
Introduction
The COVID-19 pandemic has made people more conscious about their overall health. It is a good moment to discuss tobacco smoking cessation with our patients. Tobacco smoking has overall devastating effects on health. It continues to be the number one cause of preventable disease and death in Canada. An estimated 45,000 Canadians die each year as a result of smoking and countless others live with chronic diseases.1 It is associated with several forms of lung disease and cancer. Also, various chemicals in tobacco products enhance the development of atherosclerosis, leading to strokes and heart attacks. One of tobacco’s chemicals, nicotine, acts directly on the brain, causing addiction and cognitive decline. Smokers have a 50% chance of dying from a smoking-related complication and will live on average 10 fewer years. Also, tobacco is associated with many oral pathologies including oral and pharyngeal cancers, periodontitis, tooth decay, mouth sores or leukoplakia.2
In Canada, despite public health education and prevention efforts, it is estimated that approximately 15% of Canadians currently smoke. Also, an estimate 64.4% of smokers’ report that they want to quit, and half have tried to quit in the past year.3 Tobacco dependence is a chronic disease that requires repeated and multiple attempts to quit.4 However, effective treatments exist that can significantly increase rates of long-term abstinence. It is essential that clinicians and healthcare delivery systems consistently identify and document tobacco-use status and treat every tobacco user seen in a healthcare setting. Clinicians should encourage every patient willing to make a quit attempt to use counseling treatments and medications. Healthcare providers can be influential in motivating attempts at smoking cessation.4 The goal of this article is to briefly review Nicotine Replacement Therapy (NRT) available to assist patients in their tobacco cessation attempt.
Identifying smokers
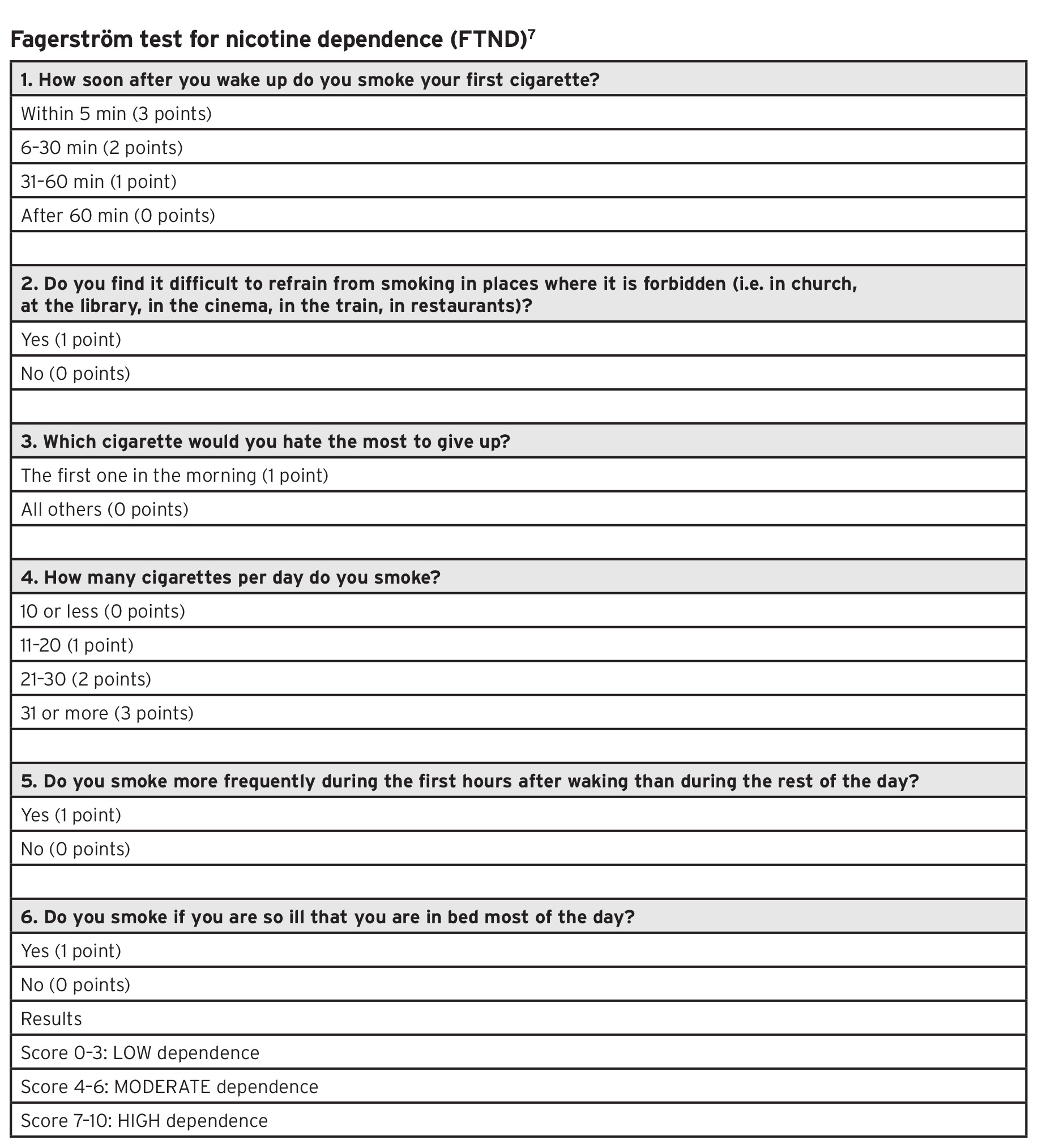
The first step in treating tobacco use and dependence is to identify tobacco users. It is estimated that one-third of smokers will see their dentist yearly. Therefore, dentists are in position to identify and counsel tobacco users.5 Once smokers are identified, their willingness to quit should be determined. Studies have shown that even if a patient is unwilling to quit, there is benefit to brief motivational intervention in increasing future quitting attempts. (Table 1)6 A patient’s degree of addiction can be quantified through screening tools, such as the Fagerström Test for Nicotine Dependence (FTND). (Table 2)7 The scores obtained from these tests can predict the likelihood of relapse after stopping and guide the clinician in selecting the most beneficial therapeutic strategy to help the patient. These questions can be asked by the front desk or simply added to the health questionnaire.
Table 1

Table 2
Pharmacological Approach: Nicotine Replacement Therapy (NRT)
Nicotine replacement therapy relies on the controlled administration of nicotine, making it easier to abstain from tobacco by partially replacing the nicotine previously obtained from tobacco use. The goal is to stimulate nicotine receptors thus removing smoking craving and withdrawal symptoms and to reduce the number of nicotine receptors.
Controlled administration of nicotine reduces the positive effects induced by smoking. Nicotine is more slowly absorbed generating lower but prolonged blood peaks, compared to cigarettes, therefore reducing rewarding effects and withdrawal symptoms.12 Each different NRT product has demonstrated the same efficacy in achieving smoking cessation. Thus, the patient’s preferences should guide the choice of the NRT product.9
Evidence from clinical trials and consensus among experts support the combination of a long-acting patch with a short-acting form such as gum, lozenge, or inhaler.9,12 In a meta-analysis, use of a nicotine patch combined with a short-acting NRT product (gum, spray, or inhaler) was more effective than a single type of NRT9 (Table 3). NRT usually lasts 12 weeks. Nonetheless, when treating heavy smokers longer intervals may be realistic.12
Table 3

Nicotine transdermal patch (long acting):
Transdermal nicotine patches deliver nicotine at a relatively balanced rate, so they are the most appropriate route of administration to reduce withdrawal symptoms. Conversely, chewing gum, lozenges, inhalers and nasal sprays reduce symptoms faster than transdermal patches, but they provide poorer base coverage.9,10,12
Oral Formulation: Nicotine Lozenge/ Nicotine Gum/Nicotine Inhaler (short acting):
Oral formulations contain nicotine absorbed by the oral mucosa. The main flaw of this class is the strict dosing scheme needed, sometimes with a fixed short interval of one to two hours. Furthermore, nicotine is absorbed by the oral mucosa only at neutral pH. Thus, the patient should be advised to avoid meals or drinks (except water) during or in the 15 minutes preceding oral nicotine use.9,10,11 Inhalers have the advantage of simulating cigarette usage, preserving the hand-to-mouth action of smoking.12 This option can be offered to patients, who say they miss the action of smoking.
Safety
Long-term NRT is not associated with increased incidence of harm. Longer therapeutic intervals are particularly indicated in patients with psychiatric or other substance use disorders.12
There are no contraindications to nicotine substitutes except evidence of allergy, which is rare for patients using patches and unusual for patients using oral formulations.
Typical adverse events common to all NRT products include gastrointestinal symptoms, dizziness, headache, and local irritation (according to the route of administration). Adverse events due to NRT can be managed by correcting the dosage to reduce symptoms or by changing products.9,10,12
Patients usually interpret some symptoms as adverse events due to treatment, instead of symptoms related to smoking cessation. Some patients who quit smoking show signs and symptoms of depression. These signs and symptoms are not linked to the therapy itself but rather to the presence of a latent depression, unmasked by smoking cessation.12 Patients with a prior history of depression should be followed carefully to avoid a relapse. Patients who are currently experiencing depression should consult their physician for adequate support.
When craving persists, there is no risk of overtreatment with NRTs. On the other hand, in a patient who is not experiencing any desire for smoking, an overdose produces the impression of excessive smoking. These symptoms are transient and disappear quickly after treatment interruption. Thus, it is possible to reintroduce the therapy later at a lower dose.
Conclusion
The dentist is in an ideal position to motivate and counsel patients on tobacco cessation. Smoking reduces the length and quality of life. Smoking cessation strategies should be implemented in every clinical context. Always have a multidisciplinary and team approach to effective counselling. The pharmacological approach to smoking cessation is safe and effective and should be offered to everyone willing to quit smoking. It is never too late to quit smoking and patients should be motivated and supported in their attempts. For those interested in more information about smoking cessation to better advise and guide their patients, they are invited to visit the Ottawa Model for Smoking Cessation website (https://ottawamodel.ottawaheart.ca/).
Oral Health welcomes this original article.
References
- Rehm, J., Baliunas, D., Brochu, S., Fischer, B. et al. (2006). The Costs of Substance Abuse in Canada, 2002. Highlights. Ottawa ON: Canadian Centre on Substance Abuse.
- Zhang Y, He J, He B, Huang R, Li M. Effect of tobacco on periodontal disease and oral cancer. Tob Induc Dis. 2019;17:40. Published 2019 May 9. doi:10.18332/tid/106187
- Reid RD, Pritchard G, Walker K, Aitken D, Mullen KA, Pipe AL. Managing smoking cessation. CMAJ. 2016;188(17-18):E484-E492. doi:10.1503/cmaj.151510
- Aubin HJ, Karila L, Reynaud M. Pharmacotherapy for smoking cessation: present and future. Curr Pharm Des. 2011;17(14):1343-50. doi: 10.2174/138161211796150837. PMID: 21524268.
- Sandhu HS. A practical guide to tobacco cessation in dental offices. J Can Dent Assoc. 2001 Mar;67(3):153-7. PMID: 11315394.
- World Health Organization. Toolkit for delivering the 5A’s and 5R’s brief tobacco interventions in primary care. 2014. https://www.who.int/tobacco/publications/smoking_cessation/9789241506953/en/. Accessed 5 Jun 2020.
- Heatherton TF, Kozlowski LT, Frecker RC, Fagerström KO. The Fagerström test for nicotine dependence: a revision of the Fagerström tolerance questionnaire. Br J Addict. 1991;86(9):1119–1127.
- Livingston EH, Lynm C. Smoking Cessation. JAMA. 2012;308(15):1599. doi:10.1001/jama.2012.4090
- Cahill K, Stevens S, Perera R, Lancaster T. Pharmacological interventions for smoking cessation: an overview and network meta-analysis. Cochrane Database Syst Rev. 2013 May 31;(5):CD009329. doi: 10.1002/14651858.CD009329.pub2. PMID: 23728690.
- Doll R, Peto R, Boreham J, Sutherland I. Mortality in relation to smoking: 50 years’ observations on male British doctors. BMJ. 2004;328(7455):1519.
- Giulietti, F., Filipponi, A., Rosettani, G. et al. Pharmacological Approach to Smoking Cessation: An Updated Review for Daily Clinical Practice. High Blood Press Cardiovasc Prev 27, 349–362 (2020). https://doi.org/10.1007/s40292-020-00396-9
- U.S. Department of Health and Human Services. Smoking Cessation. A report of the surgeon general. In: Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2020. https://www.hhs.gov/sites/default/files/2020-cessation-sgr-full-report.pdf. Accessed 19 June 2020.
About the Author
 Dr. Saleh is a Montreal native where he completed his post-secondary studies. He obtained his doctorate in Dental Medicine at the University of Montreal in 2015. After graduation, he moved to Hearst, a small town in Northern Ontario, to practice rural dentistry. After his work in Hearst, he decide to do short-term contracts in Kuujjuaq in Northern Quebec with Inuit communities, and Moose Factory in Northern Ontario with Cree communities. These contracts opened an opportunity for him to work full-time in Moose Factory for the Weeneebayko General Hospital (WAHA). He is now pursuing a masters degree in Dental Anesthesiology.
Dr. Saleh is a Montreal native where he completed his post-secondary studies. He obtained his doctorate in Dental Medicine at the University of Montreal in 2015. After graduation, he moved to Hearst, a small town in Northern Ontario, to practice rural dentistry. After his work in Hearst, he decide to do short-term contracts in Kuujjuaq in Northern Quebec with Inuit communities, and Moose Factory in Northern Ontario with Cree communities. These contracts opened an opportunity for him to work full-time in Moose Factory for the Weeneebayko General Hospital (WAHA). He is now pursuing a masters degree in Dental Anesthesiology.










