
Figure 1

Figure 2

Dental implants have been the treatment solutions for replacing missing teeth for many years. Their use has been well documented and accepted as a predictable method for teeth replacement.1,2 With the increasing use of dental implants in last few decades, the number of complications resulting from such usage has also increased. Dental practitioners must learn to recognize these complications and be ready to manage them in their practice.
Dental complications have been described and published in the literature for many years now. Goodacre et al have categorized them based on the type of prosthesis, arch location, pre-prosthetic, post-prosthetic, implant length and bone quality.3 He also categorized them as surgically related, peri-implant related and/or mechanically related implant complications. In other published article, dental implant complications have been divided into either biological or hardware related complication. Biological complications relate to those surrounding soft and hard tissue. Hardware complications relate to implant and prosthetic components of the restorations.4
Commonly used dental instruments for screw removal:
Figure 3

Explorer.
Figure 4

Curved hemostat.
Figure 5

Ultrasonic scaler.
Figure 6

Spoon excavator.
Figure 7

Round bur.
Hardware related complications, specifically implant screw loosening has been cited as the most common complication for a single tooth implant.5 Frequent screw loosening sometimes can lead to screw fracture. Goodacre et al reported an incidence of prosthetic gold screw fracture of up to 19% and abutment screws fracture of up to 8%.6 Screw loosening has been attributed to various factors. These factors can range from inadequate treatment plan and design, component misfit, inadequate screw tightening, excessive loading, and/or inadequate screw design.7 Inadequate treatment design may be related to patient assessment and inadequate treatment planning resulting from insufficient number and location of implants. Component misfit can be related to inaccurate framework leading non-passive superstructures. The passivity of the superstructures relies on an accurate understanding of dental materials and recognizing the errors caused by stone expansion, wax distortion, investment expansion, metal shrinkage and acrylic/porcelain shrinkage. These understandings should translate into proper use of clinical and laboratory techniques as well as using accurate materials. Inadequate screw tightening is another reason that can lead to loose screws or fractured screws. Not all screws are created equally nor are they designed to be all torqued to 32Ncm. Proper torque value based on manufacturers’ instruction should be followed. Excessive loading can be due to inadequate occlusal design or parafunctional habits such as bruxism. Excessive crown height or excessive cantilever lengths leading to increasing moment force can also be a contributing factor. Inadequate screw design affecting preload can be due to poor screw head design, inadequate metal composition, and surface condition and thread design.
Unfortunately, in the case where implant screw loosening eventually lead to screw fracture, dealing with such complication can be quite challenging. Many articles have been published to discuss their unique techniques in retrieving broken screws. This article will review some of the published methods of retrieving fractured implant screws as well as reviewing some clinical cases and consideration for fractured screw retrievals.
Most published articles will discuss that if there is a fractured implant screw, the treatment option is to retrieve the screw or to remove the implant. The more conservative solution is to attempt to retrieve the screw fragment so the implant can be reused again. One consideration is to distinguish if the fragment is located above the implant body or inside the implant body. If the broken screw is visible and above the implant body, most authors will discuss the technique of using a hemostat or a sharp explorer applied to the fragment in a counter clockwise direction to retrieve it.8
However, if the broken screw is embedded inside the implant body, it may be more challenging to retrieve the screw fragment. There is also an inherent risk of damaging the internal threads of the implant body. Visibility and access will become more difficult as well. Most would agree the need to isolate the area to improve visibility. Some techniques are based on commercially available retrieval system, requiring the clinician to purchase the specific drill sets to retrieve the broken screws. Other techniques attempt to modify commonly available dental tools to allow screw retrievals. Most approaches would often start with the more conservative methods. These methods may include also using a sharp explorer to loosen up the screw fragment by wedging the fragment in a counter clockwise direction. Others would recommend roughening the exposed screw fragment and to make some type of indentation with a rotary instrument before using a sharp explorer to engage the fragment. It is believed that by modifying the exposed screw fragment, there is better engagement with the rotary instrument in applying a reverse torque in order to back up the fractured fragment. In some cases, Gooty et al. recommended using an ultrasonic scaler to loosen up the fragment if other instruments have not worked.9 Satwalekar P et al. recommended modifying a spoon excavator to engage the fractured fragment after making a groove on the screw fragment.10
It is also important to realize that if the screw fragment does not loosen up, some authors suggest that there may have been internal threads damage during previous attempts of screw retrieval hindering the path that the fragment may need to travel. Some authors advocate intentionally drawing the fragment further into the implant body by applying clockwise direction and then re-tapping the few threads above the fragment before attempting to back it out.11 It is also suggested multiple retrieval attempts may leave behind metal bits in the implant body preventing proper engagement. As a result, copious irrigations should be carried throughout the procedure to clean out these metal bits and to avoid overheating the site.
Commercially Available Kits for Screw Removal:
Figure 8

Picture of Fork Shaped End Instrument.
Figure 9

Nobelbiocare retrieval kit.
Figure 10

Salvin Implant Rescue kit.
Figure 11

Screw Removal Kit OSSVK+detail.
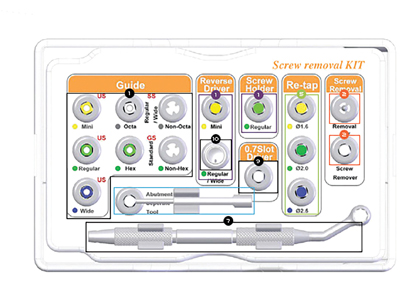
Figure 12

Neobiotech Screw Removal kit.
If the more conservative approach has proven not to work, then there are some commercially available retrieval tools and systems for purchase. Many major implant companies will carry their own if requested. Some dental implant suppliers have also created their own implant and screw rescue or retrieval kits for purchase. Many of these kits can be quite expensive. But many of them will carry similar items for the retrieval attempts. Most of these commercially available systems will include a set of drills of different dimensions, shapes and lengths. The goal is to engage the broken fragment and then applying reverse torque to back up the fragment. The kit will also include a set of drill guides or drill “sleeves”. The goal is to align or angulate the drill in proper axial direction to the implant to minimize damage to the internal threads of the implants. Lastly, the kit will usually include a set of re-tapping tools and the goal is to re-thread the internal structure of the implant should there be any damage during the retrieval process. Yilmaz and Iman have both discussed a fork shaped end instrument from Astratech specially designed to engage the screw fragment. Once engaged the instrument can be placed in a slow speed hand piece and apply a reverse torque to back up the loose fragment.12 Nergiz et al. described using IMZ TwinPlus Repair Set K 3.3 from Dentsply Friadent.13 Luterbacher et al described the service set available for the ITI system.
Some other practitioners have described in their articles their unique methods of retrieving the broken screw. Instead of relying on the expensive commercially available retrieval systems, they rely on more of the commonly available instruments in a dental office. Williamson et al first described a technique where a small round bur is used to modify the superior portion of the broken screw into a slot like configuration.14 Then another round bur is modified to shape like a slot driver where it can be placed in a slow speed hand piece and applying a reverse torque to back up the loose screw fragment.
The use of modified rotary instruments for screw retrieval can be cost saving and convenient. However, it does carry the risk of damaging the internal threads if the bur is applied at an off angle to the implant’s position. To minimize this risk, Yoon et al advocated customizing a drill guide using conventional impression post.15 In this article, he described converting an impression post using auto-polymerizing resin as a way to stabilize it over the implant without the screw. In essence, the space through the impression post that would have normally been occupied by a screw is now a channel for the rotary instruments for screw retrieval.
In the case where the broken screws cannot be retrieved or there has been damage to the internal structure of the implant rendering it non restorable, Canpolat et al have advocated making a custom dowel and cementing a locator abutment or something similar inside the implant body to be used as an overdenture abutment.16 Pipko et al also suggested a similar approach of fabricating a cast dowel core to support a single implant crown restoration.17
Case 1
This is a patient who presented to the clinic with splinted implant crowns that fractured off the implants. Examination and radiographs revealed the splinted crowns completely separated from the implants. Screw fragments were visible above the implants and were noted to be loose. A hemostat was used to secure the fragments separately and slowly rotated in the counter-clockwise direction to retrieve both fragments. The other fragments remained inside the crowns and have been removed through the access holes. It was noted however that with the new screws that were ordered, they did not fit through the screw channels of the implant crowns. It was discovered that the channels for the screws might have been distorted during the process of screw fracture. The case was sent to the lab for further evaluation and the screw channels had to be adjusted until the screws can fit into them again. The splinted implant crowns were later re-inserted and torqued to 32Ncm.
Case 1:
Figure 13

Figure 14

Figure 15

Case 2
This is a patient referred to remove an implant bridge 36-x-34. The prosthetic screw at implant site 36 was stripped and the patient also had limited mouth opening. Upon evaluation, an initial attempt was made to remove the stripped screw using conservative methods. However, with the limited mouth opening, that initial attempt was proven to be unsuccessful. It was later decided to enlarge the screw access opening on the occlusal surface to improve visibility. This is important especially for someone with limited mouth opening. The larger than normal access will allow the screwdriver or instruments to have greater freedom of maneuvering over the site for retrieval. In this case it was later noted there was binding between the walls of access opening and the screw. A ring of space was created surrounding the broken screw and slot like configuration created on the exposed screw. The bridge eventually became loose and it was removed to allow for better visibility. After the bridge was removed, the screw remained inside the body of the implant body. It was later removed with using a hemostat.
Case 2:
Figure 16

Figure 17

Figure 18

Figure 19

Case 3
This is a patient referred for screw removal. According to the history, the restorative crown was torqued over the suggested value. The resulting screw snapped off at the level of the abutment. This is an implant that has a morse taper along with the screw connection. During the examination phase, it was discovered that the abutment screw was flushed with the abutment. An attempt was made to create a slot configuration with the abutment screw. But it was proven to be ineffective due to the small available surface area. The decision was later made to forgo the abutment. The top portion of the abutment was reduced and flattened intentionally to remove previously made scratches. A ring of space was created around the broken screw. A slot configuration was created and the entire abutment was removed using a slot driver by applying a counter clockwise direction. The implant was later restored with a screw retained implant crown.
Case 3:
Figure 20

Figure 21

Figure 22

Continuous screw loosening may eventually lead to screw fracture. As a result, the dental practitioner should understand their causes and provide a solution to minimize the risk of further screw loosening and fracture. Some of these solutions would be based on proper patient selection, proper implant site selection aimed at decreasing moment force. Other methods would be aimed at providing a more accurate framework using techniques to counteract the errors inherent in the limitation of dental materials. Lastly, proper screw tightening and favourable occlusal scheme are important in minimising the risk of screw loosening and screw fractures. Implant screw fractures can be a challenge to manage clinically. Published articles that discussed suggested techniques have been reviewed here. The more conservative approach should be attempted first before considering the more invasive non-reversible procedures. There are many commercially available screw retrieval kits available for purchase. Alternatively, one may consider referring these cases out to the local prosthodontist for screw retrieval. It is important to preserve the internal structure of the implant intact in order to maintain its restorability. In any case, proper treatment planning and a good understanding of dental materials are paramount to avoid this type of implant complication. OH
Published Articles on Techniques in Retrieving Implant Screws:

Oral Health welcomes this original article.
References
- Balshi TJ: Preventing and resolving complications withosseointegrated implants. Dent Clin North Am 1989;33:821-868
- Nergiz I, Schmage P, Shahin R: Removal of a fractured implantabutment screw: a clinical report. J Prosthet Dent 2004;91:513-517
- Goodacre CJ, Kan JY, Rungcharassaeng K: Clinical complications of osseointegrated implants. J Prosthet Dent 1999;81:537-552
- Aglietta M, Siciliano VI, Zwahlen M, et al: a systematic review of the survival and complication rates of implant supported fixed dental prostheses with cantilever extensions after an observation period of at least 5 years. Clin Oral Implants Res 2009;20:441-451
- Canpolat C, Ozkurt-Kayahan Z, Kazazoglu E: Management of a fractured implant abutment screw: a clinical report. J Prosthodont 2014;23:402-405
- Luterbacher S, Fourmousis I, Lang NP, et al: Fractured prosthetic abutments in osseointegrated implants: a technical complication to cope with. Clin Oral Implants Res 2000;11:163-170
- Satwalekar P, Chander KS, Reddy BA, et al: A simple and cost effective method used for removal of a fractured implant abutment screw: a case report. J Int Oral Health 2013;5:120-123
- Williamson RT, Robinson FG: Retrieval technique for fractured implant screws. J Prosthet Dent 2001;86:549-550
- Yilmaz B, McGlumphy E: A technique to retrieve fractured implant screws. J Prosthet Dent 2011;105:137-138
- Walia MS, Arora S, Luthra R, et al: Removal of fractured dental implant screw using a new technique: a case report. J Oral Implantol 2012;38:747-750
- Cranin AN, Dibling JB, Simons A, et al: Report of the incidence of implant insert fracture and repair of Core-Vent dental implants. J Oral Implantol 1990;16:184-188
- Misch CE: Contemporary Implant Dentistry (ed 2). St. Louis, Mosby, 1999, pp. 580-582
 Dr. Beatrice Leung received her Doctor of Dental Surgery degree at the University of Toronto. Following graduation, she moved to Boston to complete a year of General Practice Residency at the Boston Medical Center. She then completed her three year Prosthodontics Residency Program as well as a Master of Public Health at the University of Pittsburgh. She has been in private practice in midtown Toronto and the York region for over 12 years. During this time, she has taught Prosthodontics to both graduate and undergraduate students at the University of Toronto as well as a staff Prosthodontist in the Implant Prosthodontic Unit at the Faculty. Dr. Leung can be reached at the following contact information: 39 Pleasant Boulevard, Lower Level, Toronto, ON, M4T 1K2, 416-927-9085. Email: drleung@drbeatriceleung.ca. Web Address: www.drbeatriceleung.ca
Dr. Beatrice Leung received her Doctor of Dental Surgery degree at the University of Toronto. Following graduation, she moved to Boston to complete a year of General Practice Residency at the Boston Medical Center. She then completed her three year Prosthodontics Residency Program as well as a Master of Public Health at the University of Pittsburgh. She has been in private practice in midtown Toronto and the York region for over 12 years. During this time, she has taught Prosthodontics to both graduate and undergraduate students at the University of Toronto as well as a staff Prosthodontist in the Implant Prosthodontic Unit at the Faculty. Dr. Leung can be reached at the following contact information: 39 Pleasant Boulevard, Lower Level, Toronto, ON, M4T 1K2, 416-927-9085. Email: drleung@drbeatriceleung.ca. Web Address: www.drbeatriceleung.ca
RELATED ARTICLE: Full Arch Implant Rehabilitation: Parafunctional Problems And Solutions








