
The ultimate goal of endodontic treatment is the prevention and/or treatment of apical periodontitis, such that there is complete healing and absence of infection1 while the overall long-term goal is the placement of a definitive, clinically successful restoration and preservation of the tooth.2
Successful endodontic treatment depends on a number of factors, including proper instrumentation, successful irrigation and decontamination of the root-canal system right to the apical terminus in addition to hard to reach areas such as isthmuses, and lateral and accessory canals3,4 (Fig. 1a & 1b).
The complexity of root canal anatomy is demonstrated by these cleared samples of maxillary molars.
FIGURE 1A. FIGURE 1B.


The challenge for successful endodontic treatment has always been the removal of vital and necrotic remnants of pulp tissue, debris generated during instrumentation, the smear layer,
micro-organisms, and micro-toxins from the root-canal system.5
It has been accepted that even with the use of rotary instrumentation, the nickel-titanium instruments currently available only act on the central body of the root canal, resulting in a reliance on irrigation to clean beyond what may be achieved by these instruments.6 “Shaping canals creates sufficient space to hold an effective reservoir of irrigant that, upon activation, can penetrate, circulate and digest tissue from the uninstrumentable portions of the root canal system”.7,8
Several challenges often arise during root canal preparation. Some of the most common ones are anatomic factors that may prevent negotiation to the apical termini as well as ledge formation, perforation and file separation.
The introduction of Nickel-Titanium (NiTi) alloy in endodontics presented a significant improvement, allowing good results in terms of cleaning and shaping of root canals, while reducing operative time and minimizing iatrogenic errors.9,10
Thanks to the superior mechanical properties of the NiTi alloy it was possible to use endodontic instruments of greater tapers in continuous rotation, increasing the effectiveness and rapidity of the cutting. However, several studies reported a significant risk of intracanal separation of NiTi Rotary instruments.11-14 In fact, file separation via torsional and cyclic fatigue has created the biggest fear and risk for dentists using rotary nickel titanium (NiTi) files for root canal treatment.11,12,15
Although multiple factors contribute to file separation, cyclic fatigue has been shown as one of the leading causes.16 Fatigue failure usually occurs by the formation of micro cracks at the surface of the file that starts from surface irregularities often caused by the grinding process during the manufacturing. During each loading cycle micro cracks develop, propagating getting deeper in the material, until complete separation of the file occurs.17 All endodontic files shows some irregularities on the surface, and inner defect, as a consequence of the manufacturing process, and distribution of these defects influence fracture strength of the endodontic instruments.18,19
Since the introduction of NiTi in 198820, varied instrument designs with claims of superior cyclic fatigue resistance have been propagated. However, there were no major changes in the manufacturing process/raw materials until the introduction of the second generation of NiTi files, ie, M-Wire (Dentsply Tulsa Dental Specialties, Tulsa, OK) in 2007 and Twisted File (TFTM) (Kerr Endodontics Formerly Axis/SybronEndo, Orange, CA) in 2008.
TF™instruments are manufactured using a proprietary heat treatment technology which changes the crystalline structure completely so the triangular cross section NiTi file blank can be twisted while maintaining the natural grain structure. “More precisely, TF™ instruments are created by taking a raw NiTi wire in the austenite crystalline structure phase and transforming it into a different phase of crystalline structure (R-phase) by a process of heating and cooling. In the R-phase, NiTi cannot be ground but it can be twisted. Once twisted, the file is heated and cooled again to maintain its new shape and convert it back into the austenite crystalline structure, which is super elastic once stressed. The manufacturing process aims at respecting the grain structure for maximum strength as grinding creates micro fracture points during the manufacturing of the instruments. Because TF™ files are twisted and not ground, no surface microfractures occur on their surface and therefore do not need be polished away; thereby not dulling the cutting edges and retaining their efficient cutting ability.”21-23
Because of the increased flexibility, the Twisted Files maintains the original canal shape better, minimizes canal transportation and stays centered even in severely curved root canals.24,25
In addition to the development of heat treated Twisted File™ technology to improve the performance and safety of NiTi instruments, the file design has also been changed with respect file dimensions, tip configuration, cross-section and flute design. More recently, a third factor has become important in this search for stronger and better instruments: Movement Kinematics, the branch of motion in which the objects move.26
“For more than a decade, NiTi instruments have been traditionally used with a continuous rotary motion, but more recently a new approach to the use of NiTi instruments in a reciprocating movement had been introduced by Yared.11 The clockwise (CW) and the counterclockwise (CCW) rotations used by Yared were four-tenths and two-tenths of a circle respectively and the rotational speed utilized was 400 rpm. The concept of using a single NiTi instrument to prepare the entire root canal was made possible due to the fact that a reciprocating motion is thought to reduce instrumentation stress.
Recent literature data shows that a reciprocating motion can extend cyclic fatigue resistance of NiTi instruments when compared to continuous rotation,27,28 mainly because it reduces instrument stress. As the instrument rotates in one direction (usually the larger angle) it cuts and becomes engaged into the canal then it disengages in the opposite direction (usually with the smaller angle) and the stresses are therefore reduced. Following these concepts new instruments have been recently commercialized; Reciproc (VDW, Munich, Germany) and WaveOne (Dentsply Maillefer, Ballaigues, Switzerland), which uses specifically developed motors that produce a specific reciprocating movement (using approximately 150 to 30°angles).
This reduction of instrumentation stress (both torsional and bending stress) is the main advantage of reciprocating movements. It has been shown that a lot of different reciprocating movements can be used, each one affecting the performance and the safety of the NiTi instruments. Therefore, when discussing the advantages and disadvantages of reciprocation, the exact motion should also be mentioned, since the actual angle of reciprocation can have substantial influence on both the clinical and experimental behaviour of NiTi instruments.”15
Another possible advantage of reciprocation could be better maintenance of original canal trajectory, mainly related to lower instrumentation stress and consequently its elastic return. However, it must be underlined that reciprocation does not affect the inherent rigidity of the instruments. If a quite rigid Niti instrument of greater taper is slightly forced into a curved canal, it will create more canal transportation than a more flexible one, due to its inherent tendency to straighten. Moreover, tip design could strongly influence canal transportation, with a cutting tip being more dangerous that a non-cutting pilot tip.
While reciprocation with NiTi instruments have become very popular in recent years, with a significant number of published articles, some of these studies have shown that there is also inherent disadvantages in the reciprocating movements.
It is well known that a small inadvertent extrusion of debris and irrigants into the periapical tissues is a frequent complication during the cleaning and shaping procedures, both with manual stainless steel and nickel-titanium rotary instrumentation techniques.29,30 However, recent studies have shown that commercially available reciprocating instrumentation techniques seem to significantly increase the amount of debris extruded beyond the apex31,32 and, consequently, the risk of postoperative pain. A clinical study comparing Reciproc and NiTi rotary instruments has also confirmed these findings.33
Since reciprocation movement is formed by a wider cutting angle and a smaller releasing angle, while rotating in the releasing angle, the flutes will not remove debris but push them apically. Reciproc and WaveOne motions are very similar (even if not precisely disclosed by manufacturers), and this fact could also explain the higher incidence and intensity of postoperative pain that has been found in recent research studies.33,34
Moreover, both WaveOne and Reciproc techniques use a quite rigid, large single-file of increased taper (usually 08 taper, size 25), which is directed to reach the apex. In many cases, in order to reach the apical working length, reciprocating instruments are used with apically directed pressure, which produces an effective piston to propel debris through a patent apical foramen, and possibly directing debris laterally, making canal debridement more difficult. Since instruments are commonly used without first performing preliminary coronal enlargement, this may result in a greater engagement of the file flutes and consequently may produce more torque and/or applied pressure on the file. Moreover, the cutting ability of a reciprocating file is decreased when compared to continuous rotation. Debris removal is also less, thus increasing the frictional stress and torque demand on the file, due to entrapment of debris within the flutes. To reduce this tendency some authors have advocated the use of NiTi rotary glide-path instruments, before using a WaveOne or Reciproc instruments, but in this case the overall technique is no longer a single file technique but a more complex and more costly technique which utilizes two different types of Niti instruments, glide path instruments and then shapers.”35,15
TF™ Adaptive
The TF™Adaptive technique has been proposed in order to maximize the advantages of reciprocation, while minimizing its disadvantages. By using a unique, patented motion, the innovative TF™ Adaptive Motion technology, together with an original three-file technique, most clinical cases can be treated effectively and safely (Fig. 2).
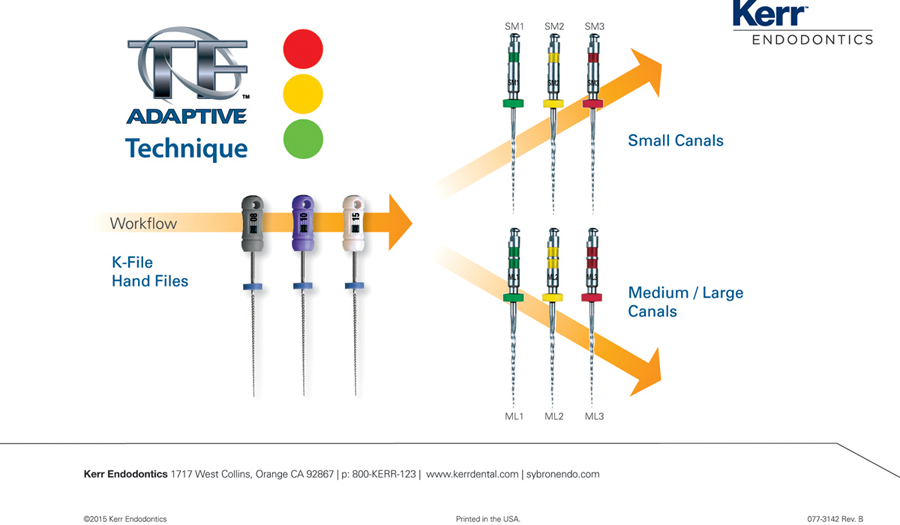
FIGURE 2. Colour-Coded File Identification. An intuitive, color-coded system designed for efficiency and ease of use. Just like a traffic light – start with green and stop with red.

TF™ Adaptive employs a patented unique motion technology, which automatically adapts to instrumentation stress, when used in the Elements Motor while in TFTM Adaptive setting (Fig. 3). When the TF™Adaptive instrument is not (or very lightly) stressed in the canal, the movement can be described as a continuous rotation, allowing better cutting efficiency and removal of debris. The cross-sectional and flute design are meant to perform at their best in a clockwise motion.
FIGURE 3. Elements™ Motor. Settings for TF™ Adaptive, TF™, K3, Lightspeed, M4 Safety Handpiece and custom settings for personal preference.

More precisely, it is an interrupted motion with the following CW-CCW angles: 600-0°. This interrupted motion is as effective as continuous rotation in lateral cutting, allowing optimal brushing or circumferential filing for better debris removal in oval canals. This interrupted motion also minimizes iatrogenic errors by reducing the tendency of “screwing in” (aka pull down), that is commonly seen with NiTi instruments of great taper that are used in continuous rotation.
On the contrary, while negotiating the canal, due to increased instrumentation stress and metal fatigue, the motion of the TF™ Adaptive instrument changes into a reciprocation mode, with specifically designed CW and CCW angles which may vary from 600-0° to 370-50° (Fig. 4). These angles are not constant, but vary depending on the anatomical complexities and the intracanal stresses placed on the instrument. This “adaptive” motion is therefore meant to reduce the risk of intracanal failure, without affecting performance, due to the fact that the best movement for each different clinical situation is automatically selected by the Adaptive motor. It is quite interesting that the clinician will hardly perceive the differences in the changing motion, due to a very sophisticated algorithm, which permits a smooth transition between the changing angles.
FIGURE 4. The motion of TF™ Adaptive instrument changes from rotary into reciprocation mode, with specifically designed CW and CCW angles which may vary from 600-0° to 370-50°.

As far as disadvantages of reciprocation are concerned, TF™ Adaptive motion is a reciprocating motion with cutting angles (CW angles) much greater than WaveOne/Reciproc movements. This results in the TF™ Adaptive instrument is working for a longer time with a CW angle, which allows better cutting efficiency and removal of debris (and less tendency to push debris apically and laterally), because the flutes are designed to remove debris in a CW rotation. This results in TF™Adaptive taking advantage of the use of a motion that is more similar to continuous rotation for optimal debris removal. There are obviously some changes in the angles depending on canal anatomy (the more complex, the smaller the CW angle), but they do not seem to significantly influence the overall result. On the contrary, these changes influence resistance to metal fatigue, since TF™ instruments used with Adaptive motion were found to have superior resistance to cyclic fatigue when compared to the same TF™ instruments used in continuous rotation.36
As mentioned before, flexibility is a fundamental property to minimize iatrogenic errors while negotiating canals, both in reciprocation and in continuous rotation. The use of a reciprocating movement, therefore, does not significantly help a NiTi instrument of greater taper to negotiate curved canals with no iatrogenic errors. It mainly helps to reduce instrumentation stress and the risk of intracanal failure. In addition, a study aimed to compare the frequency of dentinal microcracks after root canal shaping with two reciprocating (Reciproc and WaveOne) and one combined continuous reciprocating motion Twisted Files Adaptive (TFA) rotary system. Ninety molars were chosen and divided into three groups of 30 each. Root canal preparation was achieved by using Reciproc R25, Primary WaveOne and TFA systems. All the roots were horizontally sectioned at 15, 9, and 3 mm from the apex. The slices were then viewed each under a microscope at ×25 magnification to determine the presence of cracks. The absence/presence of cracks was recorded, and the data were analyzed with a Chi‑square test. The significance level was set at P < 0.05. The results found that instrumentation with Reciproc produced significantly more complete cracks than WaveOne and TFA (P = 0.032). The TFA system produced significantly less cracks then the Reciproc and WaveOne systems apically (P = 0.004). The study concluded that within the limits of this study, the TFA system caused less cracks then the full reciprocating system (Reciproc and WaveOne). Single‑file reciprocating files produced significantly more incomplete dentinal cracks than full‑sequence adaptive rotary motion.39
The TF™ Adaptive technique is basically a three file technique, designed to treat the majority of cases encountered in clinical practice. Available are two sets of three file systems, one for small, calcifying and severely curved canals and one system for more “standard” and larger canals, allowing adequate taper and increased apical preparation in both scenarios. The number of instruments within each sequence can also vary and adapt to canal anatomy, with the last instrument of the sequence used only when a greater apical enlargement is needed due to larger original canal dimensions and/or enhanced final irrigation techniques. The sequences are also different in their shaping concepts. Each file of the sequence being used is taken to full working length in a “crown down” manner such that the root canal wall is internally sculpted
incrementally, allowing dentin debris and tissue to be evacuated coronally rather than to be pushed apically. This may reduce the risk of canal blockage and the extrusion of debris into the apical tissues. The SM 1 file (single colour band green, 04 taper 20 tip size) is an excellent flexible Glide Path file which may be used with either sequence to pre-enlarge the canal thereby decreasing instrument stress for the next larger size file in sequence. This also allows better maintenance of the original canal trajectory (Fig. 2, 5).
The final apical enlargement with a size #35 file is not only meant to allow the use of the Endovac (EndoVac™ Kerr Endodontics, Orange, CA) irrigation technique, but to improve canal shaping by touching more canal walls. Figure 6 clearly shows how improved and deeper the apical one-third shape is when a 06 taper 35 tip instrument follows a 08 taper 25 tip instrument. This is why in the majority of cases two instruments are much better than a single file technique, provided that the second instrument is a flexible one. The superior flexibility allowed by the use of TFTM technology permits TFTM Adaptive to follow these criteria, and safely enlarge canals with minimal risk of iatrogenic errors like tooth weakening and canal/apical transportation. The use of a more rigid alloy would have not made this possible, especially in curved canals.”15
TF™ Adaptive Technique
TFTM Adaptive is an intuitive, color-coded system designed for efficiency and ease of use. The colour-coded system is based on a traffic light. The first instrument in sequence is green. The second instrument in sequence is yellow and the third instrument in sequence, if required, is red. Green means go. Yellow means continue or stop. Red means stop (Fig. 2).
Coronal Access And Glide Path
1. Place rubber dam.
2. Obtain straight line coronal access with slightly diverging axial walls adhering to the concept of Minmimally Invasive Endodontics.37
3. Achieve apical patency and establish an apical glide path using #8 hand file, follow that with a #10 hand file and continue at least with a #15 hand file. Glide path may be facilitated with the M4 Safety Handpiece (Kerr Endodontics, Orange, CA) (Fig. 7). The pulp chamber should be filled brimful with NaOCl (Sodium Hypochlorite).
Canal Size And File Sequence Determination
(Figs. 5 & 8)
FIGURE 5. File Size Reference Chart.
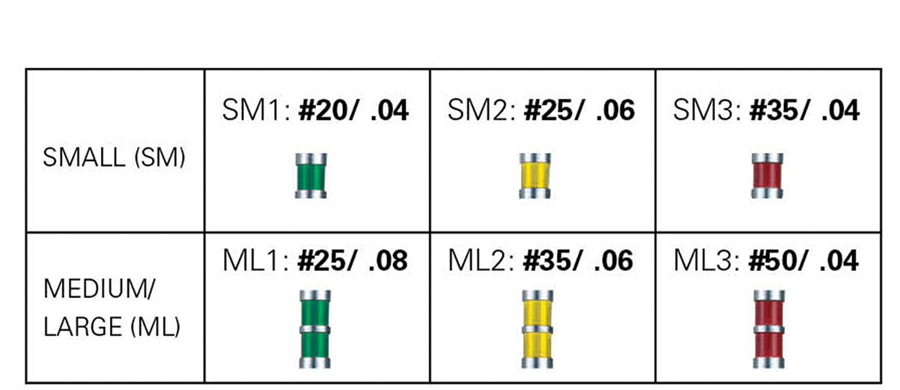
FIGURE 6. Deep Shaping. The clinical use of a second instrument (06/35) after the 08/25 significantly increases the preparation in the apical one third, improving the quality of canal shaping and allowing room for enhanced irrigation. This will also allow the use of the apical negative pressure devices such as the EndoVac to safely deliver abundant quantities of sodium hypochlorite to the apex without
the risk of apical extrusion.

FIGURE 7. M4 Safety Handpiece.

FIGURE 8. TF™ Adaptive Technique Card. Size and Sequence Determination.
Small Canals (SM)
Using tactile feel, if you struggle to get a #15 K-File to Working Length (WL) then the canal size is deemed to be “Small”. Use the Small Pack (one color band) and its instrument sequence. The small sequence may also be used in severely curved canals as well as roots that may be very thin and the risk of strip perforation is a possibility.
Medium/Large Canals (ML)
Using tactile feel, if a #15 K-File feels loose at working length then the canal size is deemed to be “Medium/ Large”. Use the Medium/Large Pack (two color bands) and its instrument sequence.
Establish Working Length
Working length should be established with a reliable apex locator. A radiograph may help the clinician as well.
TF™ Adaptive Canal Shaping Technique
1. Use the “TF™ Adaptive” setting on your Elements Motor. Figure #3
2. Ensure the pulp chamber is flooded with NaOCl or EDTA and make sure the file is rotating as you enter the canal.
3. Slowly advance the green (SM1 or ML1) with a single
controlled motion until the file engages dentin then completely withdraw the file from the canal. Do not force apically. Do not peck.
4. Wipe off the flutes. Deliver irrigant to the pulp chamber and confirm canal patency with a #15 handfile K-File.
5. Repeat steps 3 and 4 using the file you started with until working length is achieved.
6. Repeat steps 3 and 4 with the yellow SM2 or ML2 until the file reaches working length. If the desired apical size is achieved the sequence is complete. For larger apical sizes, repeat steps 3 and 4 with the red SM3 or ML3 until the file reaches working length.
Note: All TFA files may be used in a brushing manner directed towards the external surface of the root away from the canal curvature when retrieving the file from the canals.
Irrigate And Dry
When irrigating with EndoVac™, (apical negative pressure irrigation system),2 in small canals, you must take SM3 to working length. In medium/ large canals, you must take at least ML2 to working length. Note that the Microcannula is .32 mm in diameter (Fig. 9).
TF™ Adaptive matching Paper Points may be used to dry the canals.
FIGURE 9. EndoVacTM Apical Negative Pressure Irrigation System. The Master Delivery Tip (MDT) accommodates different sizes of syringes filled with irrigant, the macro cannula is attached to the autoclavable aluminum hand piece and the micro cannula is attached to an autoclavable aluminum finger piece. The macro cannula, the micro cannula and the MDT are connected via clear plastic tubing. The tubes are connected to the high volume suction of the dental chair via the Multi-Port Adaptor.

Obturation
TF™ Adaptive matching Gutta Percha in combination with the ElementsTM Free Cordless Obturation system37 may be used to obturate the root canal system. Alternatively, TF™ Adaptive carriers may be used.
CONCLUSIONS
TFA employs Twisted File technology and Adaptive Motion Technology. The TFTM Adaptive file design is based on clinically proven Twisted File technology, which means the file is twisted to shape for improved file durability, features R-Phase Technology to improve file flexibility and strength while maintaining the original canal curvature minimizing canal and apical transporation (Fig. 10).
FIGURE 10. CBCT (Cone Beam Computerized Tomography) three dimensional visualization of TFA preparation (SM sequence) in a complex molar, showing proper shape, tapered preparation and excellent maintenance of canal trajectories. Courtesy: Dr. Lucila Piasecki, Brazil and Dr. Gianluca Gambarini, Italy.

Adaptive Motion Technology is based on a patented, smart algorithm designed to work with the TF™ Adaptive file system. The authors have also found that Adaptive Motion Technology works well with other ground file rotary systems making their use safer especially in smaller and curved canals. This technology allows the TF™Adaptive file to adjust to intra-canal torsional forces depending on the amount of pressure placed on the file. This means the file is in either a rotary or reciprocation motion depending on the situation and adjusts appropriately.
This winning combination results in exceptional debris removal with the tried and trusted classic rotary Twisted File design and less chance of file pull down and debris extrusion with Adaptive Motion Technology.OH
Dr. Gary Glassman is the author of numerous publications. He lectures globally on endodontics, is on staff at the University of Toronto, Faculty of Dentistry in the graduate department of endodontics, and is Adjunct Professor of Dentistry and Director of Endodontic Programming for the University of Technology, Kingston, Jamaica. Gary is a fellow of the Royal College of Dentists of Canada, Fellow of the American College of Dentists and the endodontic editor for Oral Health dental journal. He maintains a private practice, Endodontic Specialists in Toronto, Ontario, Canada. His website is www.drgaryglassman.com and his office website is www.rootcanals.ca. He can be reached at drg@drgaryglassman.com.
Gianluca Gambarini is a full-time Professor of Endodontics, University of Rome, La Sapienza, Dental School. He is head of the Endodontic Department International lecturer and researcher. He is author of more than 450 scientific articles, three books and chapters in other books. He has lectured all over the world (more than 350 presentations) and has been invited as a main speaker in the most important international (AAE, IFEA, ESE) and national endodontic congresses in Europe, North and South America, Asia, Middle East, Australia and South Africa. Gianluca Gambarini still maintains a private practice limited to Endodontics in Rome, Italy.
Dr Sergio A. Rosler has been the Assistant Clinical Teacher in numerous graduate and post-graduate Endodontic Programs and was Clinical Fellow Teacher at Warwick Dentistry University in the United Kingdom. Dr. Rosler has lectured at conferences and several universities around the world. He maintains a private practice limited to Endodontics in Buenos Aires, Argentine and can be reached at sergiorosler@gmail.com.
Disclaimer: Drs. Gambarini and Glassman are the inventors of Adaptive Motion and receive a nominal royalty from Kerr.
Oral Health welcomes this original article.
References
1. Orstavik D, Pittford T. Essential endodontology: prevention and treatment of apical periodontitis. 2nd ed. Ames, IA: Blackwell Munksgaard Ltd; 2008:1.
2. Glassman G, Charara K . EndoVacTM Apical Negative Pressure: Safe and Effective Endodontic Irrigation from Beginning to END. Oral Health Dental Journal, May 2015, 8-14.
3. Friedman S. Prognosis of initial endodontic. Endod Top. 2002;2:59–88.
4. Schilder H. Cleaning and shaping the root canal Dent Clin North Am 1974;18:269-96.
5. Gu LS, Kim JR, Ling J, Choi KK, Pashley DH, Tay FR. Review of contemporary
6. Peters OA. Current challenges and concepts in the preparation of root canal systems: A review. J Endod. 2004;30:559-67.
7. Ruddle C. Endodontic Disinfection: Tsunami Irrigation. Endodontic Practice, 11(1): 7-15.
8. Ruddle C. Predictably Successful Endodontics. Spectrum Dental Teamwork,Vol. 8 No. 6 June/July 2015.20-25.
9. Xu X, Zheng Y. Comparative study of torsional and bending properties ifor sx models of nickel-titanium root canal instruments with different cross-sections. J Endod. 2006; 32: 372–5.
10. Gergi R, Rjeily JA, Sader J, Naaman A. Comparison of canal transportation and centering ability of twisted files, Pathfile-ProTaper system, and stainless steel hand K-files by using computed tomography. J Endod. 2010 May;36(5):904-7.
11. Yared G. In vitro study of the torsional properties of new and used ProFile nickel titanium rotary files. J Endod. 2004 Jun;30(6):410-2.
12. Pruett JP, Clement DJ, Carnes DL Jr.Cyclic fatigue testing of nickel-titanium endodontic instruments. J Endod 1997 Feb;23(2):77-85.
13. Tripi TR, Bonaccorso A, Condorelli GG.Cyclic fatigue of different nickel-titanium endodontic rotary instruments. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006 Oct;102(4):e106-14.
14. Sattapan B. Nervo GJ, Palamara JE, Messer HH. Defects in rotary nickel-titanium files after clinical use J Endod 2000; 26:161-5.
15. Gambarini G, Glassman G. TF Adaptive: A Novel Approach to Nickel-Titanium Instrumentation. “Rotary when you want it, Reciprocation when you need it”. Oral Health Dental Journal, May 2013, 22-30.
16. Shen Y, Cheung GS, Bian Z, Peng B.Comparison of defects in ProFile and ProTaper systems after clinical use. J Endod. 2006 Jan;32(1):61-5.
17. Christ HJ. Fundamental mechanisms of fatigue and fracture. Student Health Technology Information 2008 ;133: 56–67.
18. Anderson ME, Price JW, Parashos P. Fracture resistance of electropolished rotary nickel-titanium endodontic instruments. J of Endod 2007;33: 1212–26.
19. Wei X, Ling J, Jiang J, Huang X, Liu L. Modes of failure of ProTaper nickel-titanium rotary instruments after clinical use. J Endod. 2007; 33: 276–9.
20. Walia H, Brantley WA, Gerstein H. An initial investigation of the bending and torsional properties of nitinol root canal files. J Endod 1988;14:346–51.
21. Gambarini G, Grande NM, Plotino G, et al. Fatigue resistance of engine driven rotary nickel-titanium instruments produced by newer manufacturing methods. J Endod 2008;34:1003–5.
22. Bhagabati N, Yadav S, MDS, Talwar S. An In Vitro Cyclic Fatigue Analysis of Different Endodontic Nickel-Titanium Rotary Instruments. J Endod, Vol 38 No. 4 April 2012. 515-518.
23. Gambarini G, Grande NM, Plotino G, Somma F, Garala M, De Luca M, Testarelli L. Fatigue Resistance of Engine-driven Rotary Nickel-Titanium Instruments Produced byNew Manufacturing Methods, J Endod, Vol 34, No 8, August 2008, 1003-1005.
24. Zhao D, Shen Y, Peng B, Haapasalo M. Micro–Computed Tomography Evaluation of the Preparation of Mesiobuccal Root Canals in Maxillary First Molars with Hyflex CM, Twisted Files, and K3 Instruments. J Endod, Vol 39, No 3, March 2013, 385-388.
25. Hashem A, Galal Ghoneim A, Lutfy RA, Yehia Foda M, Fatah Omar GA. Geometric Analysis of Root Canals Prepared by Four Rotary NiTi Shaping Systems. JEndod, Vol 38, No 7, July 2012, 996-1000.
26. Gambarini G, Rubini AG, Al Sudani D, Gergi R, Culla A, De Angelis F, Di Carlo S, Pompa G, Osta N, Testarelli L. Influence of Different Angles of Reciprocation on the Cyclic Fatigue of Nickel-Titanium Endodontic Instruments, J Endod, Vol 38, No 10, October 2012, 1408-1411.
27. De-Deus, E. J. L. Moreira, H. P. Lopes & C. N. Elias. Extended cyclic fatigue life of F2 ProTaper instruments used in reciprocating movement. Int Endod J. 2010 Dec;43(12):1063-8.
28. You SY, Bae KS, Baek SH, Kum KY, Shon WJ, Lee W. Lifespan of One Nickel-Titanium Rotary File with Reciprocating Motion in Curved Root Canals. J Endod. 2010 ;36:1991-4.
29. Oginni A, Udoye C. Endodontic flare-ups: comparison of incidence between single and multiple visit procedures in patients attending a Nigerian teaching hospital. BMC Oral Health. 2004; 4: 4–6.
30. Siqueira JF, Jr, Rocas IN, Favieri A, Machado AG, Gahyva SM, Oliveira JC, Abad EC. Incidence of postoperative pain after intracanal procedures based on an antimicrobial strategy. J Endod. 2002; 28: 457–460.
31. Bürklein S, Schäfer E. Apically extruded debris with reciprocating single-fileand full-sequence rotary instrumentation systems. J Endod. 2012;38: 850-2.
32. Jaramillo D, Aguilar E, Leon M, Aprecio R. Comparison of the Extrusion of Dentin Debris Using a New Instrumentation Concept, Oral Health Dental Journal, May 2015, 28-32.
33. Gambarini, G., Sudani, D.A.L., Di Carlo, S., Pompa, G., Pacifici, A., Pacifici, L., Testarelli, L.Incidence and intensivity of postoperative pain and periapical inflammation after endodontic treatment with two different instrumentation techniques. Europ. J. Inflam.2102 ; 10 :99-103.
34. Gambarini G, Testarelli L, De Luca M. Milana V, Plotino G, Grande NM, Giansiracusa A, Al Sudani D, Sannino G. influence of three different instrumentation techniques on the incidence of postoperative pain after endodontic treatment . Annali di Stomatologia 2013:1; 138-41
35. Berutti E, Paolino DS, Chiandussi G, Alovisi M, Cantatore G, Castellucci A,Pasqualini D. Root canal anatomy preservation of WaveOne reciprocating files with or without glide path. J Endod. 2012 Jan;38(1):101-4.
36. Gambarini G. Influence of a novel reciprocation movement on the cyclic fatigue of twisted files (TF) instruments . Healthcare learning website. www.healthcare-learning.com London October 2012.
37. Ruddle C. Dr. Ruddle on Minimally Invasive Endodontics. Viewpoint, Oral Health Dental Journal, May 2014. 10-11.
38. Bey G. A Complicated Endodontic Retreatment Using A New Cordless Obturation System: A Case Report. Oral Health Dental Journal, May 2015, 16-26.
39. Gergi RM , Osta NE, Alfred S. Naaman AS. Dentinal crack formation during root canal preparations by the twisted file adaptive, Reciproc and WaveOne instruments. European Journal of Dentistry, Vol 9 / Issue 4 / Oct-Dec 2015, 508-512.











