
Amid our present-day pandemic, the disease of oral and oropharyngeal cancer once again has a much larger adversary. April has come and gone with very little focus on it being Oral Cancer Awareness Month. All attention understandably has been on the COVID-19 pandemic.
However, globally, the picture of oral and oropharyngeal cancer is very troubling. With the data that is available through reporting centres, we understand the burden to be approximately 640,000 cases worldwide. This number repeats itself every year with close to 50 percent of those diagnosed today not surviving beyond five years. The heartbreaking aspect is that most cases are discovered in the later stages, reducing the five-year survival rate dramatically. This is worthy of our attention and our commitment to do all we can to combat the disease and discover it in its earliest stages.
As a global community we are feeling vulnerable to the COVID-19 pandemic. When compared to oral and oropharyngeal cancer, we have taken some solace in recognizing that we can mitigate our risk by abstaining from using tobacco products and alcohol. However, don’t be misled. The rising number of oral and predominantly oropharyngeal cases are caused by a very common virus; a virus so common that the CDC (Centers for Disease Control) states that almost every adult will have an infection in their lifetime. Here are the facts.
- Human papillomavirus or HPV-related oropharyngeal cancer rose 225% in the same time period as a 50% decline was witnessed in HPV-negative oropharyngeal cancer.1,2 Refer to Figure 1.
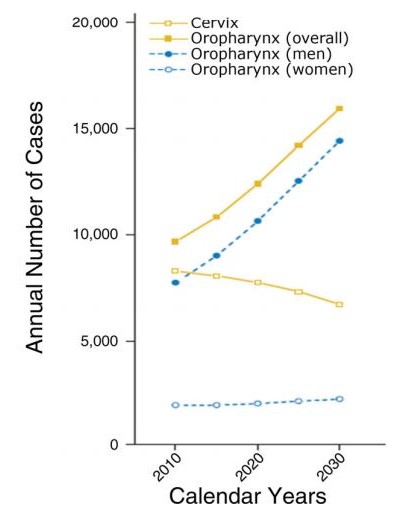
- HPV-related oropharyngeal cancer surpassed HPV-related cervical cancer in 2015 as the leading anatomical site for HPV-related cancers in the body.3 Refer to Figure 2.
- Studies estimate 70–90% of all new oropharyngeal cancers are HPV-related.4
- Patients are more likely to be younger, white males in their 40s and 50s, never smokers or have reduced alcohol exposure.4
- Males are at greater risk with an incidence of 4 to 1 over females.5
- Symptoms vary greatly from the typical oral cancer symptoms with which we are familiar.
Fig. 1
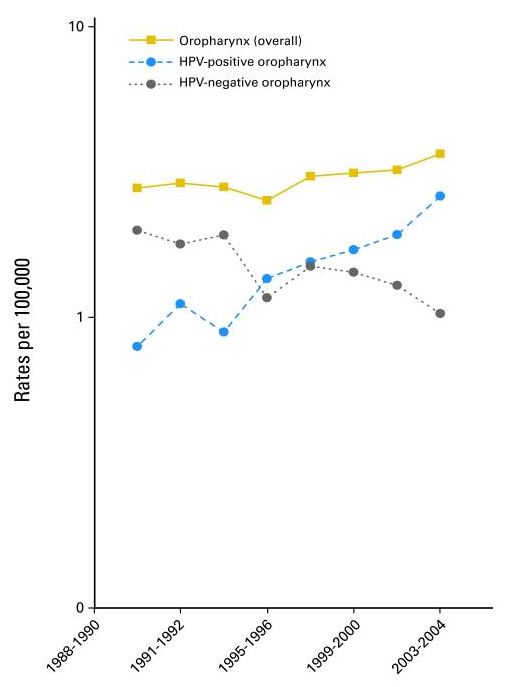
Fig. 2
Due to HPV’s affinity for lymphoid tissues, we are observing this cancer to occur in the posterior areas of the oropharyngeal region. This presents a challenge to assessment and to discovery of the presence of this cancer. No, we don’t possess a laryngoscope and ability to perform procedures to fully examine this area, however we do have eyes, ears and hands. We have eyes to evaluate asymmetry of both the face and neck. We have ears to observe a change in our client’s voice such as hoarseness. Above all we have hands to feel. The essential extraoral and intraoral visual examination needs to always be accompanied by tactile palpation. Without this component to our examination, we will miss the detection of many oral abnormalities. Relying on the visual assessment only will hinder our capabilities and place our dental clients at risk for later discovery of oral and oropharyngeal cancer. It is imperative that we recognize the subtle and often life-saving symptoms that accompany this type of cancer. The following is a list of some of these symptoms that may accompany HPV-related oropharyngeal cancer in the oropharynx.
- A non-healing lesion
- Bleeding in the mouth or throat
- Pain when swallowing or difficulty swallowing
- Unilateral ear pain
- Feeling of something caught in the throat or continual clearing of throat
- Hoarseness
- Persistent cough
- Continual lymphadenopathy; asymmetry in neck to swollen, persistent nodes
- Difficulty articulating certain words; slurred speech
- Unexplained weight loss
- Fatigue
- Continual throat infections not resolved by antibiotics
- Tonsillar asymmetry
- Tongue that tracks to one side when stuck out
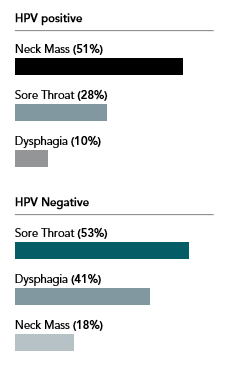
The palpation of the posterior triangle of lymph nodes including the cervical and supraclavicular group bound anteriorly by the posterior border of the sternocleidomastoid muscle and posteriorly by the anterior border of the trapezius muscle is essential. As depicted, a neck mass is more often associated with an HPV-positive tumor vs an HPV-negative.6
The etiologic pathway for lymphadenopathy may be multi-factorial and related to the onset and duration. An acute, infectious presence may be represented by a node that is tender to palpation, moveable, soft and the patient may already be aware of an underlying infection. Typically this type of occurrence will resolve on its own or with the use of antibiotic therapy. A lymph node that is firm or hard, fixed to the underlying structures, asymptomatic accompanied often by a lack of awareness is more characteristic of a malignancy. If the health history and assessment do not reveal an etiologic pathway or the lymphadenopathy persists beyond 14 days, further investigation is necessary. Computed tomography, ultrasound and the need for a fine-needle aspiration biopsy may be performed providing additional diagnostic information and a management pathway. The sensitivity and specificity of fine-needle aspiration biopsy in detecting a malignancy range is from 77% to 97% and 93% to 100%, respectively.7
Intraorally, it is imperative to continue to employ a visual and tactile approach to assessment. High risk anatomical areas include the floor of the mouth, the tongue and the palatal tissues. It is wise to follow a systematic approach when assessing the soft tissues of the oral cavity as we do with all our assessments.
At minimum, a comprehensive visual and tactile extraoral and intraoral examination should be performed on every adult client annually. A symptom or finding persisting more than 14 days should always be investigated further. Magnification and a headlight will provide the clinician with the best opportunity to discern visual changes in the soft tissues. Without the use of magnification, soft tissue abnormalities will be undeniably overlooked. The use of adjunctive screening devices such as VELscope provide us with further capabilities to see beyond what white light examination may have revealed. Typically, abnormal cellular differentiation and proliferation starts at the basement membrane. With the use of direct fluorescence visualization, adjunctive screening devices can penetrate through to the basement membrane providing greater capabilities for earlier discovery of abnormalities.
Oral cancer doesn’t observe the month of April specifically. Oral cancer is diagnosed 365 days throughout the entire year. A campaign was launched in collaboration with the Oral Cancer Foundation and Throat Scope, an all-in-one illuminated tongue depressor, with an objective to have the public check their mouth in between dental visits for anything new or different that persists beyond 14 days. This campaign alone is the biggest single opportunity we have to impact earlier discovery of oral cancer. Teach your clients how to check their mouth at home for the early signs of oral cancer through the “Check Your Mouth” website: checkyourmouth.org
The real objective is to save lives and secondly to improve lives. Late stage discovery subjects a patient to the rigors of radiation therapy often in combination with chemotherapy. Unless personally experienced, we have no idea what it must be like to live with permanent disfigurement, a total depletion of saliva, or fear of choking on thick, ropey saliva, or living with the continual fear of recurrence – and the list goes on and on. Ask an oral cancer survivor and be prepared to be shaken. Together we are a powerful team in minimizing late stage discovery of oral cancer.
Disclaimer: Jo-Anne Jones received no compensation for writing this article. She is a member of the Oral Cancer Foundation RDH Advisory Board and an advisor to Holland Healthcare Inc., developer of Throat Scope, Key Opinion Leader to Apteryx Imaging and Orascoptic. Jo-Anne will be presenting “Hindsight is 20/20: Missing the Oral/Oropharyngeal Cancer Diagnosis” supported by a collection of oral cancer survivor’s inspiring stories at the upcoming 2020 ODHA Re-Energize Conference in September. For further information or to contact Jo-Anne visit her website at jo-annejones.com
References
- Chaturvedi A, Engels A, Pfeiffer RM et al. Human Papillomavirus and Rising Oropharyngeal Cancer Incidence in the United States. Jour of Clin Oncol published on October 3, 2011.
- Dan P, Zandberg MD, Bhargava R et al. The Role of Human Papillomavirus in Nongenital Cancers. CA Cancer J Clin 2013;63:57-81.
- Trends in Human Papillomavirus-Associated Cancers – United States, 1999 – 2015. Morbidity and Mortality Weekly Report (MMWR) August 24, 2018. 67:33;918-924.
- Young D, Xiao CC, Murphy B et al. Increase in head and neck cancer in younger patients due to human papillomavirus (HPV) Oral Oncol Vol 51. Iss 8. August 2015 p. 727 – 730.
- https://oralcancerfoundation.org/understanding/hpv/hpv-oral-cancer-facts/
- McIlwain WR, Sood AJ, Nguyen SA et al. Initial Symptoms in Patients with HPV-Positive and HPV-Negative Oropharyngeal Cancer. JAMA Otolaryngol Head Neck Surg. 2014;140(5):441-447.
- Haynes J, Arnold KR, Aguirre-Oskins C, Chandra S. Evaluation of neck masses in adults. Am Fam Physician 2015 May 15;91(10):698-706.
About the Author
 Jo-Anne Jones, President, RDH Connection Inc. is a successful entrepreneur and international, award winning speaker. Jo-Anne has been selected as one of DPR’s Top 25 Women in Dentistry and is a returning 2017 Dentistry Today CE Leader for the 7th consecutive year. Jo-Anne is president of an educational and clinical training company and a sought after writer for leading dental journals and publications across the U.S., Canada, and the UK. Her frank and open style of lecturing complemented by the provision of clinical resources has earned many loyal followers. She may be contacted at jjones@jo-annejones.com
Jo-Anne Jones, President, RDH Connection Inc. is a successful entrepreneur and international, award winning speaker. Jo-Anne has been selected as one of DPR’s Top 25 Women in Dentistry and is a returning 2017 Dentistry Today CE Leader for the 7th consecutive year. Jo-Anne is president of an educational and clinical training company and a sought after writer for leading dental journals and publications across the U.S., Canada, and the UK. Her frank and open style of lecturing complemented by the provision of clinical resources has earned many loyal followers. She may be contacted at jjones@jo-annejones.com











