
Successful dental implant surgery and subsequent prosthetic restoration require careful consideration and precise execution, whether replacing a single tooth or rehabilitating a full arch. Successful implants can function reliably for many years, effectively replacing natural teeth. Poorly positioned implants, on the other hand, will often fail and/or cause further functional complications as well as aesthetic problems.1
Digital technologies are evolving to promote prosthetically-driven workflows specifically to address these concerns. CBCT and intraoral scanning provide the surgeon with high-resolution, detailed anatomic information that allows for the planning necessary to achieve both surgical and restorative goals. In order to maximize their clinical benefit, these technologies require an accurate transfer from preoperative planning to surgical execution. Static guides improve implant accuracy but may constrain the surgeon’s freedom to respond to altered anatomic conditions or new clinical insights as they emerge intraoperatively.2 The surgical guide fabrication process can reduce practice efficiency, delaying the planning-to-surgery protocol, thus negatively impacting the patient’s perception of continuous treatment. The practitioner must leverage the technological innovations in imaging and planning to meet patient demands for both expeditious treatment pathways and flawless function and aesthetics.
The goal is to extend clinical expertise through technology that augments accuracy and efficiency in dental implant surgery3-6 by expanding the benefits of digital imaging and planning through surgical precision. The Yomi robotic guidance platform (Neocis, Miami FL) increases implant placement predictability over freehand surgery, avoids static guide drawbacks, and enhances the patient experience throughout by increasing restorative outcome confidence.
Technologically Augmented Workflow
As digital technology increasingly impacts dentistry,2 robotic guidance during the surgical procedure delivers repeatable surgical precision, moving the practice closer to a truly digital workflow. The process begins with procedural mapping: restorative-driven imaging that illuminates tooth orientation, bone and soft tissue structure and volume, and nerve positions.
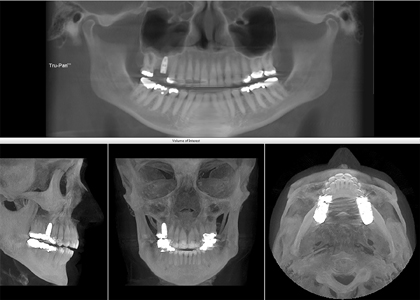
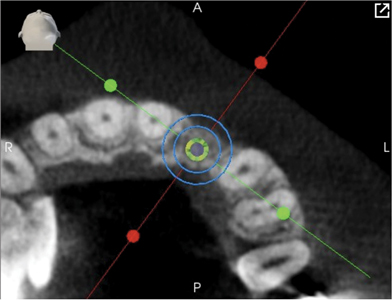
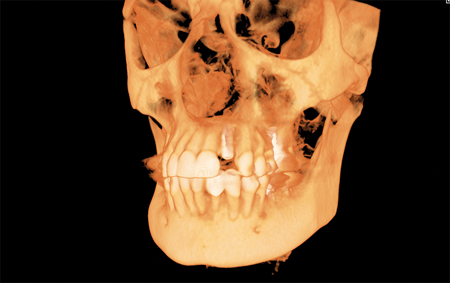
The Yomi process involves a fiducial array, a 3-dimensional orientation target that is splint-affixed to the patient in the preoperative scan (Figs. 1-3). These images, relating the patient relative to the robotic system, are processed with planning software to create a 360-degree view of the oral structures, and to develop a “map” for surgery (Fig. 4). Linking this map with Yomi robotic guidance increases implant accuracy and restorative predictability.
Fig. 1

Fig. 2

Fig. 3

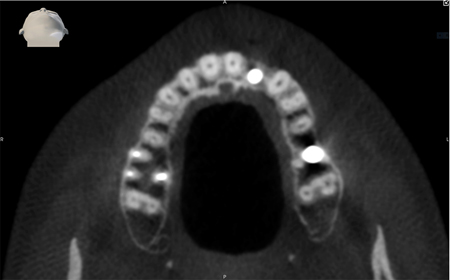
Fig. 4

Note thick sinus membrane indicative of inflammation and 5 mm x 10 mm implant planned within sinus cortical plate.
The Yomi robotic arm manages the handpiece and responds to the surgeon’s hand movements throughout the procedure, providing physical feedback (haptic boundaries) based on drill location with respect to the surgical plan.3-6 These haptic boundaries prevent deviations from the surgical plan. Surgical guides may block visual access to the operative site while navigation requires following visual cues on a monitor. Haptic guidance, on the other hand, allows continuous direct visualization of the surgical site throughout the procedure (Fig. 6). The Yomi robotic platform also provides visual and audio confirmations, enabling assistants to closely follow the workflow and anticipate the next steps. If the practitioner wishes to consult the monitor, robotic haptics stabilize the handpiece improving efficiency and ergonomics (Fig. 7). Yomi’s patient-tracking always tracks the fiducial on the affixed splint to precisely locate the patient relative to the robotic arm (Fig. 5). While Yomi guides the entire surgical process, it does not control it: the plan may be updated for reasons dictated by clinical circumstances at any time. This dynamic control of the procedure (impossible with a static guide) empowers surgeons and encourages responsive patient care.
Fig. 5

Fig. 6

Fig. 7

The following cases illustrate the value of robotic haptic guidance extending the surgeon’s expertise where precise implant placement was critical:
Case Report #1
A female patient presented with an abscess at the root of tooth #16. The tooth was extracted, the site grafted, covered with a membrane, and allowed to heal for several months. At implant surgery, a tooth-borne splint was placed on the anterior dentition, remote to the site of surgery. A fiducial array was attached to the splint and imaged by CBCT scan (iCat, KaVo) (Fig. 3). The resulting DICOM indicated minimal available bone height for implant support due to sinus proximity. The thickened sinus lining exhibited signs of inflammation within the sinus (Fig. 4). The plan was to utilize the maximum available height for implant placement, without intruding into the sinus, yet engaging the floor of the sinus for additional primary stability.7 Precision implant placement planned on Yomi software, and surgically guided by the robotic arm, allowed the achievement of these goals.
A 5mm x 10mm implant was carefully positioned within the sinus cortical plate utilizing the planning software. Robotic guidance allowed the surgeon to proceed with a flapless technique under local anesthetic. Following a landmark check to verify that Yomi had properly located the patient 3-dimensionally, the surgeon performed Yomi-guided osteotomies utilizing the manufacturer’s soft bone protocol (Figs. 5-8). The implant was then placed with robotic guidance (Fig. 9), assuring secure depth control. A healing collar was placed on the implant (Fig. 10) and the splint was removed along the seam (Fig. 11). The patient reported no discomfort during the procedure, likely because guidance enabled a minimally invasive approach. Post-operative imaging revealed the implant placed precisely, as planned, at the sinus floor, avoiding intrusion into the sinus while maximizing primary stability (Fig. 12).
Fig. 8

Fig. 9

Fig. 10

Fig. 11

Fig. 12
Case Report #2
Implant positioning for tooth #22 is extremely challenging due to space limitations and the need for very precise angulation to develop an aesthetically acceptable emergence profile.8 The patient’s tooth #22 had failed endodontics and cystic degeneration following apicoectomy.
The tooth was extracted, and the site grafted anticipating implant placement. Following Invisalign treatment to optimize occlusion and aesthetics, implant placement space was created. For comprehensive smile design, both the mesial-distal positioning and the implant angulation were critical. Additionally, correct implant depth was required for ideal emergence. Depth control was also crucial to engaging the nasal floor (cortex) for added primary stability. Yomi treatment planning software virtually positioned the implant for ideal angulation and optimal bone presence for osseointegration pre-surgery (Figs. 13A,B,C,D).
Fig. 13A

Fig. 13B

Fig. 13C

Fig. 13D
Robotic guidance then executed the plan with minimal invasiveness and great visibility. Yomi-guided surgery proceeded under local anesthetic with osteotomies and dental implant placement, at the planned location, angulation, and depth. The implant was covered with a healing screw. Post-operative CBCT revealed the implant placed to plan within the necessary bony margins (Figs. 14A,B,C,D).
Fig. 14A
A. 3D image.
Fig. 14B

Fig. 14C
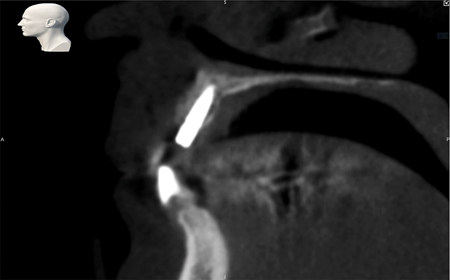
Fig. 14D
Discussion
The Yomi robotic guidance platform offers a digital workflow for providing reliable, predictable dental implants with minimal recovery time. Robotic surgical guidance makes full use of detailed patient-specific virtual plans which can be created and/or modified by the practitioner as required. Treatment comfort and confidence increase patient satisfaction. The robotic guidance platform provides increased surgical speed and accuracy, while centered on human surgical judgement, serves as an extension and enhancement of clinical expertise.
Oral Health welcomes this original article.
Disclosures: The author received no specific funding for this work.
References
- Orentlicher G, Horowitz A, Goldsmith D, Delgado-Ruiz R, Abboud M. Cumulative survival rate of implants placed “fully guided” using CT-guided surgery: A 7-year retrospective study. Compend Contin Educ Dent. 2014 Sep;35(8):590-98, 600.
- Wismeijer D, Joda T, Flügge T, et al. Group 5 ITI Consensus Report: Digital technologies. Clin Oral Implants Res. 2018;29 Suppl 16:436–442. doi:10.1111/clr.13309.
- Grant, BT. Implant surgery with robotic guidance: Digital workflows for patient care. Oral Health. 2019 Jun.
- Rawal S, Tillery D, Brewer P. Robotic-assisted prosthetically driven planning and immediate placement of a dental implant. Comp Cont Educ Dent. 2020 Jan;41(1):26-30.
- Wu Y, Wang F, Fan S, Chow JK. Robotics in dental implantology. Oral Maxillofac Surg Clin North Am. 2019 Aug;31(3):513-518. doi: 10.1016/j.coms.2019.03.013.
- Wu Q, Zhao YM, Bai SZ, Li X. Application of robotics in stomatology. Int J Comput Dent. 2019;22(3):251-260.
- Ragucci GM, Elnayef B, Suárez-López Del Amo F, Wang HL, Hernández-Alfaro F, Gargallo-Albiol J. (2019). Influence of exposing dental implants into the sinus cavity on survival and complications rate: A systematic review. Int J Implant Dent. 2019 Feb;5(1):6. doi:10.1186/s40729-019-0157-7.
- Steigmann M, Monje A, Chan HL, Wang HL. Emergence profile design based on implant position in the esthetic zone. Int J Periodontics Restorative Dent. 2014 Jul-Aug;34(4):559-63. doi: 10.11607/prd.2016.
About the Author
 Ryaz Ansari is a Board Certified Oral and Maxillofacial Surgeon. He is a Fellow of the American Association of Oral and Maxillofacial Surgeons. Dr. Ansari studied dentistry at the University of Western Ontario, completed his Oral and Maxillofacial Surgery Residency at the Brooklyn Hospital Center. He completed a Fellowship in Cosmetic/Maxillofacial surgery at the Missouri Baptist Medical Center. He is currently in private practice in West Hartford, Connecticut. Dr. Ansari can be reached at DocAnsari@JawFixers.com
Ryaz Ansari is a Board Certified Oral and Maxillofacial Surgeon. He is a Fellow of the American Association of Oral and Maxillofacial Surgeons. Dr. Ansari studied dentistry at the University of Western Ontario, completed his Oral and Maxillofacial Surgery Residency at the Brooklyn Hospital Center. He completed a Fellowship in Cosmetic/Maxillofacial surgery at the Missouri Baptist Medical Center. He is currently in private practice in West Hartford, Connecticut. Dr. Ansari can be reached at DocAnsari@JawFixers.com
To see more articles from the July/August 2020 issue, please click here!










