
The Past
When it became possible to bond tooth colored restorative materials to enamel in the early 1980’s, dental practice, as we know it was changed forever. The “Age of Aesthetic Dentistry” was born. No longer did the dentist deal with only dental disease (caries and periodontal), but now could offer solutions for aesthetic dental problems that were never before possible. Around the same time, tooth whitening, or “bleaching” was also discovered to be a conservative way to help “aesthetically enhance” the color of a people’s teeth. There were early struggles within the profession to accept these “aesthetic or cosmetic” treatments as “real dentistry”, but eventually these procedures became a part of the majority of general dental practices. In the 1990’s, postgraduate “institutes” or “learning centers” were formed to help train dentists in the latest aesthetic procedures and to convert their general practices to “elective aesthetic (cosmetic) dental centers”. Soon, many dental practices were promoted as “aesthetic or cosmetic” losing focus on the “general” dental services they provided. These types of offices flourished for several years…till around 2007, when the worldwide economic downturn began to affect many businesses, including dentistry. As the discretionary incomes of many disappeared, so did the demand for elective dental services. Many dentists who followed the advice of the “gurus”, limiting their practices to aesthetic (cosmetic) services found their “bottom lines” suffering and as a result, reverted back to building their “general services”, which even during the “downturn” were services that patients continued to need.
The Present
Fast forward to 2017…..while according to some “experts”, economic recovery has occurred in the business of dentistry, it does not appear that it has been “across the board”. Many offices have had to scale back fees on elective services to make them more affordable in today’s economy. Also, fee for service practices have to compete with corporate dental entities that tend to have greatly reduced fee structures. “Bread and butter” general dentistry is still what keeps the profession moving forward. Does this mean that the “Age of Elective Aesthetic Dentistry” is now behind us? Many do not believe so, although the “game” is surely changing. One possible strategy for the aesthetically oriented general dental practices moving forward is to offer a “tiered level” of aesthetic services at different price points to allow those patients interested in aesthetic dentistry to opportunity to afford elective service.
This article will discuss some of the many aesthetic dental services that can provide a beautiful result that patients will appreciate: 1) Tooth Whitening, 2) Invisalign and Six Months Smile (Short Term Orthodontics) 3) Direct Composite Restorations (Single Tooth and Bridges), and 4) Indirect Composite Veneers (Prefabricated and Laboratory Fabricated) and 5) All Ceramic Veneers, Crowns, and Bridges. It is important to remember that acceptance of aesthetic procedures is very subjective, both to the patient and dentist. Some in our profession will accept only the highest level of dental artistry, but it is important to remember whom it is we are trying to satisfy. If the patient cannot discern the aesthetic difference between “a Chevy” and “a Rolls Royce”, does everyone really need a Rolls Royce?
Tooth Whitening
Tooth whitening, or “bleaching” continues to be a very popular, low cost conservative solution to for patients to improve the aesthetics of their smile. As we age, are teeth tend to darken in shade (lower in value) as the thickness of the enamel layer decreases due to wear and attrition, while the dentin desiccates and deepens in color. Whitening agents, either hydrogen peroxide or carbamide peroxide both work based on concentration and time in contact with the teeth. While the argument continues as to which produces better results – “over the counter” whitening agents or professionally dispensed “at home” or “in office” treatments, the fact is that tooth whitening is unpredictable and is extremely variable in the results that are obtained. That being said, because of the economical price point and conservative nature of the treatment, it remains a popular choice by many patients (Fig. 1).
Figure 1
In office whitening is shown being performed after isolating the gingival tissues with a liquid dam to protect from the use of more concentrated hydrogen peroxide solutions.

Six Month Smiles (Short Term Orthodontics), Essix MTM (Minor Tooth Movement) Aligners, and Invisalign
Today more than ever, some type of tooth movement (orthodontic) is being done in the general dental practice to cosmetically and/or functionally correct the positions of patients’ teeth. This service is provided both as stand-alone treatment and also in conjunction with tooth whitening and/or prosthetic services. Six Month Smiles is designed to be a short-term cosmetic treatment to correct alignment, crowding, and rotations of teeth (Fig. 2). It is not meant to be a full orthodontic correction that will change Angle’s Classification or make major occlusal corrections. Of course, the patient needs to be aware of this before beginning treatment. Essix aligners for minor tooth movement have been used for many years to correct up to four anterior teeth with crowding and rotations up to 4 mm. Invisalign orthodontics can be utilized for minor tooth movement (Invisalign Express), cosmetic realignment similar to six-month smiles when fixed appliances are not desired by the patient, and for full orthodontic cases as well (Fig. 3).
Figure 2
A patient is shown after fixed orthodontic appliances (Six Month Smiles) have been placed to correct generalized minor rotation and crowding by expanding the arches to accommodate the mesio-distal widths of the teeth.

Figure 3
A patient is shown mid treatment wearing Invisalign clear aligners for a full orthodontic correction of an anterior open bite.

Creative Uses For Direct Composite Resin To Restore Aesthetic Problems
Advances in materials science have allowed for direct composite to be used for restorative solutions that in the past typically required indirect solutions for optimal biologic, aesthetic, and functional results. Diastema closures and filling of “Black Triangles” (excessive gingival embrasures) have been done with composite resin for years, but not with the precision of indirectly fabricated ceramic restorations…until now! Replacing single missing teeth with a direct composite bridge is not typically in most dentists “restorative repertoire”. Direct composite veneers can be difficult and time consuming to master and place for even the most experienced operator. A unique template system is now available that “levels the playing field” for everyone. These new breakthroughs offer clinical results that are beautifully aesthetic and more economically affordable in many cases, for these deceptively difficult direct restorative solutions.
Bioclear matrices for diastemas closure and “black triangle” restorations have revolutionized direct composite restoration if these difficult clinical areas. The direct restoration using composite has been traditionally difficult in anterior proximal Class III areas because of limited access, large instrumentation, the need to layer composite during placement, and flat matrices (mylar strips) used in conjunction with non anatomic wedges to seal them gingivally. Bioclear matrices are convex in shape, are positioned intimately against the tooth/root surface and held in place with heavy gauge rubber dam, so wedging in not needed to build the sub contact proximal areas between teeth. A convex emergence profile to the restoration is developed by “injection molding” using flowable and heated composites that are injected behind the matrix then light cured. No finishing or polishing is required in the interproximal area, so instrumentation is not an issue (Figs. 4-8).
Figure 4
A preoperative smile view of a patient with a diastema between the mandibular central incisors. Note the small space (less than 3 millimeters) would be very difficult to restore with flat Mylar strip matrices and direct composite. Also, finishing to proper emergence profile in the tight interproximal space, even with the smallest rotary instrument or polishing disc would be next to impossible.

Figure 5
Bioclear matrices are in place held intimately to the proximal tooth surface by the rubber dam. The emergence angles can be clearly seen to be physiologic in contour.

Figure 6
One side of the diastema closure is seen after “injection molding” with heated composite resin. Once light cured, the proximal area of the restorative material should not be touched! The finish from the Mylar is smoother than any polishing instrument could achieve and the emergence profiles of the composite will never be better than at matric removal. Any finishing and polishing will be performed as needed on facial and lingual surfaces to blend the restorative material into the natural tooth surface.
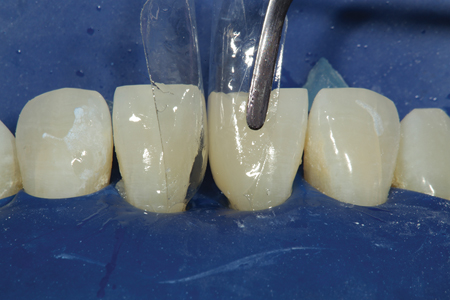
Figure 7
A smile view of the completed diastema closure.

Figure 8
A preoperative view of a patient missing a mandibular right central incisor after completing orthodontic treatment. The patient is 16 years old and not a
candidate for grafting and implant placement at this time.

A common problem faced by restorative dentists is how to handle post orthodontic patients with congenitally missing teeth. Lite cured composite bridges with fiber reinforcement offer these patients an excellent intermediate or long-term solution in one patient visit with no additional laboratory cost. There is a unique fiber reinforcement (everStick C&B: GC America) material that is made up of a bundle of fibers surrounded by a matrix of polymethyl methacrylate (PMMA) and bis-GMA, which allows it to bond directly to composite or acrylic restorative materials, unlike other fiber reinforcement materials currently available. Using this type of fiber material, either as an intracoronal or extracoronal splint (retainer), a direct composite pontic can be sculpted directly to it, closing the space and replacing the missing tooth. Not only can this be a beautifully aesthetic restoration made with little or no preparation (depending on the occlusal relationship of the patient), but also this type of restoration is economical to place and is easily repaired should it fracture at any time during occlusal stress. “Maryland” type bridges made of ceramic materials do not offer either of these advantages and must be remade if they fracture incurring more chair time and additional costs (Figs. 9-12).
Figure 9
Fiber reinforcement is being placed on the lingual aspect to support the pontic and act as an orthodontic retainer as well.

Figure 10
After placement of the “dentin portion” of the pontic on the facial and lingual aspects of the bonded fiber, a course diamond is used to shape and create a roughened surface for addition of the “enamel” increment of composite.

Figure 11
A retracted facial view of the completed direct composite fiber reinforced bridge replacing tooth number 25. When this patient is older, an implant can be
considered if so desired.

Figure 12
A preoperative retracted facial view of a patient that presents with a fractured porcelain restoration on tooth number 8. Both tooth numbers 8 and 9 also have gingival recession with root surface exposure. The patient is getting married in two weeks and needs an immediate “fix” for his aesthetic and functional dilemma.

The Uveneer System (Ultradent Products) is a reusable, anterior labial (facial) surface template kit that provides the dentist with preformed anatomic surfaces for simplified and expedient composite placement and finishing. The system was designed to create direct composite veneers with predictable shape and symmetry quickly and easily. There are many clinical applications for Uveneer templates that extend beyond the typical placement of composite veneers that make this product very useful to the restorative dentist. Uveneer templates come in two sizes to better fit the facial profiles of most teeth. The sizes of the templates are made to match ideal 75-80% width-to-length ratios and to correspond to smile design aesthetic proportions (“golden proportion”). With the nuances of facial proximal line angles, proper heights of contour and facial outline form in the template, Uveneer templates provide a fast, predictable way to create anatomically beautiful direct composite veneers in a fraction of the time when compared to traditional freehand sculpting and contouring. For cases where the templates are not as perfect of a fit, minor contouring and polishing may be required, but the time savings in placement is significant because of the preformed facial anatomy. Uveneer templates are constructed from a non-stick tempered plastic so they are autoclavable and reusable. Any type of composite can be used with the Uveneer system and the dentist can use a single or multiple layer technique depending upon the desired outcome (Figs. 13-15).
Figure 13
After preparing into the ceramic to make space, composite will be bonded to the ceramic using a Uveneer template to recreate the facial anatomy, proximal facial line angles, and incisal embrasures of the restoration in one step.

Figure 14
A postoperative smile view of the patient shown in Figure 13. Some white composite tint was placed at the incisal edge on the dentin layer prior to placement of the enamel increment to better match the patients’ natural surrounding teeth.

Figure 15
A preoperative smile view of a female teenage patient that has aesthetic and functional issues with tooth numbers 7 to 10. She is not financially able to afford ceramic veneers and the minimal amount of overjet and functional concerns could limit the longevity of traditional composite bonding.

Indirect Composite Veneers
Prefabricated composite veneers offer yet another aesthetic option for patients. These veneers come fabricated in three different sizes and are luted to place with nano microhybrid composite and adhesive bonding technique. Since the sizes of the veneers are not exact, the nano microhybrid composite may make up a portion of the finished surface of the restoration. And, because both the luting medium and veneer are made out of the same material, when light cured both surfaces are finished and polished leaving a seamless transition. Figures 16 and 17 show a case in which tooth numbers 7 through 10 were treated with prefabricated indirect composite veneers. As far as economics are concerned, these restorations are placed in one patient visit and the cost per tooth of materials is about one half of the most economical laboratory processed veneer. They also share the same physical properties and surface luster as their laboratory fabricated counterparts since because of 100% conversion of monomer to polymer chains during processing.
Figure 16
A postoperative view after placement of prefabricated composite veneers to correct her problem. This photograph was taken at 5 years post placement.

Figure 17
A preoperative smile view of a patient that had been going through aligner treatment, but decided to have indirect veneers done because she was unhappy with the shape and color of her teeth. One advantage of indirect laboratory fabricated composite veneers is that in many cases they require less tooth reduction and a huge plus is that they are easily repairable with direct composite resin.

Indirect Laboratory Processed Composite Veneers, or “Pearlfect Smile” (Mizrachi Dental Laboratory: Reynoldsburg, OH) is one of dentistry’s “best kept secrets”. Indirect composite restorations are processed in a nitrogen environment under heat and pressure resulting in 100% conversion of monomer to polymer chains, as opposed to direct composite, which converts up to only 70% with light curing alone. The result is a stronger, more highly polished restoration than it direct counterpart. “Pearlfect Smile” veneers also require two patient visits to complete the procedure and are cemented using total etch bonding technique and resin cements (Figs. 18 & 19).
Figure 18
A postoperative view of the patient’s smile after being restored with laboratory fabricated composite veneers. Notice the lifelike texture and finish in the composite that rivals the best ceramic!

Figure 19
A preoperative view of a patient that is in need of a functional and aesthetic dental rehabilitation. His chronological age is 53 years old. His teeth have the color and wear typically seen on a person in their seventies.

All Ceramic Veneers and Crowns
Porcelain laminate veneers have represented the most “popular” elective aesthetic option for patients who desire not only a change in color, but also in the position of their teeth (when orthodontics is not an option for the patient). Full coverage all ceramic restorations can also transform old, worn teeth back to a very youthful appearance, both for aesthetic and functional purposes. These restorations represent the most costly option for the patient because of the chair time involved and laboratory costs, which for some “high end” ceramists can exceed several hundred dollars per tooth. Lithuim disilicate and zirconia can offer a stronger and sometimes, less costly alternative to traditional feldspathic materials because of milling versus hand stacking. Partial coverage porcelain restorations (veneers) require two patient visits to place and are bond utilizing resin cement technologies. High strength full coverage ceramics can in many cases be cemented with traditional cements such as calcium aluminate (Ceramir Crown and Bridge: Doxa Dental) and resin modified glass ionomers (Figs. 20-22).
Figure 20
A five-year postoperative view of the aesthetic reconstruction of the patient shown in Figure 19. Not only has the patient taken years of the patient’s appearance, but also he has preserved his remaining tooth structure for years to come.

Figure 21
A preoperative retracted view of a Class III malocclusion prior to orthognathic surgery to reposition the maxilla and prosthetic reconstruction.

Figure 22
A one-year postoperative view of the patient shown in Figure 21. This case took over two years to complete and the result was an aesthetic Class I correction without orthodontics and mandibular resection. Aesthetic rehabilitations of this kind are ‘life changing” for a patient.

Conclusion
Several different elective aesthetic options have been shown that offer patients the ability to “upgrade” their smile. By setting proper patient expectations, these services and different price points can offer the patient a dental aesthetic alternatives that are economically and aesthetically fit their needs. OH
Oral Health welcomes this original article.
 Dr. Robert A. Lowe graduated magna cum laude from Loyola University School of Dentistry in 1982 and was a Clinical Professor in Restorative Dentistry until its closure in 1993. He maintains a private practice in Charlotte, North Carolina, lectures internationally, and publishes on aesthetic and restorative dentistry. Dr. Lowe is a member of Catapult Elite Speakers Bureau and has Fellowships in the AGD, ICD, ADI, ACD, IADFE, and ASDA. In 2004, he received the Gordon Christensen Outstanding Lecturers Award, and in 2005, Diplomat status on the American Board of Esthetic Dentistry. Dr. Lowe can be reached at 704-450-3321 or at boblowedds@aol.com.
Dr. Robert A. Lowe graduated magna cum laude from Loyola University School of Dentistry in 1982 and was a Clinical Professor in Restorative Dentistry until its closure in 1993. He maintains a private practice in Charlotte, North Carolina, lectures internationally, and publishes on aesthetic and restorative dentistry. Dr. Lowe is a member of Catapult Elite Speakers Bureau and has Fellowships in the AGD, ICD, ADI, ACD, IADFE, and ASDA. In 2004, he received the Gordon Christensen Outstanding Lecturers Award, and in 2005, Diplomat status on the American Board of Esthetic Dentistry. Dr. Lowe can be reached at 704-450-3321 or at boblowedds@aol.com.
RELATED ARTICLE: Quality Aesthetics in the Digital Age
Follow the Oral Health Group on Facebook, Instagram, Twitter and LinkedIn for the latest updates on news, clinical articles, practice management and more!










