
The Need
It is estimated that 30% or more of the adult population is partially or totally edentulous. For the edentulous patient, dentures offer many advantages when compared to other alternatives. They can be esthetically pleasing, easy to maintain and cost effective; however, these benefits are often hampered by patient discomfort, difficulties in chewing, problems with pronunciation, and the process of generating acceptable facial expressions such as smiling or laughing. It has been noted that over time, nine out of 10 people will complain of difficulties with a mandibular denture1.
There are numerous over the counter products that offer a bandaid solution to some of these complications, but they never address the core problem; dentists, meanwhile, dedicate countless hours to adjustments and managing patient dissatisfaction.2
To compensate, denture wearers often change their daily routines and diets in ways that expose them to general health risks. With the greater focus today on the relationship between dentistry and systemic health, we recognize that edentulousness has a direct impact on patients’ overall health with problems ranging from psychological, to nutritional and digestive concerns. According to Dr. Carl Misch, studies demonstrate that complete tooth loss is associated with the increased presence of illness, citing that 28% of the edentulous population is required to take medicines for gastrointestinal disorders.3 Clearly this situation leaves dentists less than excited about proposing dentures as a viable solution. Some dentists may be delaying necessary tooth extractions, particularly in the mandibular arch, because they are well aware of poor retention of dentures and continual bone resorption.
There are, however, treatment options that can dramatically improve the patient experience with a lower denture and prevent bone resorption. Meijer et al., reported that patients with mandibular overdentures supported by implants are more satisfied when compared to patients who lack implant support.4 In the transformative McGill Consensus published in 2002, it was determined that mandibular dentures should be retained with a minimum of two implants, thereby helping to counter the effects of bone resorption and providing a more stable and retentive denture.5
The Innovation
Many patients have benefitted from newly adapted protocols for securing lower dentures using minimally invasive implant treatment. In particular, the narrow diameter, or mini implant, has made access to treatment vastly more attainable because of the reduced costs, reduced chairside time and more straightforward planning. The American Dental Association endorsed this treatment in 2004.6
One system in particular has taken measures to develop a protocol that compensates for ridge changes and bone resorption by cushioning the denture-ridge interface while optimizing patient comfort. Ten years of long-term clinical and university-based research support the ATLAS Denture Comfort Implant System (Dentatus, New York NY) as an excellent retentive system for lower dentures.
The hermetically retained liner is easy to maintain. Thus, patients express very high satisfaction while wearing their dentures and describe the ease with which their dentures are inserted and removed.7,8,9 The Tuf-Link silicone material provides cushioned support and stabilization of the denture with gentle, firm retention while effectively distributing the masticating forces on the ridge and implants. This is accomplished without housings, O-rings or adhesives and overcomes restrictions of parallelism, space, stress, and the other limiting obstacles of the edentulous arch. Patients do not suffer with the sore spots that are typically caused by a hard acrylic denture base rubbing against the sensitive gingival tissue.
The minimally invasive ATLAS procedure is generally performed without a surgical flap. ATLAS implants can be loaded immediately, and thus patients can leave the single-visit chairside procedure with a cushioned, comfortable, and stable denture.
The Technique
The ideal condition for the procedure requires the existing denture to have a functional fit in a repeated position on the existing ridge (Fig. 1). A quick, auto-cure reline with reduced flanges can prevent denture lift in functional and parafunctional movements.
FIGURE 1. Clinic case courtesy of Dr. Wolfram Bucking.

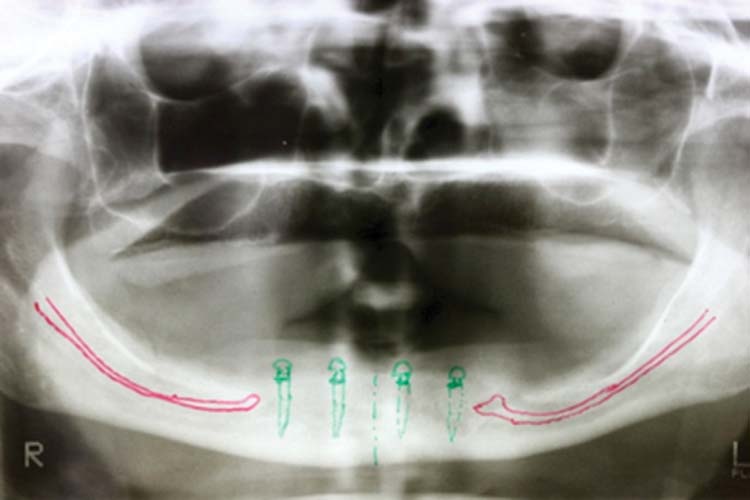
A panorex was used to plan the four Atlas Implant locations, anterior to the mental foramina for a balanced, cross-arch stabilization and retention (Fig. 2). The locations were then translated to the mucosa with a sterile marking pen.
FIGURE 2. Clinic case courtesy of Dr. Wolfram Bucking.

The Dentatus CePo Pilot Drill made the initial pierce through the gingival tissue (without rotation) indenting the bone to precisely locate the subsequent osteotomies (Fig. 3). In knife-edge ridges, a small window incision is made to flatten the bone to achieve a purchase point for the pilot drill (Fig. 4). The drills, operated at 1300-1500 RPM with coolant, were angled for implant placement within the bilk of bone. The osteotomies were prepared to full depth for the implant platform to seat in the mucosa. For implants wider than 1.8 mm diameter, the osteotomies are enlarged with the correspondingly marked drills to the pre-drilled depth.
FIGURE 3. Clinic case courtesy of Dr. Wolfram Bucking.

The manual carrier driver attached to the sterilized implant was used to safely transfer the implant to the osteotomies and to engage a few threads. The carrier driver was removed and the placement was continued with the right-angled handpiece driver (or with the winged manual driver which provides tactile feedback) to complete seating (Fig. 5). To obtain
good initial stability, an installation torque of 40 Ncm is recommended.
FIGURE 4. Clinic case courtesy of Dr. Wolfram Bucking.
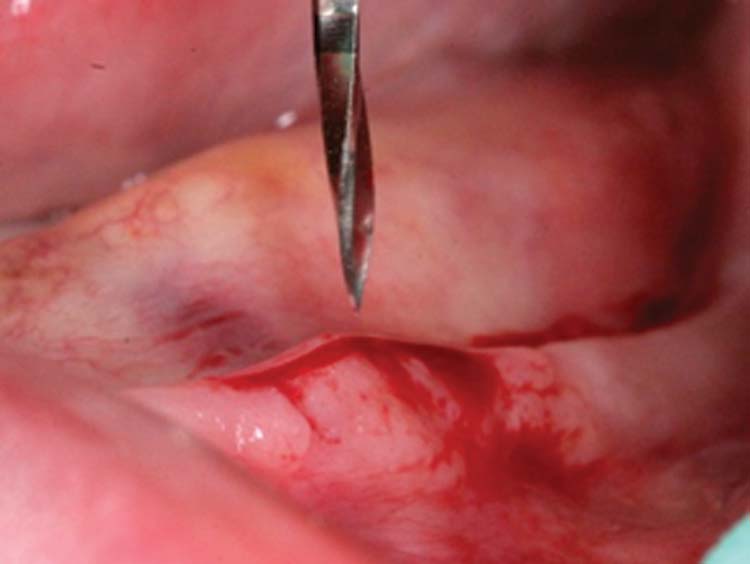
FIGURE 5. Clinic case courtesy of Dr. Wolfram Bucking.

To retrofit the prosthesis, a seam line outline was marked in the denture, approximately 2-3 mm below the flange extensions. This was extended up to the retromolar pads in a curved form for seamless liner adaptation. A series of three gauged burs created the undercut and 1 mm space within the denture (Fig. 6) for the Tuf-Link, such that it could fit securely around the heads of the implants (Fig. 7). Marking caps were placed on the Atlas Implants to transfer their positions in the denture (Fig. 8). The spherical cutting instrument indented the marked spaces allowing the denture to seat passively on the mandibular arch with the implants in place.
FIGURE 6. Clinic case courtesy of Dr. Wolfram Bucking.
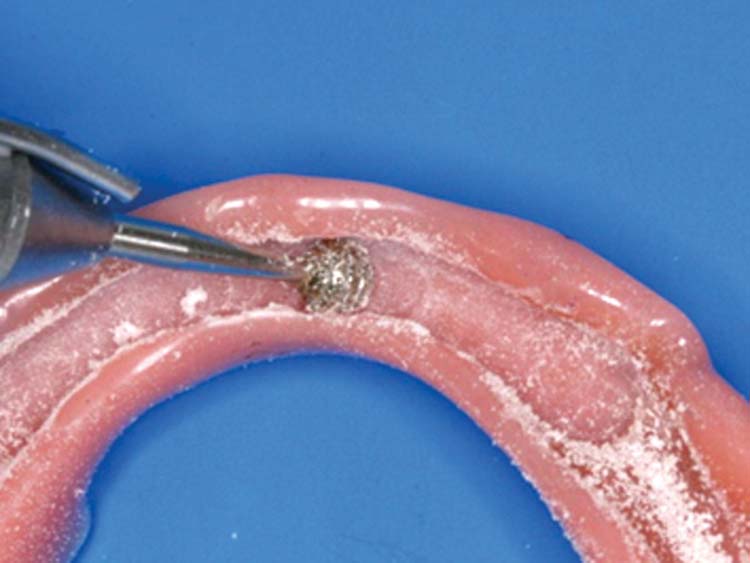
FIGURE 7. Clinic case courtesy of Dr. Wolfram Bucking.

FIGURE 8. Clinic case courtesy of Dr. Wolfram Bucking.
The practitioner injected sufficient silicone into the denture to create the necessary pressure for a dense, nonporous liner. The denture was inserted from the posterior direction, and guided forward with pulsating side motions. The patient was asked to contact their opposing arches and to hold the occlusion in place while the liner set (typically five minutes).
Once polymerization was complete, the denture was removed, and the liner gently lifted out of the denture base. The flash was cut away along the clearly delineated seam line. To reinsert the liner, it was first positioned at one end of the denture and guided into place with light finger pressure. Depending on the patient’s function and habits, the liner should remain resilient for 12–18 months (Figs. 9 and 10).
FIGURE 9. Clinic case courtesy of Dr. Wolfram Bucking.

FIGURE 10. Clinic case courtesy of Dr. Wolfram Bucking.

The Conclusion
With Atlas Denture Comfort, patients are assured of having prostheses that look and feel like their very own teeth. Patients experience healthier and better-looking smiles that are both comfortable and secure. Bone loss in the remaining ridges is decreased, and patients experience substantial relief from the pain and discomfort of ill-fitting dentures. The stabilization of prostheses gives patients a heightened quality of life that only comes from the confidence of being able to laugh, to speak and to eat like once before. OH
Oral Health welcomes this original article.
References:
1. Christesen CDS MWM Lecture 2005
2. Elena Preoteasa, DMD, PhD/Marina Imre, DMD, PhD/Cristina Teodora Preoteasa, DMD “A 3-Year Follow-up Study of Overdentures Retained by Mini–Dental Implants” JOMI, Volume 29 , Issue 5 September/October 2014 Pages 1170–1176
3. Misch,CE, Dental Implant Prosthetics, 2nd Edition p 757
4. Meijer HJA, Raghoebar GM,Van’t Hof MA, et al. Implant retained mandibular overdentures compared with complete dentures; a 5 years’ follow-up study of clinical aspects and patient satisfaction. Clin Oral Impl Res 1999; 10 (3): 238-244
5. Feine JS, Carlsson GE, et al. The McGill consensus statement on overdentures. Mandibular two-implant overdentures as first choice standard of care for edentulous patients. Gerodontology. 2002 Jul;19(1):3-4.
6. ADA Brochure on Mini Implants, 2004
7. Cho S-C, Froum S, Tai CH, et al. Immediate loading of narrow diameter implants in severely atrophic mandibles. Pract Proced Aesthet Dent. 2007;19(3):167-174.
8. LaBarre, Eugene; Ahlstrom, Robert H.; Noble, Warden H. “Narrow Diameter Implants for Mandibular Denture Retention”, CDA Journal, Volume 36, Number 4, Apr. 2008 pages 283-286
9. Tomasi, C.; Idmyr, B.-O.; Wennstrom, J.L. “Patient satisfaction with mini-implant stabilised full dentures. A 1-year prospective study”, Journal of Oral Rehabilitation. 2013
Follow the Oral Health Group on Facebook, Instagram, Twitter and LinkedIn for the latest updates on news, clinical articles, practice management and more!











