

Congenital missing teeth (CMT) or dental agenesis is a common dental abnormality, in which some dental buds fail to develop, leaving an empty space in the arch which causes numerous complications.1 In most countries, out of every 10 to 20 individuals, at least one suffers from agenesis of at least one or two permanent teeth.2,3
CMT can present either as part of a syndrome such as cleft lip and palate, ectodermal dysplasia, Van Der Woude syndrome or Down’s syndrome, or on its own as a non-syndromic condition.3 Although it is a hereditary condition, it has also been found in patients without a family history of CMT. While CMT precise aetiology remains to be determined, it is thought to be caused by environmental or genetic factors.4
Involvement of multiple disciplines of dentistry (orthodontics, prosthodontics, paediatric dentistry, surgery, and general dentistry) at an early stage is a must to ensure proper treatment and good prognosis. Replacement of CMT is very costly considering all the disciplines involved and the time it takes to finalise treatment, since complete growth is expected before starting with the prosthodontic and final portion of the treatment.2-5 In Ontario, there are various programs that aid parents with the financial burden of replacing CMT for their children (as long as the patient fits the criteria and is accepted into the program), but these programs have a maximum allowed for all the treatment, and they only provide coverage for a percentage of the grand total.6
Dental implants, orthodontic space closure, and retaining deciduous teeth are the most commonly prescribed treatment for replacement of CMT.2 However, there are other options that can be offered to patients as an interim or definitive basis. These options included fixed partial dentures, resin bonded prosthesis, partial dentures and complete overdentures.5
DENTAL IMPLANTS
Replacing CMT with dental implants has a good prognosis as long as there is adequate bone and attached soft tissue in the edentulous space in terms of local parameters.7 In most cases, there is the need for bone grafting and/or soft tissue grafting before placing a dental implant. This will not only increase the overall time in completing the treatment but also the costs associated with it. Many studies have been published about mucosal discoloration for implant fixtures and especially in fixtures when replacing teeth in the anterior mandible and in the anterior maxilla.7-9
The maxillary lateral incisor is the second most common congenitally absent tooth and since it is positioned in the esthetic zone, a replacement option should be carefully selected.2,8,9 There are three treatment options that exist for replacing missing lateral incisors. They include canine substitution, a tooth-supported restoration, or a single-tooth implant. Selecting the appropriate option depends on the malocclusion, specific space requirements, tooth-size relationship, and size and shape of the canine.4 The ideal treatment is the most conservative option that satisfies individual esthetic and functional requirements.
In Figs. 1-4 below, we see a patient with congenitally missing teeth.12,22,42 After orthodontic treatment provided proper spacing for missing teeth, the prosthodontic portion was then initiated.
Fig. 1

Fig. 2

Fig. 3

Fig. 4

Autogenous bone grafting in edentulous sites was first carried out, and then the patient was able to receive dental implants to replace his missing teeth.
When a patient is missing the majority of their teeth, dental implants become the treatment of choice, either to support a fixed partial denture or a removable partial/complete denture.11 Figs. 5-10 show a case where the diagnosis for the patient was ectodermal dysplasia. The patient was initially evaluated by different dental specialists when he was a child and then, when he completed his growth, a restorative treatment that suited his needs was carried out: full coverage restorations for existing malformed maxillary teeth which served as abutments for a maxillary partial denture, and 4 dental implants to retain a mandibular bar-overdenture.
Fig. 5
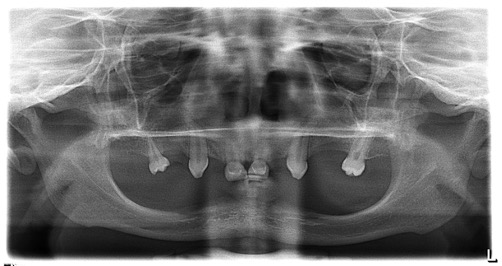
Fig. 6

Fig. 7
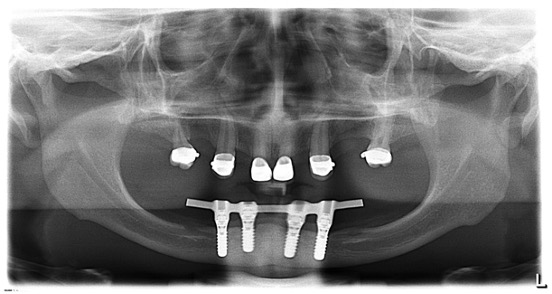
Fig. 8

Fig. 9

Fig. 10

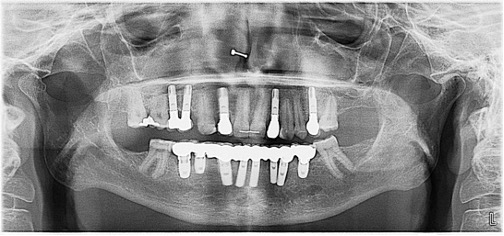
Most of these patients with CMT receive dental implant treatment as young adults, and they are expected to have proper dental maintenance throughout their lives. Implant ailment and failure years later can be catastrophic psychologically and financially.12-14 Figs. 11-14 shows a case where a then 18 year-old patient received implant supported fixed prosthesis to replace her CMT, 20 years later, she presented to my office with peri-implantitis around multiple implants, and fractured porcelain of her restorations. Treatment for this patient will involve periodontal, surgical and prosthodontic treatment.
Fig. 11

Fig. 12

Fig. 13

Fig. 14
ORTHODONTIC MOVEMENT (INCLUDES SPACE CLOSURE)
In almost all cases of CMT, an orthodontist is involved. Orthodontics will provide a proper positioning of present teeth and establishment of an ideal vertical dimension of occlusion, especially when the patient is missing multiple teeth in one of the arches as shown in Figs. 15 & 16.
Fig. 15

Fig. 16

Replacing the missing lateral incisors after opening the space with a removable, fixed, or implant retained prosthesis is one treatment option which demands long-term maintenance that can be quite costly.15 This can be avoided by using canine substitution to close the space. Evidence from practice indicates that patients with canine substitution have improved periodontal health and reported higher levels of satisfaction with their appearance compared to those with dental prostheses.12,13 Although the orthodontist positions the canine in the most aesthetic and functional location, the restorative dentist in most cases needs to place a porcelain or composite veneer or a crown to recreate normal lateral incisor shape and colour. Esthetic concerns have been cited when choosing to move the canines to the lateral positions when these are missing, however, this would be the most conservative treatment option.5,9,13 In Figs. 17-18, our patient had tooth 13 moved to the 12 position. After orthodontic treatment, a laminate veneer was placed on tooth 13 to reshape it, and having ceramic restorations for teeth14,11,21,22,23 helped improve the esthetic outcome.
Fig. 17

Fig. 18

The literature has also shown that patients tend to be more satisfied with the space closure treatment outcome compared to patients who underwent space opening and prosthetic replacement.4-5,7
FIXED PARTIAL DENTURES
Other options for replacement of CMT, especially when the edentulous space is short, include fixed partial dentures (FPDs).
A FPD is also an option when adjacent teeth need to be properly shaped and will receive or already have crowns. This is a great treatment modality when replacing mandibular incisors, since their replacement with dental implants will always require bone grafting and the implant diameter will still be narrow, which brings its own bio-mechanical challenges.16,17 Figs. 19-21 show replacement of CMT 31 and 41. There was limited buccolingual bone due to lingual concavity.The prosthetic space was too narrow for replacing 2 mandibular central incisors. With a 3-unit FPD, three mandibular incisors of similar dimensions were created.
Fig. 19

Fig. 20

Fig. 21

When congenitally missing lateral incisors, a resin-bonded fixed dental prosthesis (RBFDP) is also an excellent choice as long as there is a favourable occlusion, lack of signs of parafunction, lack of mobility of the abutments, and enough tooth surface for bonding the restoration.18 RBFDPs constitute a relatively minimal invasive approach and can serve either as a definitive or interim prosthesis until implant rehabilitation is permitted.19 Since its development in 1973, RBFDP has undergone significant alterations in design, materials, and tooth preparation. From the early technique of direct macromechanical bonding using a Rochette bridge,20 a perforated gold casting, to the Maryland bridge,21 a non-perforated, nonprecious metal alloy framework with micromechanical retention by electrolytic etching, these advancements have led to the evolvement of resin cements, fiber-reinforced resin, and ceramic materials.22 Nonetheless, the retentive capabilities of previous RBFDPs could frequently result in the loss of additional tooth structure, beyond the enamel boundaries, in order to achieve mechanical resistance for the prevention of debonding. With the introduction of all-ceramic RBFDPs in the early to mid-1990s, superior and more predictable bonding to the tooth structure could be obtained along with an enhanced aesthetic appearance.19,22,24
In the case shown in Figs. 22-24, a congenitally missing tooth 22 is replaced by a RBFDP. There was limited tooth surface on the lingual aspect of teeth 21 and 23, so crown lengthening was done before tooth preparation. All other inclusion criteria were met by the patient in order to treat her with a RBFPD.
Fig. 22

Fig. 23

Fig. 24

The disadvantages of a FPD treatment modality are: 1) a more meticulous hygiene is needed under the pontic region; 2) it is technique sensitive not only for the preparation of abutment teeth, but also for the cementation (especially for a RBFDP); 3) continuous bone resorption of the pontic region, resulting in a less esthetic appearance after a few years.16,19,22,24
REMOVABLE DENTURES
A removable denture is the most frequently used treatment for multiple CMT.25 When primary teeth are present for support, overdentures have been successful. In addition to being straightforward and inexpensive, removable dentures are a reversible and conservative treatment that will leave the teeth of the young patient intact and preserve the alveolar bone.26 Subsequently, the adult patient can be provided with a more definitive treatment, including implant-supported prostheses. Overdentures help to achieve better function, esthetics, and phonetics, along with improved self-image.27 Limitations of this option with very young patients include the patient’s failure to comply with oral hygiene, which may require several recall visits (3 to 4 months), daily application of stannous fluoride to minimise dental caries, and periodic replacement of the overdenture because of the child’s normal growth.28
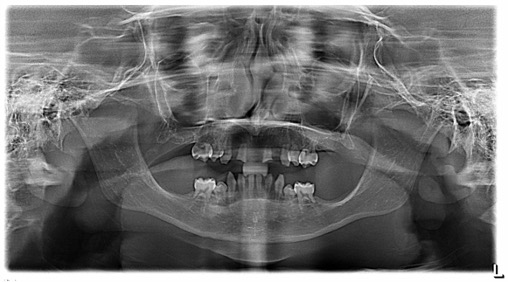
Removable partial or complete dentures are commonly used while patients with CMT complete their growth.29 In some cases, the patients will require several dental prostheses throughout the treatment span. Removable dentures are also used as a definitive prosthesis, especially if the patient is missing multiple teeth or all the teeth in one arch.30 In the case presented in Figs. 25-27 a panoramic radiograph shows absence of all permanent teeth for this 12-year-old patient. Removable tooth-supported overdentures can be used while the patient completes her growth, providing her with function and esthetics.
Fig. 25
Fig. 26

Fig. 27
The use of complete overdentures for the restoration of acquired and congenital anomalies that involve CMT has been advocated for many years. This therapeutic approach can provide an esthetic and functional restoration for missing, malformed, or discoloured dentition. For some patients, tissue coverage similar to a complete denture is disconcerting, especially when the majority of the teeth are present. The removable partial overdenture provides a functional, esthetic, and economical alternative.27,29,30
RETENTION OF DECIDUOUS TEETH
Retention of primary teeth resulting from CMT can greatly affect the proper spacing of dental arches and if in the esthetic zone, patient appearances.2,7 In many cases, retained primary teeth can be treated conservatively with composite restorations or porcelain veneers. When the extraction of retained primary teeth is indicated, dental implants offer a predictable outcome with known advantages.11 Figs 28 & 29, show a 50 year old patient with CMT maxillary canines with retained teeth 53 and 63. Tooth 53 presented significant mobility and a decision was made to remove the tooth and replace it with a dental implant. Tooth 63, which had a composite veneer, continued to be stable and the patient was never bothered by the esthetics.
Fig. 28

Fig. 29

Discussion:
Patients with CMT often raise difficult treatment planning issues. Therefore, to produce the most predictable esthetic and functional results, it is important to choose the treatment that will best address the initial diagnosis. Restoration of spaces in CMT patients needs to take into account many factors including, the number of missing teeth, the distribution of space, the size of the teeth, and the age of the patient. The importance of interdisciplinary team treatment planning is emphasised as a requirement for achieving optimal esthetics and function.1-5
Implant restorative treatment is commonly perceived as the most conservative approach, since it does not involve any modification or utilisation of the adjacent teeth. However, endosseous implant placement in growing patients is indicated until after the completion of craniofacial/skeletal growth unless severely partial or complete edentulism requires an earlier intervention. Several studies have suggested the continuation of craniofacial growth on average until the age 17 and 21 for females and males, respectively.14 The impact of facial growth on implant timing and position can be explained by the amount of implant submergence and displacement which in turn depends on the patient’s skeletal and dental age and growth pattern as well as the maxillary or mandibular positional placement. Taking into consideration that chronologic age is not sufficient in estimating growth, due to the significant variability within one gender, radiographics methods must be considered before any implant treatment attempt in young individuals.14
RBFDPs and implants are both minimally invasive treatment options for the replacement of single anterior missing teeth, with comparable levels of longevity and patient satisfaction. However, RBFDPs have the advantage of being an eligible option for young patients (as young as 10 years old), which is contraindicated for treatment with implants. Additionally, the replacement of a single anterior missing tooth with RBFDPs is still possible for those with limited available space (< 7 mm) or with angled roots of adjacent teeth; implantation placement in such individuals requires orthodontic treatment. Moreover, when compared with single implants, RBFDPs are a reversible option, require shorter treatment time, cost less and require less demanding postoperative care.7-12,18,19
Finally, since the majority of the treatment is completed when patients are young adults, conversations with parents should also include the importance of long-term maintenance and possible complications of treatment.
Oral Health welcomes this original article.
References
- Durey K, Cook P, Chan M. The management of severe hypodontia. Part 1: Considerations and conventional restorative options. Br Dent J. 2014 Jan;216(1):25-9.
- Bishop K, Addy L, Knox J. Modern restorative management of patients with congenitally missing teeth: Conventional restorative options and considerations. Dent Update. 2007 Jan-Feb;34(1):30-2, 34, 37-8.
- Rakhshan V, Rakhshan H. Meta-analysis of congenitally missing teeth in the permanent dentition: Prevalence, variations across ethnicities, regions and time. Int Orthod. 2015 Sep;13(3):261-73.
- Heuberer S, Ulm C, Zechner W, Laky B, Watzak G. Patterns of congenitally missing teeth of non-syndromic and syndromic patients treated at a single-centre over the past thirty years. Arch Oral Biol. 2019 Feb;98:140-147.
- Krassnig M, Fickl S. Congenitally missing lateral incisors—a comparison between restorative, implant, and orthodontic approaches. Dent Clin North Am. 2011 Apr;55(2):283-99, viii.
- https://www.sickkids.ca/en/care-services/clinical-departments/dentistry/#programs
- Cosyn J, Wessels R, Garcia Cabeza R, Ackerman J, Eeckhout C, Christiaens V. Soft tissue metric parameters, methods and aesthetic indices in implant dentistry: A critical review. Clin Oral Implants Res. 2021 Oct;32 Suppl 21:93-107.
- Lacarbonara M, Cazzolla AP, Lacarbonara V, Lo Muzio L, Ciavarella D, Testa NF, Crincoli V, Di Venere D, De Franco A, Tripodi D, Grassi FR, Capogreco M. Prosthetic rehabilitation of maxillary lateral incisors agenesis using dental mini-implants: a multicenter 10-year follow-up. Clin Oral Investig. 2022 Feb;26(2):1963-1974.
- Kinzer GA, Kokich VO Jr. Managing congenitally missing lateral incisors. Part III: single-tooth implants. J Esthet Restor Dent. 2005;17(4):202-10.
- Knobloch LA, Larsen PE, Saponaro PC, L’Homme-Langlois E. Early implant placement for a patient with ectodermal dysplasia: Thirteen years of clinical care. J Prosthet Dent. 2018 May;119(5):702-709.
- Ben Gassem A, Hashem D. Multidisciplinary management of congenitally missing lateral incisors: A minimally invasive approach. Clin Case Rep. 2021 Jul 26;9(7):e04521.
- Naoum S, Allan Z, Yeap CK, Razza JM, Murray K, Turlach B, Goonewardene MS. Trends In orthodontic management strategies for patients with congenitally missing lateral incisors and premolars. Angle Orthod. 2021 Jul 1;91(4):477-483.
- Brough E, Donaldson AN, Naini FB. Canine substitution for missing maxillary lateral incisors: the influence of canine morphology, size, and shade on perceptions of smile attractiveness. Am J Orthod Dentofacial Orthop. 2010 Dec;138(6):705.e1-9; discussion 705-7.
- Borzabadi-Farahani A. Orthodontic considerations in restorative management of hypodontia patients with endosseous implants. J Oral Implantol. 2012 Dec;38(6):779-91
- Kokich VO Jr, Kinzer GA. Managing congenitally missing lateral incisors. Part I: Canine substitution. J Esthet Restor Dent. 2005;17(1):5-10.
- Kinzer GA, Kokich VO Jr. Managing congenitally missing lateral incisors. Part II: tooth-supported restorations. J Esthet Restor Dent. 2005;17(2):76-84.
- Newman GV, Newman RA. Report of four familial cases with congenitally missing mandibular incisors. Am J Orthod Dentofacial Orthop. 1998 Aug;114(2):195-207.
- Brignardello-Petersen R. All zirconia resin-bonded fixed dental prostheses replacing missing incisors probably have a high 10-year survival rate in patients who are highly compliant. J Am Dent Assoc. 2017 Dec;148(12):e202.
- Balasubramaniam GR. Predictability of resin bonded bridges–a systematic review. Br Dent J. 2017 Jun 9;222(11):849-858.
- Thomas GD. Rochette bridge: current techniques. Dent Tech. 1983 Mar;36(3):11-5
- Thompson VP. Whence the Maryland Bridge? The evolution of the adhesive bridge. Dent Hist. 2017 Jan;62(1):9-14.
- Kern M, Passia N, Sasse M, Yazigi C. Ten-year outcome of zirconia ceramic cantilever resin-bonded fixed dental prostheses and the influence of the reasons for missing incisors. J Dent. 2017 Oct;65:51-55.
- Hvaring CL, Øgaard B, Birkeland K. Tooth replacements in young adults with severe hypodontia: Orthodontic space closure, dental implants, and tooth-supported fixed dental prostheses. A follow-up study. Am J Orthod Dentofacial Orthop. 2016 Oct;150(4):620-626.
- Stylianou A, Liu PR, O’Neal SJ, Essig ME. Restoring Congenitally Missing Maxillary Lateral Incisors Using Zirconia-Based Resin Bonded Prostheses. J Esthet Restor Dent. 2016 Jan-Feb;28(1):8-17.
- Guo TW, Xing HL, Wang J, Wang BC. [Summary of 61 cases of removable denture restoration in children with congenital tooth deficiency]. Shanghai Kou Qiang Yi Xue. 2019 Aprial;28(2):196-200.
- Alsayed HD, Alqahtani NM, Alzayer YM, Morton D, Levon JA, Baba NZ. Prosthodontic rehabilitation with monolithic, multichromatic, CAD-CAM complete overdentures in an adolescent patient with ectodermal dysplasia: A clinical report. J Prosthet Dent. 2018 Jun;119(6):873-878.
- Kutkut A, Abu-Eid R, Sharab L, Abadi B, Van Sickels J. Full Mouth Implant-supported Rehabilitation of a Patient with Ectodermal Dysplasia: Clinical Report and Literature Review. J Int Acad Periodontol. 2015 Apr;17(2):34-41.
- Rakhshan V. Congenitally missing teeth (hypodontia): A review of the literature concerning the etiology, prevalence, risk factors, patterns and treatment. Dent Res J (Isfahan). 2015 Jan-Feb;12(1):1-13.
- Rogoff GS, Graser GN. Overdentures for acquired and congenital anomalies: 1. Complete dentures. Int J Prosthodont. 1990 May-Jun;3(3):229-37.
- Graser GN, Rogoff GS. Overdentures for acquired and congenital anomalies: 2. Partial overdentures. Int J Prosthodont. 1990 Jul-Aug;3(4):361-7.
About the Author
 Cecilia Aragon is a Prosthodontist who maintains a full-time private practice in London, Canada. She is an Adjunct Clinical Professor at the Schulich School of Dentistry and a Lecturer at the Faculty of Dentistry at the University of Toronto. She is also a Staff member at the Thames Valley Children’s Centre. E-mail: doctor@aragonprosthodontics.com www.aragonprosthodontics.com
Cecilia Aragon is a Prosthodontist who maintains a full-time private practice in London, Canada. She is an Adjunct Clinical Professor at the Schulich School of Dentistry and a Lecturer at the Faculty of Dentistry at the University of Toronto. She is also a Staff member at the Thames Valley Children’s Centre. E-mail: doctor@aragonprosthodontics.com www.aragonprosthodontics.com
RELATED ARTICLE: Congenitally Missing Teeth: A Prosthodontic Case Report










