
Introduction
Congenitally missing maxillary lateral incisors present a challenge for both the orthodontic and restorative treating dentists. Often, only two scenarios are discussed: canine substitution or replacing the missing lateral.1 The former is often considered an orthodontic solution while the latter is more restoratively driven. However, there are complexities in these cases that are dependent on the various stages of development which require further deliberation. Dentists are also tasked with devising solutions for untreated or mismanaged cases (revisions) in the adult stage. The goal of this article is to categorize stages and case types while offering some expanded strategies for transitional, definitive and revision treatment options.
Discussion of Stages, Case Types and Treatment Options for Missing Lateral(s)
Adolescent Stage Presentations
Type 1: Early mixed dentition prior to eruption of the permanent canine.
Treatment options:
Interceptive orthodontics to maintain or open space for future lateral incisor replacement. This option will ensure the patient has a full complement of teeth (natural and prosthetic) with the best chance for an idealized occlusion and esthetics. The barrier to case acceptance is navigating the transition period until the young patient is ready for definitive treatment. The most common modalities for long term space maintenance are transitional removable appliances or fixed prostheses, both have their limitations and problems.
The success of this case is dependent on the orthodontist and restorative/implant team working together from the beginning to plan and execute this challenging case type. The eventual replacement of the missing lateral with either a fixed bridge or an implant often requires hard and soft tissue augmentation along with pontic/implant site development. Transitional prostheses will not maintain the alveolar bone so anticipate deficient buccal tissues.2 Also essential for a successful outcome is great lab communication to ensure proper shade selection and pontic/implant site design for esthetic excellence.
Traditional canine substitution with posterior teeth protracted mesially to close all space. This satisfies the desire to replace the missing lateral and provide a definitive treatment at an early age and eliminate the transition period. The key to canine substitution is the ability to transform a canine into a lateral.3 This requires an understanding of anatomy and composite skills. While the occlusion is acceptable it is a compromise as it deviates from ideal norms.
Type 2a: Late mixed dentition with permanent canine erupted into the lateral space and primary canine present.
Treatment options:
Orthodontics including extraction of primary canine and distalization of permanent canine to open space for future lateral replacement. Like early mixed dentition but now the ectopically erupted canine must be translated back to its normal position. Care must be taken to bodily move the tooth so that the crown and root end up in their proper inclination and angulation. If the tooth is tipped distally during orthodontic therapy the root position will hinder future implant placement.
Traditional canine substitution: Extract the primmary canine and proceed as described for Type 1. Non-traditional canine substitution with primary canine maintained in the canine position: The non-traditional canine substitution has advantages both clinically and socially for an adolescent patient. While canine substitution presents significant esthetic challenges as previously discussed, maintaining the primary canine (if indicated by root stability) will provide the patient a full complement of teeth and avoid interim space maintenance. This strategy also avoids orthodontic therapy to protract posterior teeth which at this stage is more difficult. The occlusion is stabilized as the posterior teeth remain in their normal relationships. The alveolar bone and soft tissue are also maintained with the presence of the primary tooth, thereby improving the predictability of future esthetic success. However, in these cases two teeth will need to be modified, in addition to modifying the permanent canine to mimic a lateral, the primary canine will need to be widened to that of the of a permanent canine.4 (Figs. 1-3) This should be coordinated during orthodontic treatment for best results. When the teeth are correctly proportioned the orthodontist now knows exactly where to finish the case and therefor space management is simplified.
Fig. 1
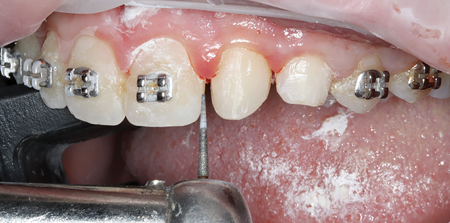
Fig. 2

Fig. 3

Type 2b: Late mixed dentition with permanent canine erupted into the lateral space and primary canine is not present.
Treatment options:
Orthodontics to distalize the permanent canine, then maintain space for future lateral replacement.
Traditional canine substitution.
Non-Traditional Canine substitution while maintaining or opening space for future canine replacement. By not protracting the posterior teeth to fill the space vacated by the canine you must plan for its future replacement. Since the canine is an integral part of occlusal schemes, controversy regarding a natural tooth vs a prosthetic or implant replacement in that position is understandable.5
Type 3a: Late mixed dentition with permanent canine erupted into canine space and primary lateral is present.
Treatment options
Extract primary lateral incisor, then maintain or open space for future lateral replacement.
Extract primary lateral incisor, then traditional canine substitution.
Primary lateral substitution. Re-proportion the primary lateral to mimic permanent lateral. If the primary root is stable this is the ideal way of maintaining the space as well as preserving the alveolar bone and soft tissue for future implant or prosthetic replacement.
Type 3b: Late mixed dentition with permanent canine erupted into canine space and primary lateral is not present.
Treatment options
See Type 1 options. This rarely happens as the canine erupts or migrates mesially without the presence of a primary or permanent lateral.6
Adult Stage Presentations (Treated or Relapsed in need of Revision and Untreated)
Type 4: Untreated Missing lateral(s) and canine and/or central drift with residual space
Treatment options
Orthodontics to open space for lateral replacement. (Figs. 4-8)
Fig. 4

Fig. 5

Fig. 6

Fig. 7

Fig. 8

Restore six or more anterior teeth with orthodontics to re-allocate space. This is the compromise if the patient declines tooth replacement but accepts orthodontic treatment. Re-allocation of the residual space to create restorations with improved proportions.
Restore six or more anterior teeth without orthodontics. A risky option when a patient declines orthodontics or lateral replacement and you attempt to solve the tooth size arch discrepancy with restorations alone. The amount of residual space and the current positions of the anterior teeth could make this option viable, however the esthetic results are usually compromised as the individual and relative proportions of the anterior teeth do not appear natural. (Figs. 9,10)
Fig. 9

Fig. 10

Type 5: Lateral space currently restored with non-satisfactory fixed prosthesis or being maintained with a removable prosthesis
Treatment options
Replace fixed prosthesis. Resin-bonded prostheses (Maryland bridges) are common treatments for one or two missing laterals, often with a history of debonding or compromised esthetics. Correctly diagnosing the cause for failure will direct you to the best treatment plan moving forward. Reasons for repeated debonding are insufficient interocclusal space, compromised enamel for achieving adhesion, poor prosthetic preparation or design, poor material selection for wings or pontic, improper adhesive selection or technique.7 Before replacing also consider one wing instead of two, full coverage retainers, or implant.
Replace transitional removable prosthesis with implants or fixed prosthesis. Evaluate for implant replacement first by assessing hard and soft tissue volume and quality, clinical tooth position and space. (Figs. 11,12) A Radiographic evaluation of root positions is also necessary because clinical appearance alone can be misleading, and canine roots can reapproximate after time.8 (Fig. 13)
Fig. 11

Fig. 12

Fig. 13

Type 6: Unesthetic canine substitution with bicuspid in the canine position.
Treatment options
Idealize the shape and contours of substituted canine and bicuspid. Utilize direct or indirect restorations combined with orthodontics (as indicated) to establish correct tooth positioning and proportions. (Figs. 14-16)
Fig. 14

Fig. 15

Fig. 16

Type 7: Canine substitution with canine space open or prosthetically replaced.
Treatment options
Orthodontics to distalize canine and open lateral space for replacement.
Idealize the shape and contours of substituted canine then restore canine space with implant or prosthesis. These cases often require orthodontics to ideally position teeth and ensure proper spatial proportions. Consider group function on side with implant or pontic in place of canine.
Adult Case Example
The following case demonstrates an adult stage type 7. This 27-year-old female presented for consultation with a desire to improve her smile with veneers prior to her wedding in 10 months. (Figs. 17,18) After comprehensive clinical and radiographic examination the following conditions were noted: Congenitally missing maxillary left lateral incisor (#10) with canine substitution. Peg maxillary left lateral incisor (#7) restored with ceramic veneer. Fractured maxillary left central incisor (#9) and a PFM bridge to replace missing substituted canine (#11).
Fig. 17

Fig. 18

As an adolescent the orthodontic treatment plan apparently was to substitute the canine into the missing lateral space and leave the vacated canine space open for future prosthetic replacement. Treatment was completed but the patient was never happy with the esthetics. It was decided to revise this case with limited orthodontics to reposition the maxillary anterior teeth. Sectioning the bridge and creating properly shaped provisionals would be done prior to bracketing to set up the case for the final restorations. (Figs. 19,20)
Fig. 19

Fig. 20

Once the case was set up orthodontically, the upper right fixed bridge and the porcelain veneer #7 were redone. Fractured tooth #9 was conservatively restored with composite. (Figs. 21-26)
Fig. 21

Fig. 22

Fig. 23

Fig. 24

Fig. 25

Fig. 26

Adolescent Case Example
It is likely the previous adult case example started off very similar to this adolescent stage type 1 case (early mixed dentition prior to eruption of canine). This 9 y/o presented with a congenitally missing maxillary left lateral incisor (#10). The treatment decision was to allow the permanent canine (#11) to erupt and then translate it back into the normal canine position followed by space maintenance until the child was ready for implant or prosthetic placement. (Figs. 27-30)
Fig. 27

Fig. 28

Fig. 29

Fig. 30

Interceptive orthodontic treatment began by placing the patient in an upper and lower Brehm Nitinol Utility Arch (Ortho Arch: Schaumburg, IL,). (Figs. 31,32) This allows for correction of the deep bite, arch development, anterior alignment, and proper inclination. Once the canine is erupted enough to bracket, a D2 Appliance (Ortho Arch: Schaumburg, IL,) was placed to begin translating the canine back into the proper
canine position. (Fig. 33)
Fig. 31

Fig. 32
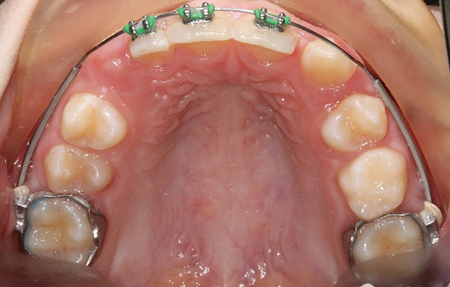
Fig. 33

Phase two conventional fixed orthodontic therapy begins after the canine translation is completed. (Fig. 34) The goal of phase two is to correct any remaining alignment issues, midline discrepancy and finish with a class one occlusion. If you are planning for a resin-bonded bridge, now is the time to create a little excess overjet to decrease the need for lingual tooth preparation.
Fig. 34

Prior to de-band ensure the root angulation of the adjacent teeth are correct and the site is set up for future implant placement. (Fig. 35) Retention with conventional removable retainers is fine but in this case an immediate composite one wing resin bonded bridge was place soon after the orthodontics was completed.9 (Fig. 36) Compared to the previous revision case example; this young patient is set up for success when she is ready for her definitive treatment. (Fig. 37)
Fig. 35

Fig. 36

Fig. 37

Exploring all options that satisfy the patients desires while providing predictable results in a responsible manner should always be our goal. Congenitally missing teeth, especially those in the esthetic zone, present significant challenges. This article further details previous attempts to organize treatment decisions for missing lateral(s) by considering varied presentations at different stages of development. Noticeable missing from this article is discussion of malocclusion types on the treatment decision process, specifically, if the Angle classification favors one treatment over another. That topic has been extensively covered in the literature and is beyond scope of this article.
Oral Health welcomes this original article.
References
- Priest, George. The treatment dilemma of missing maxillary lateral incisors-Part I: Canine substitution and resin-bonded fixed dental prostheses Volume 31, Issue 4 July/August 2019.
- Uribe F, Chau V, Padala S, Neace WP, Cutrera A, Nanda R. Alveolar ridge width and height changes after orthodontic space opening in patients congenitally missing maxillary lateral incisors. Eur J Orthod. 2013 Feb.
- Kokich VO Jr, Kinzer GA. Managing congenitally missing lateral incisors. Part I: Canine substitution. J Esthet Restor Dent. 2005.
- Kiliaridis S, Sidira M, Kirmanidou Y, Michalakis K. Treatment options for congenitally missing lateral incisors. Eur J Oral Implantol. 2016.
- Auroy P, Lecerf J. Prosthetic restoration of the canine. J Dentofacial Anom Orthod. 2010.
- Ngan P, Early Timely Management of Ectopically Erupting Maxillary Canines. Seminars in Orthodontics, Volume 11, Issue 3.
- Creugers NH, Käyser AF. An analysis of multiple failures of resin-bonded bridges. J Dent. 1992 Dec.
- Olsen TM, Kokich VG Sr. Post-orthodontic root approximation after opening space for maxillary lateral incisor implants. Am J
Orthod Dentofacial Orthop. 2010 Feb. - Kern M. Clinical long-term survival of two-retainer and single-retainer all-ceramic resin-bonded fixed partial dentures. Quintessence Int. 2005;36(2):141-147.
About the Author
 Salvatore Lotardo is the owner of Bella Smiles of Long Island, a multi-practice group with a focus on multidisciplinary esthetic dentistry in New York. He is an Accredited Member and Past President of the AACD. He graduated from Stony Brook School of Dental Medicine in 1990. Dr. Lotardo’s passion is mentoring young dentists and he devotes much time lecturing nationally and internationally. He can be contacted at DrL@BellaSmilesNow.com or 631.875.5222
Salvatore Lotardo is the owner of Bella Smiles of Long Island, a multi-practice group with a focus on multidisciplinary esthetic dentistry in New York. He is an Accredited Member and Past President of the AACD. He graduated from Stony Brook School of Dental Medicine in 1990. Dr. Lotardo’s passion is mentoring young dentists and he devotes much time lecturing nationally and internationally. He can be contacted at DrL@BellaSmilesNow.com or 631.875.5222










