
Introduction
Among the most frequently performed procedures in dentistry are posterior direct composite restorations. Traditionally requiring the incremental placement of composite layers in order to prevent polymerization shrinkage, postoperative sensitivity, and marginal leakage, direct posterior restorations can be difficult and time-consuming treatments. 1-3 Their location in the mouth can oftentimes hinder the precise placement of the requisite multiple layers of composite and, therefore, potentially compromise the durability and functionality of the restorations. 4
For example, it is not uncommon for incrementally placed composite layers to succumb to polymerization shrinkage, which can subsequently result in gaps, voids, and ultimately adhesive bond failure. As bonds between the tooth and restoration fail, postoperative sensitivity and marginal leakage can result. 5,6 Further complicating direct posterior restorations is the variety of composites available today. Some composites may be appropriate only for either anterior or posterior indications, depending upon their composition and esthetic, wear, and strength characteristics, while others may be suitable for universal placement anywhere in the mouth. 7
However, the durability and long-term function associated with posterior direct composite restorations are predicated on a combination of factors. These not only include preparation protocol and composite material placement and curing techniques, but also adhesive material characteristics and protocol, which also can be technique sensitive and time consuming. 8-10 Therefore, in recent years manufacturers have introduced a variety of direct restoratives and adhesive solutions to help eliminate the challenges associated with efficiently placing predictable posterior composite restorations.
Universal Adhesives & Bulk Fill Composites
Among these materials are direct bulk fill composites that can be placed in a single increment or layer of up to 4 mm, then fully cured (i.e., Tetric EvoCeram® Bulk Fill, Tetric EvoFlow® Bulk Fill; Ivoclar Vivadent), as well as single-component, truly universal adhesive systems (e.g., AdheSE Universal; Ivoclar Vivadent) that are indicated for light-cured direct composite restorations, indirect restorations, and all etching techniques (i.e., self-etch, selective enamel-etch, and total-etch).
Because AdheSE Universal demonstrates high bond strengths, it is ideal for use on both dentin and enamel in the posterior, where the impact of strong mastication forces on restorations is a concern. It also provides dentists with an opportunity to save themselves and their patients chair time without sacrificing procedural predictability.
Likewise, the benefits of placing Tetric EvoCeram® Bulk Fill in a single 4 mm increment include the elimination of time-consuming and technique sensitive layering – which is prone to gap and void formation. Simultaneously, better marginal adaptation to preparations can be achieved as a result of the material’s physical properties and handling characteristics. These advantages combine to further reduce polymerization shrinkage stress and prevent microleakage, postoperative sensitivity, and secondary caries.
The following case demonstrates the capabilities of AdheSE Universal and Tetric EvoCeram Bulk Fill for delivering a high-quality direct posterior composite restoration according to a simplified, efficient, and minimally invasive protocol.
Case Presentation
A 17-year-old female presented post-orthodontic treatment. During the examination, which was performed using intraoral cameras (e.g., DexCam) for diagnosis and patient education, occlusal decay on tooth #27 was suspected. The diagnosis was confirmed radiographically, as well as through the use of an adjunctive caries detection system (e.g., CariVu, Dexis), which further facilitated diagnosing the decay (Fig. 1). The decision was made to conservatively and minimally-invasively restore the tooth with a combination of flowable and regular viscosity bulk fill composites (e.g., Tetric EvoFlow® Bulk Fill, Tetric EvoCeram® Bulk Fill). Bulk filled composites have been used successfully and conservatively to achieve esthetic and functional results while simultaneously eliminating time-consuming and tedious protocol. 11
The patient was anesthetized, and a rubber dam was placed with a clamp on tooth #27 (Fig. 2). A tight interface between the band and tooth was established in order to facilitate predictable adaptation of the bulk fill composite to the margins.
The decay was thoroughly removed, after which the preparation design was completed to specifically accommodate the anticipated direct composite restoration. In particular, the preparation shape resembled a “Calla Lily” flower, with soft and flared margins (Fig. 3). This preparation design was in sharp contrast to the outline form advocated by G.V. Black for amalgam restorations. 12 The completed preparation was then particle abraded prior to initiating any adhesive protocols using an air abrasion unit (e.g., PrepStart, Danville) in order to homogenize the dentin, seal the dental tubules, facilitate increased bond strength to dentin, 13 and reduce sensitivity.
Fig. 1
Preoperative CariVu image of tooth #27 revealing occlusal decay.

Fig. 2
Preoperative view of tooth #27 with rubber dam in place.

Fig. 3
The preparation was completed with soft and flared margins.

The preparation was etched using a total etch technique. A 37% phosphoric acid was first applied to the enamel for 15 seconds, and then to the dentin for 10 seconds (Fig. 4). The preparation was rinsed and air dried. Prior to adhesive placement, a re-wetting agent (e.g., G-5, Clinician’s Choice) was applied.
A universal adhesive (e.g., AdheSE Universal) was applied to the preparation by vigorous rubbing, first onto the dentin using the application tip (Fig. 5), then onto the enamel. The adhesive was allowed to set for 20 seconds, after which it was dispersed with air and light-cured for 10 seconds.
Then, to line the preparation and block any potential dark underlying tooth structure, an increment of flowable bulk fill composite in shade IVA (e.g., Tetric EvoFlow Bulk Fill) was placed into the preparation (Fig. 6). Because this flowable bulk fill composite could be placed in increments of up to 4 mm without concerns about shrinkage stresses or incomplete curing, it was ideal for use in even the deepest preparations. The material’s self-adapting and assencio technology would contribute to a void-free restoration. This flowable increment was light cured for 10 seconds using an LED curing light (e.g., Bluephase, Ivoclar Vivadent), after which the composite demonstrated a dentin-like opacity.
Fig. 4
A total etch technique using 37% phosphoric acid was performed to condition the enamel and dentin.

Fig. 5
The AdheSE Universal bonding agent was applied to the dentin.

Fig. 6
An increment of Tetric EvoFlow Bulk Fill composite in shade IVA was placed to line the preparation.

To complete the restoration, a single increment of the bulk fill composite (e.g., Tetric EvoCeram® Bulk Fill) in shade IVA was injected directly into the cavity preparation (Fig. 7). A modeling instrument (e.g., OptraSculpt, Ivoclar Vivadent) was then used to easily sculpt, shape, and contour the composite into place, as well as create the proper anatomy (Fig. 8). Using this modeling instrument was key to establishing proper anatomy and contouring the cuspal inclines, which ultimately reduced the amount of high-speed hand-piece, post-curing contouring and finishing that would be required. The bulk increment was then light cured for 10 seconds from each aspect. Prior to finishing, a layer of glycerin (e.g., DeOx, Ultradent) was applied over the restoration and light polymerized. This step is taken to polymerize the oxygen inhibited layer of the composite.
Fig. 7
A single increment of Tetric EvoCeram® Bulk Fill composite in shade IVA was injected directly into the cavity preparation to complete the restoration.
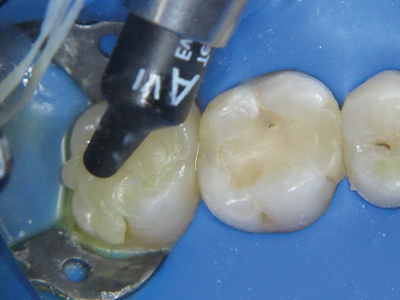
Fig. 8
An OptraSculpt modeling instrument was used to easily sculpt, shape, and contour the composite into place and create the proper anatomy.

The restorations were finished (Fig. 9), the patient’s occlusion was checked, and any adjustments made (Fig. 10). The rubber dam and clamp were removed, and a final polish was performed using an advanced polishing system consisting of a series of grey, green, and pink polishing points (Astropol, Ivoclar Vivadent) (Fig. 11).
Fig. 9
The amount of high-speed finishing required was greatly reduced by properly contouring the easy-to-handle and manage bulk fill composite.

Fig. 10
The patient’s occlusion was checked, after which any adjustments made.

Fig. 11
The Astropol advanced polishing system was used to impart the restorations with a final polish.

Fig. 12
Postoperative view of the completed direct posterior bulk fill composite restoration on tooth #27.

Conclusion
The availability of bulk fill composites such as Tetric EvoCeram® Bulk Fill, combined with the versatility of AdheSE Universal adhesive bonding system, can enable dentists to eliminate the complicated protocol traditionally associated with providing direct posterior composite restorations. In this case, the ability to bulk fill the composite in one increment was key to an efficient process for delivery an esthetic result (Fig. 12). By shortening the length of the procedure, Tetric EvoCeram® Bulk Fill and AdheSE Universal contribute to the efficient and cost-effective delivery of predictable and esthetic restorations. OH
Oral Health welcomes this original article.
References
- Sarrett DC. Clinical challenges and the relevance of materials testing for posterior composite restorations. Dent Mater. 2005;21(1):9-20.
- Giachetti L, Scaminaci Russo D, Bambi C, Grandini R. A review of polymerization shrinkage stress: current techniques for posterior direct resin restorations. J Contemp Dent Pract. 2006;7(4):79-88.
- Christensen GJ. Remaining challenges with class II resin-based composite restorations. J Am Dent Assoc. 2007;138(11):1487-9.
- Mackenzie L, Shortall AC, Burke FJ. Direct posterior composites: a practical guide. Dent Update. 2009;36(2):71-2, 74-6, 89-80 passim.
- Opdam NJ, Bronkhorst EM, Roeters JM, Loomans BA. Longevity and reasons for failure of sandwich and total etch posterior composite resin restorations. J Adhes Dent. 2007;9(5):469-75.
- Rodrigues Junior SA, Pin LF, Machado G, Della Bona A, Demarco FF. Influence of different restorative techniques on marginal seal of class II composite restorations. J Appl Oral Sci. 2010;18(1):37-43.
- Ferracane JL. Resin composite—state of the art. Dent Mater. 2011 Jan;27(1):29-38. Epub 2010 Nov 18.
- Campodonico CE, Tantbirojn D, Olin PS, Versluis A. Cuspal deflection and depth of cure in resin-based composite restorations filled by using bulk, incremental and transtooth-illumination techniques. J Am Dent Assoc. 2011 Oct;142(10):1176-82.
- Souza-Junior EJ, de Souza-Régis MR, Alonso RC, de Freitas AP, Sinhoreti MA, Cunha LG. Effect of the curing method and composite volume on marginal and internal adaptation of composite restoratives. Oper Dent. 2011 Mar-Apr;36(2):231-8. Epub 2011 Jun 24.
- Van Ende A, De Munck J, Van Landuyt KL, et al. Bulk-filling of high C-factor posterior cavities: effect on adhesion to cavity-bottom dentin. Dent Mater. 2013 ;29(3):269-277.
- Margeas RC. Bulk-fill materials: simplify restorations, reduce chairtime. Compend Contin Educ Dent. 2015 Jan;36(1):e1-4.
- Osborne JW, Summitt JB. Extension for prevention: is it relevant today? Am J Dent. 1998 Aug;11(4):189-96.
- Chaiyabutr Y, Kois JC. The effect of tooth-preparation cleansing protocol on the bond strength of self-adhesive resin cement to dentin contaminated with a hemostatic agent. Oper Dent. 2011 Jan-Feb;36(1):18-26. doi: 10.2341/09-308-LR1. Epub 2011 Feb 21.
About the Author
 Dr. Marangos is a graduate of the University of Toronto, Faculty of Dentistry, 1986. He completed a General Practice Residency at Mount Sinai Hospital in Toronto in 1987. He maintains a private practice in Toronto with emphasis on aesthetic and restorative dentistry and orthodontics. Dr. Marangos has lectured for many groups and study clubs on restorative dentistry, orthodontics and the management of TMD and craniofacial pain, direct and indirect restorative dentistry, Biometrics, Occlusion, Predictable Aesthetic Dentistry as well as teaching hands-on programs in Adhesive dentistry and the placement of direct anterior and posterior composite restorations. In 2012-2017 he was awarded the distinction of being “A Leader in C.E.” by the publication Dentistry Today. He is the principal doctor at the Yorkville TMJ Centre, a practice that focuses on the management of head, neck and TMJ related pain as well as treating patients diagnosed with sleep disordered breathing. Dr. Marangos can be reached at 416-465-9343, 416-465-9310 (fax) or by email at dmarangos@rogers.com.
Dr. Marangos is a graduate of the University of Toronto, Faculty of Dentistry, 1986. He completed a General Practice Residency at Mount Sinai Hospital in Toronto in 1987. He maintains a private practice in Toronto with emphasis on aesthetic and restorative dentistry and orthodontics. Dr. Marangos has lectured for many groups and study clubs on restorative dentistry, orthodontics and the management of TMD and craniofacial pain, direct and indirect restorative dentistry, Biometrics, Occlusion, Predictable Aesthetic Dentistry as well as teaching hands-on programs in Adhesive dentistry and the placement of direct anterior and posterior composite restorations. In 2012-2017 he was awarded the distinction of being “A Leader in C.E.” by the publication Dentistry Today. He is the principal doctor at the Yorkville TMJ Centre, a practice that focuses on the management of head, neck and TMJ related pain as well as treating patients diagnosed with sleep disordered breathing. Dr. Marangos can be reached at 416-465-9343, 416-465-9310 (fax) or by email at dmarangos@rogers.com.
Follow the Oral Health Group on Facebook, Instagram, Twitter and LinkedIn for the latest updates on news, clinical articles, practice management and more!










