded fellowships in numerous academies and taught restorative dentistry for many years at his Alma mater McGill University. He is the co-inventor of the “PerioTwist”™ interdental cleaner and delivery device.
Nathalie Fiset is a registered hygienist who has been practicing Oral Hygiene for 20 years in Montreal Canada and has dedicated herself to instructing as well as motivating her patients in the prevention of oral disease. She is a co-inventor of the “PerioTwist”™ interdental cleaner and delivery device.
Oral Health welcomes this original article.
References:
1. Spear Education, LLC, Denise Prichard, Jan 16, 2013
2. Slot DE, et al.a systematic review Int J Dent Hygiene 2008; 6: 253–2642.
3. A Comparison of the Efficacy and Ease of Use of Dental Floss and Interproximal Brushes in a Randomised Split Mouth Trial Incorporating an Assessment of Subgingival Plaque. Noorlin I, Watts TL. Oral Health Prev Dent 2007; 5: 13-18.
4. https://www.perio.org/ june, 2015
5. The Role of Dental Plaque Biofilm in Oral Health. Gurenlian JR. American Dental Hygienists’ Association | March 2012 http://www.cdeworld.com/courses/0009.
6. American Academy of Periodontology;http:// www.perio.org. June 23, 2015
7. Chronic Diseases and Health Promotion. Centers for Disease Control and Prevention. 13 Aug. 2012. Web. 15 Sept. 2013.
8. The effectiveness of interdental brushes,Irene Esteves, RDH,MPH. RDH
9. The Role of Dental Plaque Biofilm in Oral Health. Gurenlian JR. American Dental Hygienists’ Association | March 2012 http://www.cdeworld.com/courses/0009.
10. Interproximal tooth morphology and its effect on plaque removal. Smukler H, Nager MC, Tolmie PC. Quintessence Int 1989:20:249-255.
11. Comparison of Interdental Brush to Dental Floss for Reduction of Clinical Parameters of Periodontal Disease: A Systematic Review. Pauline H. Imai, DipDH,BDSc(DH),MSc(Dent Sc),RDH; Xiaoli Yu, MSc; David MacDonald, BDS, BSc(Hons.),MSc, DDS(Edin.), DDRRCR, FDSRCPS,FRCD(C).











