
Abstract
Patients who are diagnosed with MRONJ while being treated with bone modifying agents(BMAs) at oncologic doses, there is insufficient evidence to support or refute the discontinuation of BMAs. Administration of the BMA may be deferred at the discretion of the treating physician, in conjunction with discussion with the patient and the dental specialist. The importance of communication with the dental specialist , patient and treating oncologist on appropriate management strategy is key. Effective management of MRONJ in the oncology patient does not solely rely on the expectation that lesion resolution is the only acceptable outcome.

Medication-related osteonecrosis of the jaw (MRONJ) is defined as exposed bone or bone that can be probed through an intraoral or extra oral fistula in the maxillofacial region and that does not heal within 8 weeks and that occurs in a patient who has received a bone-modifying agent (BMA) or an angiogenic inhibitor agent and has no history of head and neck radiation.1,2 The condition may involve the mandible or the maxilla.
Table 1 lists the common medication associated with risk of MRONJ. BMAs that have been linked with MRONJ principally include bisphosphonates and denosumab. (Table 2)
Table 1

Table 2

BMAs are a key component of the management of patients with cancer with skeletal metastases, prevention of osteoporosis, reduction in the risk of bone metastases and treatment of hypercalcemia of malignancy. These medications provide a number of clinical benefits, including a reduced incidence of skeletal-related events (eg, pathologic fractures and spinal cord compression) and reduced need for radiation or surgery to bone. Use of BMAs is associated with MRONJ, which occurs in approximately 1% to 9% of patients with advanced cancer. MRONJ can be challenging to treat and can cause significant pain and reduced quality of life. Many studies have established that preventive oral care methods combined with effective oral health practices are associated with a lower rate of MRONJ.3-16
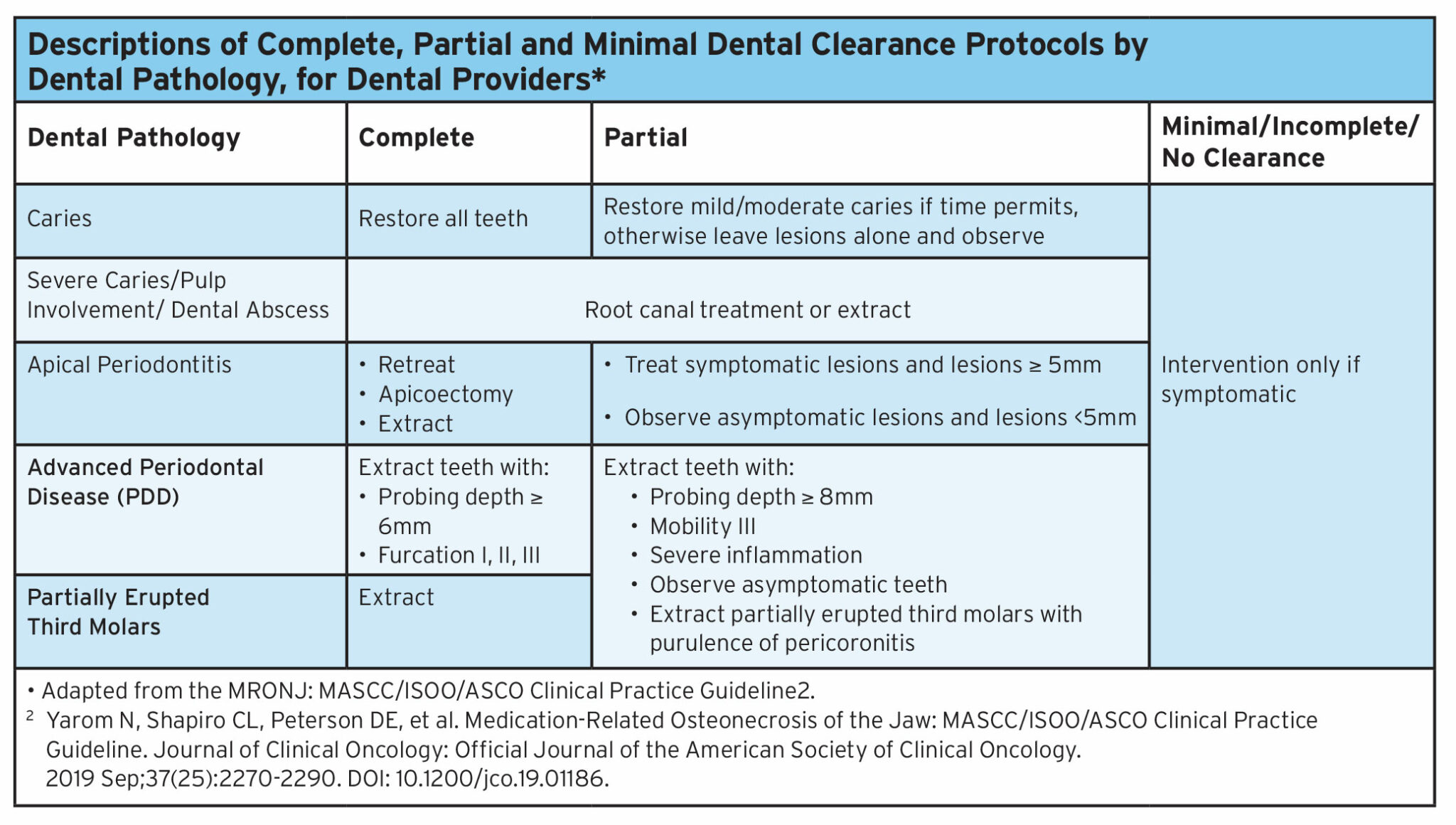
The importance of collaboration among the cancer care team, dentists, and dental Specialists is essential in increasing the awareness and importance of compliance to oral care and pre-treatment dental examination. Dentists may be community based or hospital based and are the providers who typically complete the pre–cancer therapy dental evaluation and provide long-term preventive management. Dental specialists are dentists with expertise in the clinical management of MRONJ. A pre-cancer therapy dental evaluation is similar to a comprehensive dental examination on a routine visit with the increased awareness of dental clearance based on the patients overall disease stability and prognosis. (Table 3) A complete dental clearance protocol for instance would be recommended in a patient with over all stable disease or those prescribed a BMA for the prevention of osteoporosis or reduction in the risk of bone metastases. A partial clearance protocol would apply to a patient commencing a BMA with skeletal metastases but not end of life, and the minimal clearance dental protocol would be reserved for patients requiring symptom management and avoidance of risk for acute infection. The International Society of Oral Oncology/ Multinational Association of Supportive Care in Cancer and the American Society of Clinical Oncology ( ISOO/MASCC and ASCO) recommends that patients on BMA’s be seen on oral follow up by the community dentist every 6 months and in the instances where an MRONJ is noted or suspected, a referral to a Dental Specialist with communication to the oncologist. Lesion stability should be reported and follow up should be every 8 weeks with the dental specialist until the lesion has resolved. At the time the lesion has resolved the patient can resume routine 6 month follow up with their community dentist.
Table 3
Modifiable risk factors associated with MRONJ should be addressed as early as possible by all members of the multidisciplinary team. These risk factors include poor oral health, invasive dental procedures carried out after commencement of a BMA., ill-fitting dentures, uncontrolled diabetes mellitus, and tobacco use.
Historically, full mucosal healing was used as the prototypic indicator to reflect the stability of the MRONJ lesion; however, it is now recognized that the decision to alter therapy based on the absence of full mucosal healing of an MRONJ lesion may not benefit the patient. In some cases, lesion stability rather than full healing may be an acceptable outcome. The proposed outcome categories as published in the MASCC/ISOO/ASCO MRONJ Practice Guideline are intended to complement the AAOMS staging criteria.
During the course of MRONJ treatment, the dentist/dental specialist should communicate with the medical oncologist the objective and subjective status of the lesion – resolved, improving, stable, or progressive. The clinical course of MRONJ may affect local and/or systemic treatment decisions with respect to the cessation or recommencement of BMAs.
Clinical case comparison
Subject A Patient presents with a fistula probable to bone realized 12 weeks post dental extraction. The patient is asymptomatic with no history of purulence but referred to the dental specialist from the family dentist. Patient’s medical history includes metastatic prostate cancer with past history of fracture. His ECOG status is 1. After an 8-week follow-up with this patient the lesion is still present and asymptomatic. (Figure 1A)
Fig. 1A

Subject B Patient presents with a medical history of multiple myeloma that is poorly controlled. The patient is referred to the dental specialist from the medical oncologist for MRONJ management. His ECOG status is 3. The patient does not complain of pain or trauma to the oral cavity but pain generalized prior to commencement of BMA therapy 12 months ago. After 8 week follow up you note no changes in lesion size or symptoms. (Figure 1B)
Fig. 1B

Taking aside the aspect of lesion extent and size, radiographic findings and focusing on lesion status, both of these lesions would be considered clinically stable but not resolved. Based on each of the patients medical status, both Subjects A and B are benefiting from their BMA therapy; Subject A in management of future fracture risk, Subject B in management of osteopathic pain from the myelomatous disease. Both cases exemplify the need to address this aspect of management over the focus for full resolution of the lesion.
In conclusion, patients who are diagnosed with MRONJ while being treated with BMAs, there is insufficient evidence to support or refute the discontinuation of BMAs. Administration of the BMA may be deferred at the discretion of the treating physician, in conjunction with discussion with the patient and the oral health provider. The importance of communication with the dental specialist , patient and treating oncologist on management strategy is key. Effective management of MRONJ in the oncology patient does not solely rely on the expectation that lesion resolution is the only acceptable outcome.
A full copy of the MASCC/ISOO/ASCO Clinical Practice Guideline for Medication-Related Osteonecrosis of the Jaw can be downloaded at https://doi.org/10.1200/JCO.19.01186 Ontario Health Symptom Management to Oral Care: MRONJ can be downloaded at file:///C:/Users/dsaunders/Downloads/Medication-RelatedOsteonecrosisOfTheJawAlgorith
Oral Health welcomes this original article.
References
- Khan A, Morrison A, Cheung A, et al: Osteonecrosis of the jaw (ONJ): Diagnosis and management in 2015. Osteoporos Int 27:853-859, 2016.
- Ruggiero SL, Dodson TB et al: American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw — 2022 update. J Oral Maxillofac Surg :1-24, 2022.
- Gabbert TI, Hoffmeister B, Felsenberg D: Risk factors influencing the duration of treatment with bisphosphonates until occurrence of an osteonecrosis of the jaw in 963 cancer patients. J Cancer Res Clin Oncol 141:749-758, 2015.
- Guarneri V, Miles D, Robert N, et al: Bevacizumab and osteonecrosis of the jaw: Incidence and association with bisphosphonate therapy in three large prospective trials in advanced breast cancer. Breast Cancer Res Treat 122:181-188, 2010.
- Haidar A, Jønler M, Folkmar TB, et al: Bisphosphonate (zoledronic acid)-induced osteonecrosis of the jaw. Scand J Urol Nephrol 43:442-444, 2009.
- Kajizono M, Sada H, Sugiura Y, et al: Incidence and risk factors of osteonecrosis of the jaw in advanced cancer patients after treatment with zoledronic acid or denosumab: A retrospective cohort study. Biol Pharm Bull 38:1850-1855, 2015.
- Mavrokokki T, Cheng A, Stein B, et al: Nature and frequency of bisphosphonate-associated osteonecrosis of the jaws in Australia. J Oral Maxillofac Surg 65: 415-423, 2007.
- Merigo E, Manfredi M, Meleti M, et al: Bone necrosis of the jaws associated with bisphosphonate treatment: A report of twenty-nine cases. Acta Biomed 77:109-117, 2006.
- Palaska PK, Cartsos V, Zavras AI: Bisphosphonates and time to osteonecrosis development. Oncologist 14:1154-1166, 2009.
- Patel CG, Yee AJ, Scullen TA, et al: Biomarkers of bone remodeling in multiple myeloma patients to tailor bisphosphonate therapy. Clin Cancer Res 20:3955-3961, 2014.
- Pires FR, Miranda A, Cardoso ES, et al: Oral avascular bone necrosis associated with chemotherapy and biphosphonate therapy. Oral Dis 11:365-369, 2005.
- Rabelo GD, Assunção JNR Jr, Chavassieux P, et al: Bisphosphonate-related osteonecrosis of the jaws and its array of manifestations. J Maxillofac Oral Surg 14:699-705, 2015.
- Saad F, Shore N, Van Poppel H, et al: Impact of bone-targeted therapies in chemotherapy-naïve metastatic castration-resistant prostate cancer patients treated with abiraterone acetate: Post hoc analysis of study COU-AA-302. Eur Urol 68:570-577, 2015.
- Sim IeW, Sanders KM, Borromeo GL, et al: Declining incidence of medication-related osteonecrosis of the jaw in patients with cancer. J Clin Endocrinol Metab 100:3887-3893, 2015.
- Vidal-Real C, Pérez-Sayá ns M, Suá rez-Peñaranda JM, et al: Osteonecrosis of the jaws in 194 patients who have undergone intravenous bisphosphonate therapy in Spain. Med Oral Patol Oral Cir Bucal 20:e267-e272, 2015.
- Walter C, Grötz KA, Kunkel M, et al: Prevalence of bisphosphonate associated osteonecrosis of the jaw within the field of osteonecrosis. Support Care Cancer 15:197-202, 2007.
- Yarom N, Shapiro C, Saunders D et al.: Medication- Related Osteonecrosis of the Jaw: MASCC/ISOO/ASCO Clinical Practice Guideline. J Clin Oncol 37.
About the Author
 Deborah Saunders is the medical director of the Department of Dental Oncology at the North East Cancer Centre and Associate Professor at the Northern Ontario School of Medicine in Sudbury Ontario. Dr. Saunders is the immediate past president of the International Society of Oral Oncology and senior author of the Clinical Practice Guideline in collaboration with the Multinational Association of Supportive Care in Cancer (MASCC)/International Society of Oral Oncology (ISOO) and the American Society of Clinical Oncology (ASCO).
Deborah Saunders is the medical director of the Department of Dental Oncology at the North East Cancer Centre and Associate Professor at the Northern Ontario School of Medicine in Sudbury Ontario. Dr. Saunders is the immediate past president of the International Society of Oral Oncology and senior author of the Clinical Practice Guideline in collaboration with the Multinational Association of Supportive Care in Cancer (MASCC)/International Society of Oral Oncology (ISOO) and the American Society of Clinical Oncology (ASCO).










