

The general dentist may often encounter patients that have undergone maxillofacial surgery at some point in the past. These patients may present with findings that include the presence of fixation hardware that is placed during surgical procedures. This hardware may not always be seen clinically. Consequently, radiological imaging is one of the key tools used to aid the general dentist in patient assessment and care. It is therefore important that practitioners be able to interpret radiographic imaging even though these images may present with findings that are not encountered on a regular basis.
Using a series of cases, the aim for this paper is to provide a simplified overview of the appearance of hardware placed during surgery both from a clinical and radiographic perspective.
In many situations, patients may be referred to dentists for the repair of fractured, avulsed or luxated teeth. These patients often present with other injuries which include maxillary, mandibular or alveolar fractures. These injuries may have been treated via open or closed reduction prior to referral. In closed reduction, the use of Erich arch bars is often utilized as an effective means to immobilize the mandible and maxilla. The arch bars are held in place through the use of stainless-steel wires that are passed around the bar and the teeth. The upper and lower bars are then connected through the use of more wires to achieve fixation (Fig. 1). They offer a cost-effective means of achieving fixation of specific non-displaced fractures of the mandible. However, the large disadvantage with this technique is the time it takes to place them as well as the risk of needle stick injury.
Fig. 1A

Fig. 1B

Fig. 1C

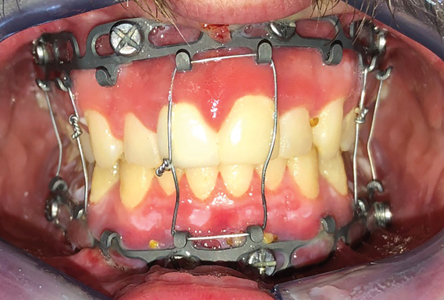
An alternative to arch bars are Intermaxillary fixation (IMF) screws. These screws come in many shapes and sizes. They are placed into the maxilla and mandible and are then connected with stainless steel wire so as to allow for immobilization during surgery in such procedures which include fracture repair and orthognathic surgery (Fig. 2). This technique offers several advantages over conventional arch bars in that they 1) shorten surgical time and increase OR efficiency and 2) significantly reduce to risk of needle stick injury.
Fig. 2A

Fig. 2B

However, IMF screws do also present with drawbacks. These include 1) cost 2) the risk of iatrogenic tooth root damage (Coburn, 2002) and 3) lack of versatility beyond the pure maintenance of occlusion as these screws cannot be used in situations that require stabilization of loose teeth or splinting fragments of the alveolar process (Cornelius et al., 2010).
An intermediate between arch bars and IMF screws is the hybrid arch bar system which utilizes screws rather than wires to anchor the arch bars to the maxilla and mandible (Fig. 3). The advantage of this system is that it allows for the increased efficiency compared to arch bars while at the same time providing strong, stable fixation across the maxillary and mandibular arches.
Fig. 3

In more complex fractures or in cases where a large bony defect is present, open surgical reduction and fixation is required. In these situations, MMF screws or arch bars are not enough.
In the past, the use of circumferential wires had been used to aid in the reduction of fractures where there was no stability in the teeth adjacent to the fracture segment (Maloney, 2015). These wires would be passed through the floor of the mouth and up through the buccal vestibule and anchored to the Erich arch bars to help reduce fractures as well as stabilize teeth adjacent to the fracture (Fig. 4). This technique was found to be especially useful in pediatric patients when tooth buds within the mandible did not allow internal fixation with plates and screws. In these situations, stability can be achieved with an acrylic splint fixed to the teeth and to the mandible with circummandibular wire (Sharma 2009).
Fig. 4

However, this technique has fallen out of favor as the use plates and screws offers superior stability and predictability. These titanium plates and screws are utilized to fixate two opposing bony segments. This provides maximum functional stability and allow healing. Heavier plates with bicortical screws are placed along the inferior border of the mandible (Fig. 5). In order to avoid separation of the fracture superiorly, additional smaller plates are placed with the use of monocortical screws. These screws are often shorter in length (5-6mm). Therefore, they only penetrate through the buccal cortex, thereby causing no damage the dentition even though they may appear to be hitting the teeth on radiographic imaging.
Fig. 5


The same principles are applied to several other procedures including orthognathic surgery and reconstructive surgery. In orthognathic surgery, dento-facial deformities and associated malocclusion are treated through osteotomies in the maxilla and mandible in order to allow for movement of the maxilla-mandibular complex in 3 dimensions. Although several osteotomy designs exist, the Le Fort osteotomy, Bilateral Sagittal Split osteotomy, and Genioplasty are the most common techniques utilized. Once the osteotomies are performed and the bones moved into the correct position, plates and screws are used again to achieve fixation and allow for healing. In the maxilla and chin, monocortical screws are used to hold plates in place. In the mandible however, bicortical screws are utilized to achieve fixation at the sagittal split osteotomy sites (Fig. 6). The screws are placed with the position of the inferior alveolar nerve in mind. They are placed in a manner so as to not compromise the nerve. However, on imaging, this can be somewhat deceiving as they often appear to be placed very close or into the nerve canal even though, in reality, they are not impinging on the canal.
In certain clinical scenarios where there are large movements made of the maxilla and mandible, bone grafts are often used to provide stability and prevent against relapse. In order to stabilize these grafts, even more hardware is often utilized so as to provide stability (Fig. 6).
Fig. 6

Another important consideration in oral maxillofacial surgery is that. Because access is limited, fractures are sometimes approached via a transcutaneous approach through the neck. In these situations, several anatomical structures are encountered. These including nerves and blood vessels. Blood vessels will sometimes interfere with access to the surgical site. Therefore, they are ligated so as 1) gain better surgical access 2) control hemorrhage during surgery or 3) to prevent a bleed in the post-surgical phase. In order to achieve this, vascular clips are utilized. They are small titanium clamps that are applied around the vessels. They can be used in the place of sutures to achieve hemostasis. They are designed such that two parallel bars with a gap between them are placed around a blood vessel with a clip applicator. When activated the bars act to compress the tissue. They have several surgical applications as they can also be used to outline tumor margins (Bitterman et al., 2015).
Because many vessels are often encountered during surgery, it is not uncommon to see several dozens of these clips on radiographic imaging. They are designed to stay for the lifetime of the patient (Fig. 7).
Fig. 7

Distraction osteogensis is an extremely useful technique for gradually achieving large movement advancements for facial reconstruction, with the added advantage of creating new bone and soft tissue as it is performed. In the case illustrated, two dentoalveolar transport discs were created through the use of segmental osteotomies, which were then transported across the anterior bilateral alveolar and palatal defect to achieve primary union of bone and soft tissue (Figs. 8 & 9). In its wake, the area behind the transport discs fill with new distracted bone regenerate, and new additional soft tissue. This not only eliminates the requirement for bone and soft tissue grafting, but adds to the stability of the repositioned segments as bone consolidates behind the transport discs. While screw fixation may appear on two-dimensional view to interfere with dental anatomy, engagement of only the outer cortex, combined with placement designed to avoid root anatomy, ensures tooth vitality (Figs. 9 & 10).
Fig. 8


for distraction osteogenesis, to correct a
patient with a bilateral cleft alveolus & palate
deformity ; a) pre-distraction following
reduction of the premaxilla, osteotomy
and placement of distraction appliances; b)
Post-distraction with the anterior alveolar
and palatal defect closed primarily through
the activation of the appliances and creation
of new hard and soft tissues.
Fig. 9

two distractors in place immediately prior
to beginning the bone distraction process.
Intra-osseous screw fixation was used to
secure the posterior footplate of the device
in stable bone, and the anterior footplate
to the dentoalveolar transport segment to
be distracted. Note also the plate fixation
hardware in the anterior mandible as a
genioplasty advancement was performed
simultaneously.
Fig. 10


As illustrated in this paper, a wide array of hardware is used in oral and maxillofacial surgery, which can appear unusual on radiographic appearance, if not disruptive to the dental anatomy. In this article, our goal was to provide a brief summary of some of the applications of these materials and to review for purposes of interpretation their appearance on radiographic imaging. In doing so, the hope is to provide the reader with an overview of what they can expect to encounter in surgical patients that present to their practice.
Oral Health welcomes this original article.
References
- Bittermann G, Voss P, Duttenhoefer F, Zimmerer R, Vach K, Metzger MC. The validity of surgical clips as radiographic markers for the tumour resection cavity in head and neck cancer treatment. J Craniomaxillofac Surg. 2015;43(6):758–762.
- Cornelius CP, Ehrenfeld M. The Use of MMF Screws: Surgical Technique, Indications, Contraindications, and Common Problems in Review of the Literature. Craniomaxillofac Trauma Reconstr. 2010;3(2):55–80. doi:10.1055/s-0030-1254376
- Coburn DG, Kennedy DW, Hodder SC. Complications with intermaxillary fixation screws in the management of fractured mandibles. Br J Oral Maxillofac Surg. 2002;40(3):241–243
- Maloney, K. “Circummandibular Wires for Treatment of Dentoalveolar Fractures Adjacent to Edentulous Areas: A Report of Two Cases.” Craniomaxillofacial trauma & reconstruction vol. 8,3 (2015): 246-50.
- Miloro, M., & Peterson, L. J. (2012). Peterson’s principles of oral and maxillofacial surgery. Shelton, CT, People’s Medical Pub. House-USA.
- Sharma S, Vashistha A, Chugh A, Kumar D, Bihani U, Trehan M, et al. Paediatric mandibular fractures: A review.
Int J Clin Pediatric Dent 2009;2:1-5.
About The Authors
 Dr. Nadir Elias is a third-year resident in the Oral and Maxillofacial Surgery program at the University of Toronto. He obtained his dental degree from Nova Southeastern University in 2014. He then completed a General Practice Residency at Advocate Illinois Masonic Medical Centre in Chicago, Illinois. He then pursued a year-long surgery-based residency at Newark Beth Israel Medical Centre in Newark, New Jersey.
Dr. Nadir Elias is a third-year resident in the Oral and Maxillofacial Surgery program at the University of Toronto. He obtained his dental degree from Nova Southeastern University in 2014. He then completed a General Practice Residency at Advocate Illinois Masonic Medical Centre in Chicago, Illinois. He then pursued a year-long surgery-based residency at Newark Beth Israel Medical Centre in Newark, New Jersey.
 Dr. Iain A. Nish is a graduate of The University of Toronto in both Dentistry and Oral & Maxillofacial, and subsequently completed a Fellowship in Plastic & Reconstructive Surgery in Basel, Switzerland. Dr. Nish was a Staff OMFS at Sick Kids Hospital for two decades, with a particular interest in reconstructive surgery as applied to patients with Cleft Lip & Palate and Craniofacial deformities.
Dr. Iain A. Nish is a graduate of The University of Toronto in both Dentistry and Oral & Maxillofacial, and subsequently completed a Fellowship in Plastic & Reconstructive Surgery in Basel, Switzerland. Dr. Nish was a Staff OMFS at Sick Kids Hospital for two decades, with a particular interest in reconstructive surgery as applied to patients with Cleft Lip & Palate and Craniofacial deformities.
 Dr. Bruce Pynn is Oral Health’s editorial board member for oral and maxillofacial surgery. He maintains a private practice in Thunder Bay, ON. He is an Associate Professor, North Ontario School of Medicine, Lakehead University, and Chief of Dentistry, Thunder Bay Regional Health Sciences Center.
Dr. Bruce Pynn is Oral Health’s editorial board member for oral and maxillofacial surgery. He maintains a private practice in Thunder Bay, ON. He is an Associate Professor, North Ontario School of Medicine, Lakehead University, and Chief of Dentistry, Thunder Bay Regional Health Sciences Center.
RELATED ARTICLE: Oral and Maxillofacial Surgery – What is That?
Follow the Oral Health Group on Facebook, Instagram, Twitter and LinkedIn for the latest updates on news, clinical articles, practice management and more!










