
Many people experience a deep fear of sitting in the dental chair even though dentistry can significantly improve their health. By understanding a few key basics about the nervous system (and how fear, pain, and anxiety work in the body), you can help minimize pain, shut down fear responses, and decrease inflammation. This understanding can decrease the load on your staff and schedule, and help your clients leave their appointments smiling. Understanding the interaction of the trigeminal nerve with the vagus nerve and their roles in either upregulation of the nervous system (fight or flight) or relaxation and pain relief (a parasympathetic state) can help you accomplish this.
The brain can say, “Hey that’s interesting. Turn up the volume on this pain information that’s coming in”, or it can say, “Oh no – let’s turn down the volume on that and pay less attention to it,” says David Linden (a professor of neuroscience at Johns Hopkins University and author of the new book Touch: The Science of Hand, Heart, and Mind.) By mastering the interaction of the trigeminal and vagus nerves, you can mitigate pain, anxiety, fear, and inflammation. Let’s explore the interaction and role of these two powerhouse nerves to see how this can work for you.
Major Roles of the Trigeminal nerve
According to Gray’s anatomy, the trigeminal nerve is the largest cranial nerve. It carries sensory input from the face, the greater part of the scalp, the teeth, the oral and nasal cavities and is the motor supply to the masticatory and other facial muscles. It contains proprioceptive nerve fibers from the masticatory and extraocular muscles and contains connections to the vagus nerve through the main sensory nucleus in which the vagus nerve may be influenced by masticatory reflexes. 3 The trigeminal nerve plays a major role in the sympathetic state of the nervous system.
It is the link between the trigeminal nerve and the vagus nerve that makes it possible to enhance either feelings of anger, fear, anxiety, pain (increasing inflammation) or the sense of well-being and peace that your patient experiences in association with their visit to your office. The complex interaction between the vagus and trigeminal nerves is becoming clearer through recent research that has noted their connections through nerve stimulating studies related to treatment of neuropsychiatric disorders. 12
Major Roles of the Vagus nerve
The vagus nerve is responsible for various tasks, including: heart rate, GI function, sweat, and many muscle movements in the mouth, as well as speech (via the recurrent laryngeal branch of the vagus nerve). It also innervates the inner canal portion of the outer ear and part of the meninges. 2
When the vagus nerve is functioning properly, the gag reflex is diminished, the stomach is calm, heart rate is slow, and breathing is normal. Stress can cause the vagus nerve to operate poorly and may even cause a person to faint when faced with extreme distress.

The vagus nerve plays a major role in decreasing inflammation and monitoring/regulating heart functions. As mentioned previously, it assists in lowering the heart rate. The right-side vagus innervates the sinoatrial node. Neuroscientist Otto Loewi first demonstrated that nerves secrete neurotransmitters, which have effects on receptors in target tissues. Loewi electrically stimulated the vagus nerve of a frog heart, causing the heart rate to slow. Then he took the fluid from the heart and transferred it to a second frog heart, one which had the vagus nerve removed. The second heart slowed down without any electrical stimulation. This shows that the vagus nerve stimulates secretion of calming neurotransmitters, a key element in calming your patients. Heart rate variability is a measure that can be used to assess autonomic (parasympathetic) activity in response to meditation or calming.
Physical and Emotional Effects
Excessive activation of the vagus nerve during emotional stress can cause vasovagal syncope due to a sudden drop in cardiac output. Vasovagal syncope affects young children and women more than other groups experiencing moments of extreme fear or stress to the nervous system.
Understanding the interaction of these two nerves can make one ask, “What if you could calm down the trigeminal nerve and enhance the functioning of the vagus nerve?” Bilateral application of vibration through these powerful cranial nerves may just hold the answer.
Part II: Science and applied vibration in TMJD
Introduction
Temporomandibular joint dysfunction (TMJD) is a disorder commonly involving pain and dysfunction in the jaw and/or muscles involved in controlling jaw movement. While the absolute numbers of those affected by TMJD is unknown and while published studies differ on the prevalence of TMJD based on population, age, and country or origin demographics, the disorder tends to be more common in women than men. Studies report at least twice the prevalence in women than men for various factors including: pain, joint sounds, opening difficulty and bruxism. 6
Background
The National Institute of Dental and Craniofacial Research (NIDCR), one of the National Institutes of Health (NIH), has stated that pain is a major disorder of TMJD. Current and ongoing research regarding pain being conducted under the NIH umbrella include: understanding the nature of facial pain in TMJ disorders and what it may hold in common with other pain conditions, such as headache and widespread muscle pain, pinpointing factors that lead to chronic or persistent jaw joint and muscle pain, exploring differences between men and women in how they respond to pain and to pain medications, examining the effects of stressors, such as noise, cold and physical stress, on pain symptoms in patients with TMJ disorders to learn how lifestyle adjustments can decrease pain, identifying medications, or combinations of medications and conservative treatments, that will provide effective chronic pain relief: and investigating possible links between osteoarthritis and a history of orofacial pain (https://www.nidcr.nih.gov/oralhealth/Topics/TMJ/TMJDisorders.htm).
In rehabilitation, application of heat (thermotherapy), has been known to help decrease joint stiffness, relieve muscle spasm, increase blood flow and temporarily decrease pain perception. Furthermore, a combination of heat, laser therapy and pulsed magnetic therapy has been reported to help decrease pain associated with TMJD. 8 More recently, the use of vibration has been reported to be helpful in reducing perceived pain and is suggested to decrease pain for dental nerve blocks9 or local anesthesia injections for cosmetic surgery. 11 Although published literature relating to vibration use for treatment of TMJD is extremely limited, a study looking at the use of a vibratory stimulation-based occlusal splint was reported to alleviate painful symptoms related to TMJD following a 15-day management period. 4
Position 1

Position 2

Position 3

The effect of vibration on the mechanics of pain is most commonly described using a modified Melzack and Wall gate theory. The use of vibration will stimulate receptors at the point of localized vibration application. The stimulation of peripheral receptors then sends signals back to the spinal cord and releases neurotransmitters. Thus, the release of pain neurotransmitters inhibits neural pain signaling. While the actual mechanism for pain reduction at the spinal cord level versus higher level (central or cortical) remains unclear and debated, recent research has pointed more towards central or higher level interactions (think vagus nerve) for pain suppression. 5 While much more research is needed, recent research in rats has demonstrated that mechanical stimulation of HT7 (an acupuncture point) at a frequency of 85 Hz for 60 sec was sufficient to reduce cocaine-induced locomotor activity in dependent rats. 7 This frequency has been shown to suppress neuron firing activity. Whether or not this has a potential tie into pain management and pain medicine addiction has yet to be seen, but early data appears promising.
Vibration works within a particular amplitude (measured in mm) and frequency (measured in Hz). Vibration appears to inhibit activation of antagonist muscles. 1 As more studies have looked at effects of vibration application, the vibration stimulus has been found to reduce H-reflex activity within the muscle for a period of five to 10 minutes. 10 The use of localized vibration can also help to alleviate muscle stiffness and has been used adjunctively as a form of “massage”, although with a greater amount of sensory stimulation based on the frequency of vibration.
Although the measures of pain and stiffness have been limited to visual analog scales (VAS) or pressure point threshold (PPT) testing (which rely heavily on the individual’s subjective rating), the use of localized vibration appeared to influence the state of both muscle and neural input. Recently, shear wave elastography (SWE) (a form of ultrasound testing) has emerged as a potential objective method to monitor “stiffness” or “strain” responses of soft tissues and is being used to detect a variety of medical issues. A recent study reported that SWE is useful to quantify masseter muscle stiffness by showing that SWE was able to detect approximately a two-fold greater increase in masseter stiffness in two separate groups of females with TMJD as compared to those in a healthy control group. 13
An investigative university study recently sought to determine if the use of localized vibration would alter masseter muscle stiffness in females without diagnosed TMJD. Their hypothesis was that localized vibration would induce a neuromechanical response that would be evidenced in muscle stiffness of the masseter. They used 12 female subjects (21 +/- 1.8. years) without any history of TMJ disorder under both control (vibration turned off) and vibration conditions on two different days. Subjects underwent a relaxation period in a reclined seated position before having the baseline masseter SWE measures taken with the jaw in a relaxed position. An ultrasound machine with a probe was used under the elastography setting. SWE values were calculated within the muscle borders of the captured image. Multiple images were assessed and averaged for the calculation of the baseline SWE measure in kilopascals (kPa). Subjects then underwent localized vibration treatment using a Rezzimax® handheld vibration module (see www.rezzimax.com) with a two-pronged bilateral contact extension (Tuner). All Subjects underwent two sixty-second rounds of vibration at three of the targeted points suggested by the creators of the Tuner: supraorbital margin of both eyes (70 Hz), medial and lateral sides of the base of the neck (105 Hz), and inside the mouth at a point just in front of the bilateral mandibular ramus (105 Hz).
SWE. Pre-vibration Baseline Measure

Post-vibration Measure
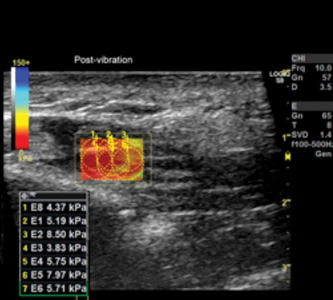
Post-measures of SWE followed the same protocol as the baseline measures, and the “Control” condition group utilized the same Rezzimax® Tuner but without the vibration turned on. [Statistical analysis of the results showed no significant difference in Baseline Control vs Post Control measurements (p = .180) or Baseline Control and Baseline Vibration (p=.984). However, Baseline Vibration vs Post vibration was significant (p=.000). With the Post-measures following vibration treatment decreasing by almost 50% when compared to no vibration or the pre-treatment means.]
The researchers summarized that localized vibration to these three spots resulted in acute reductions in masseter stiffness as measured by SWE in normal individuals. Use of localized vibration may be beneficial in reducing tension/stiffness of the masseter muscle in those with chronic TMJ disorder; however, future studies are needed to determine if the stiffness due to the disorder would respond differently and if stiffness changes translate into pain reduction. The researchers are currently looking to assess the amount of vibration transmission that occurs to the jaw when undergoing these localized vibration treatments to quantify the amount and pattern of vibration transmission.
Part III: Using Calibrated Resonance on Bilateral Pressure Points in Practice
Unilateral vibration applied to an area of pain appears to calm the pain. This concept of bilateral application of resonance (carefully calibrated vibration) to key points in the head and face may have an even stronger and longer lasting benefit through the interaction of the cranial nerves, especially the trigeminal and vagus nerves with their strong role in the central nervous system. As a physical therapist, the primary author has been using the bilateral application of vibration on key cranial nerves to calm down pain and improve functioning for clients in acute and chronic distress from craniofacial pain for several years. We know the patient experience can be greatly enhanced with improved pain control. We conclude this article with excerpts from the experiences of a dentist that has successfully implemented the use of the concepts described in this article to help his clients in chronic and acute pain.
“I have used the Rezzimax® Tuner in my office now for approximately a year. I have found it to be a nice adjunct to what I was already doing in relieving craniofacial pain, and primary headaches in addition to other disorders of the face, jaw and neck. I found that when patients use the device correctly they get good results and pain resolutions. Much of it is palliative and first line, which I believe has decreased the need for pain relievers generally used for relief. I like to use the Tuner with patients when they present with what is expected to be a more refractory case. It allows us to calibrate them in office on the proper use of the device so that they can get the most benefit when they are away from the office. I have found the device useful for myofascial pain syndrome, localized myalgia, tension type headaches and migraines and as a catalyst to improve autonomic tone. I like the dual nature of the design and the concept of bilateral activation of afferent fibers to block c fiber transmissions. This is a very viable way to relax the central nervous system. I plan to continue using this modality in office and prescribing its use outside the office for my craniofacial pain patients,” says Michael Bennett, DDS, who is one of hundreds of dentists who have added in the Rezzimax® vibration techniques into practice since the FDA registered device was invented nearly two years ago. OH
Oral Health welcomes this original article.
References
- Cardinale, M, Bosco, C. The use of vibration as an exercise intervention. Exerc Sport Sci Rev 31: 3-7, 2003.
- Eljamel, S. Problem based neurosurgery: World Scientific Publishing Company; 2011
- H, G. Gray’s anatomy. In. London: Churchill Livingston; 1989
- Hara, ES, Witzel, AL, de Luca, CE, Ballester, RY, Kuboki, T, Bolzan, MC. A novel vibratory stimulation-based occlusal splint for alleviation of TMD painful symptoms: a pilot study. J Oral Rehabil 40: 179-184, 2013.
- Hollins, M, McDermott, K, Harper, D. How does vibration reduce pain? Perception 43: 70-84, 2014.
- Johansson, A, Unell, L, Carlsson, GE, Soderfeldt, B, Halling, A. Gender difference in symptoms related to temporomandibular disorders in a population of 50-year-old subjects. J Orofac Pain 17: 29-35, 2003.
- Kim, SA, Lee, BH, Bae, JH, Kim, KJ, Steffensen, SC, Ryu, YH, Leem, JW, Yang, CH, Kim, HY. Peripheral afferent mechanisms underlying acupuncture inhibition of cocaine behavioral effects in rats. PLoS One 8: e81018, 2013.
- Navratil, L, Navratil, V, Hajkova, S, Hlinakova, P, Dostalova, T, Vranova, J. Comprehensive treatment of temporomandibular joint disorders. Cranio 32: 24-30, 2014.
- Pedersen, C, Miller, M, Xu, KT, Carrasco, L, Smith, C, Richman, PB. Use of a Dental Vibration Tool to Reduce Pain From Digital Blocks: A Randomized Controlled Trial. Reg Anesth Pain Med 42: 458-461, 2017.
- Ritzmann, R, Kramer, A, Gollhofer, A, Taube, W. The effect of whole body vibration on the H-reflex, the stretch reflex, and the short-latency response during hopping. Scand J Med Sci Sports 23: 331-339, 2013.
- Sharma, P, Czyz, CN, Wulc, AE. Investigating the efficacy of vibration anesthesia to reduce pain from cosmetic botulinum toxin injections. Aesthet Surg J 31: 966-971, 2011.
- Shiozawa, P, Silva, ME, Carvalho, TC, Cordeiro, Q, Brunoni, AR, Fregni, F. Transcutaneous vagus and trigeminal nerve stimulation for neuropsychiatric disorders: a systematic review. Arq Neuropsiquiatr 72: 542-547, 2014.
- Takashima, M, Arai, Y, Kawamura, A, Hayashi, T, Takagi, R. Quantitative evaluation of masseter muscle stiffness in patients with temporomandibular disorders using shear wave elastography. J Prosthodont Res 61: 432-438, 2017.
About the Authors
 Sharik is the CEO of Rezzimax, LLC. He received his bachelor’s degree in physical therapy from the University of Utah and his master’s degree in counseling from Utah State University. He is passionate about pain relief and determining how the nervous system works, and humanitarian work to relieve suffering. You can reach Sharik at sharik@rezzimax.com or www.rezzimax.com
Sharik is the CEO of Rezzimax, LLC. He received his bachelor’s degree in physical therapy from the University of Utah and his master’s degree in counseling from Utah State University. He is passionate about pain relief and determining how the nervous system works, and humanitarian work to relieve suffering. You can reach Sharik at sharik@rezzimax.com or www.rezzimax.com

J. Brent Feland is an Associate Professor at Brigham Young University in the Department of Exercise Sciences. He has been researching the effects of vibration and vibration training on performance, rehabilitation, and neuromechanics for the past 15 years. You can reach Brent at brentfeland@gmail.com
![]()
Michael Bennett, DDS is board certified by the American Board of Craniofacial Pain and the American Board of Craniofacial Dental Sleep Medicine. He limits his Orem Utah practice to helping people with TMD, craniofacial pain, and sleep-disordered breathing. You can reach Mike at dentaldocmike@gmail.com










