
“I always do the best for the patient”. That is noble, we’ve all said it and absolutely should practice that way. However, our ability to deliver on this is often limited by many factors including patient desires, ability to afford treatment, and practice limitations. It’s very rare that a patient comes into the office wanting only the absolute best care possible regardless of what it costs. It’s much more common for a patient to say “do whatever my insurance will pay for”.
From a practice management point of view, doing excellent work doesn’t always have to be the most expensive. If fact, with the proliferation of fee cutting insurances, corporate dentistry, increased competition, and managed care, being prudent with office expenditures is more important than ever and perhaps more of a determinant on materials and procedures than ever before. When we can provide excellent service for less cost, that can be a win-win for both the office and the patient.
With indirect restorations, we strive for aesthetic, comfortable, and durable consistency. If the goal was to truly do “the best” work possible in every case, we could always hire one of the cosmetic guru ceramists who charge more nearly $1000 (USD) per unit. There are certain cases where that expertise is worth every penny; but not always. What are we willing to pay per unit and what is our (and the patients) return on that investment? When is “good enough” good enough?
Trendy Indirect Materials
There are generally three materials that dominate crown and bridge materials today; lithium disilicate, anterior zirconia, posterior zirconia. They all have an excellent record of clinical success and can meet the esthetic demands of many clinical situations with or without layering porcelain and customization.
For conservative restorations like veneers, where most, if not all, of the adhesion is to enamel, a silica-based ceramic like lithium disilicate is hard to beat. Plus, when bonded to etched enamel with a bonding agent and composite luting material, the longevity is undeniably excellent. Monolithic lithium disilicate has a flexural strength of 360-400 MPa which is quite good with an excellent history of service if the preparation and cementation are sufficient whether in the anterior or posterior.
Zirconia has become the market leader in volume because, simply put, it works well. Anterior (high translucency) zirconia has less flexural strength (750-850 MPa) than its older, more opaque posterior zirconia cousin (1050-1300 MPa) and can often give a more natural vitality because of this. There is now even a choice to have both the more translucent anterior and more strength posterior zirconia blended in one restoration (e.max ZirCAD Prime (Ivoclar) resulting in arguably the best esthetics ever in a non-layered restoration.
To Layer or Not to Layer
Certainly, all three of these materials can be customized with layering when the situation demands a higher cosmetic standard. In the hands of the right ceramist the beauty and realism can be incredible. So, for those premium cases, a great ceramist and layered restoration can be the ultimate in aesthetics. But there is a significant expense.
The two main reasons NOT to layer are strength and cost. No doubt that cutting back and adding characterization porcelain can add beauty, depth, and realism, but may not be as durable as a monolithic one. The flexural strength of the add on materials is weaker than the substructure, generally 150-200 MPa, which is the “weak link” compared to the stronger, non-layered material and more likely to chip or break. With that in mind, even in anterior cases, a non-layered lithium disilicate or anterior zirconia restoration may at times be “best”.
So, some of you reading this will say, “I never compromise and only do the best”. No one can argue with that. Many of us though, practice in an environment where fees and overhead are a concern and we don’t have an unlimited amount to spend on “the absolute best” (whatever that means). The best blend of value, aesthetics, and function depends of course the unique view of each practitioner and with the ongoing development of stronger, more aesthetic materials, that view keeps changing. It hasn’t been that long since we were doing platinum dies and 100% water-powder hand stacked feldspathic porcelain for our high-end cases.
Generally speaking, the lab fees for a non-layered restoration is considerably less than one with cut back, layering, and customization. That is fair. With less expenditure of time and often without the help of a certified ceramist, a lab has less investment in time and labor with a monolithic restoration. Particularly with digital impressions and model-less restorations, the fabrication cost per unit is reduced and turnaround time often faster. That is often “good enough”.
Monolithic Anterior Zirconia Case
In this case, the patient had interproximal decay, failing restorations, irritated gingiva, uneven color, and a worn dentition (Figs. 1-3). I forgot to mention that she had a limited budget. She wanted to have her smile improved but her insurance lowered the fee to $739 (USD). Despite wanting to do “the best”, budget and reality made us head towards “good enough” (Figs. 4 & 5).
Fig. 1

Fig. 2

Fig. 3

Fig. 4

Fig. 5

Teeth were prepped, decay removed, build ups done, and impressions taken. Teeth were cleaned with 2% chlorhexidine (Cavity Cleanser, Bisco) and temporaries placed in the shade closest to what the patient chose for the final restorations (ProV Temp, Bisco). All records were sent to the lab with a complete set of pre-op and procedure photos. After one-week in temporaries the patient returned for a follow up to evaluate color, length, and experience with the temps (Fig. 7). Polishing was done, photos taken, and desired changes communicated with the lab (Fig. 8).
Fig. 6

Fig. 7

Fig. 8

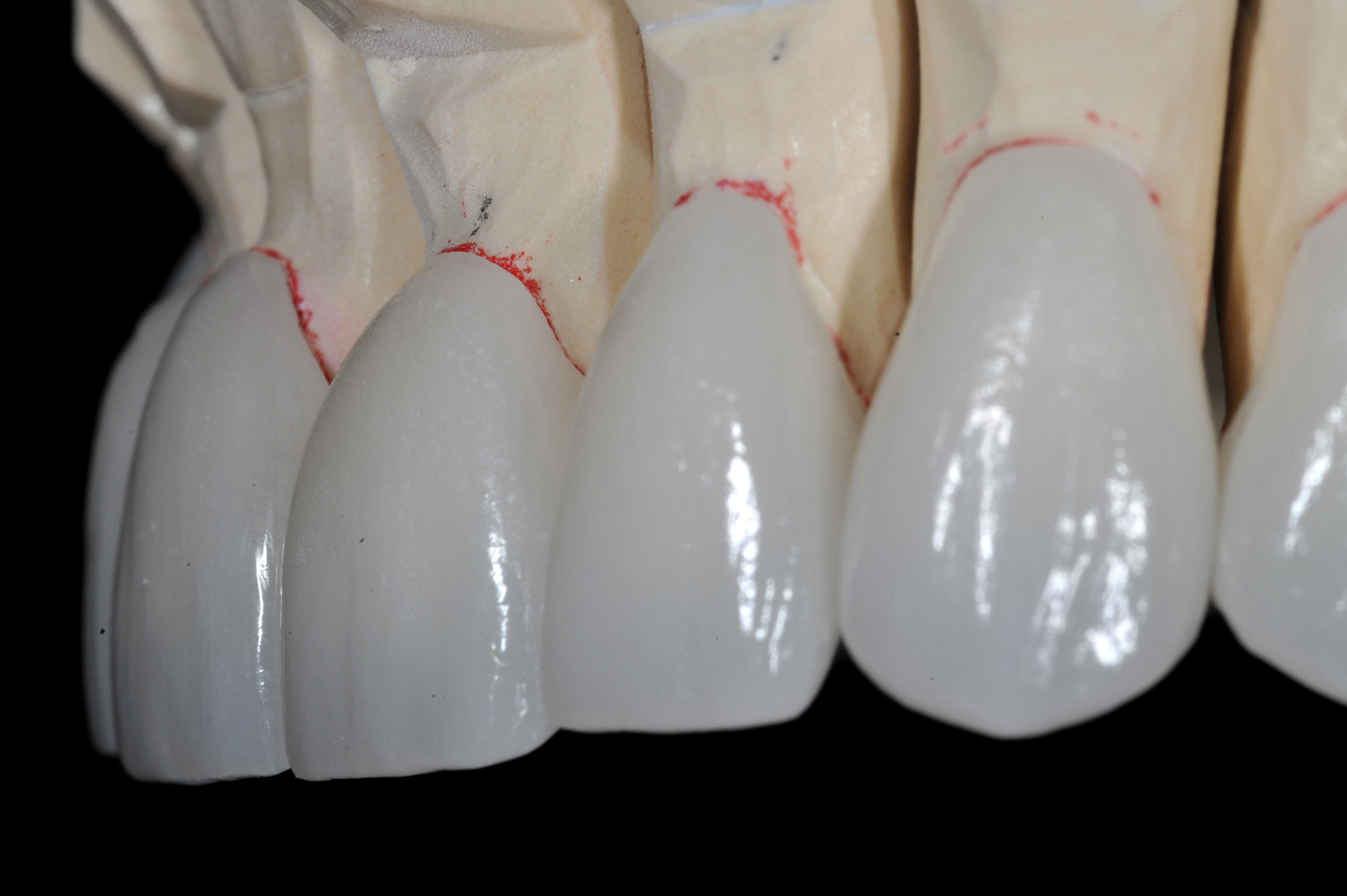
The preps were conservative but done in full coverage to cover old restorations, decay, and missing enamel (Fig. 9). To best meet the needs of the patient within the financial constraints, we asked the lab to use monolithic “anterior zirconia” full coverage restorations in shade 0.5M1 as the patient chose (Fig. 10). The anterior zirconia, without layering porcelain, is opaque enough to cover the color of the model underneath but transparent enough to maintain vitality (Fig. 11). The lab put facial anatomy and slight character stain in the glaze for an excellent aesthetic result (Fig. 12).
Fig. 9

Fig. 10

Fig. 11
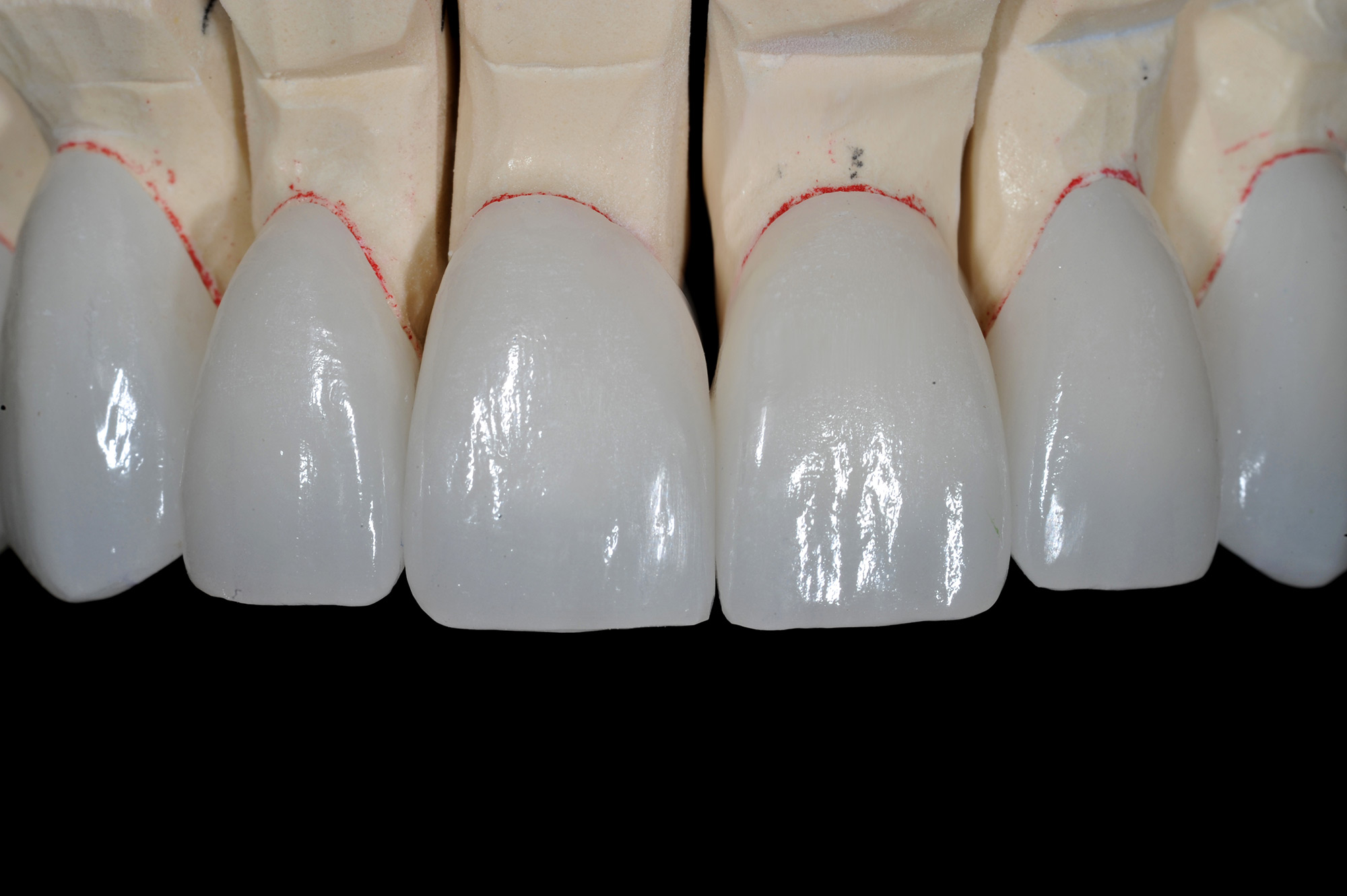
Fig. 12
Bio-interactive Cementation
At the insertion appointment, the temps were removed, restorations tried in, a cleaner applied (ZirClean, Bisco), rinsed, and dried (Fig. 13). Anterior zirconia has the strength to be cemented with almost any material but our preference is to use a regenerative, bio-interactive, self-adhesive, dual cure cement because of its excellent tissue response (TheraCem, Bisco) (Fig. 14). The teeth were isolated, cleaned again with 2% chlorhexidine, and restorations placed two at a time starting with the central incisors and working posteriorly (Figs. 15-16).
Fig. 13

Fig. 14

Fig. 15

Fig. 16

We allow the chemical cure to begin first without light curing and start clean up after initial set by pushing up down at each papilla, going around the margins with a CH3 explorer, and removing the semi-set material in several large pieces (Fig. 17). This easy to clean up cement is light cured only after complete clean up including flossing. Not also the transparency of the anterior zirconia when the curing light is applied (Fig. 18).
Fig. 17

Fig. 18

Critique
The soft tissue response is good (Fig. 19). The noted translucency of these monolithic restorations is good even with this light shade with a slight influence of the preparations underneath in the gingival 2/3 of each one (Fig. 20). To be critical and honest, the upper left cupid, which was necrotic with a metal post, could have been more opaque or I could have done better hiding the grayness with a more opaque build-up, replacement of the post, or a less translucent restorative material.
Fig. 19

Fig. 20

The value of monolithic restorations can be excellent depending upon the clinical situation and patient circumstances (Figs 21-23). I certainly could have ordered a cut back and several different character layering ceramics added. That certainly creates more of a “wow” effect for us dentists to look in the journals, but we’ve all probably had patients who weren’t as excited about the incisal translucency and tertiary anatomy as we were.
Fig. 21

Fig. 22

Fig. 23

When the restoration provides patient pleasing service for many years, it is always “good enough”.
Oral Health welcomes this original article.
About the Author
 Dr. Griffin is a full-time practitioner and has owned multiple practices in the St. Louis area for 30 years. He has earned Diplomate status with the American Board of Aesthetic Dentistry, Accreditation in the American Academy of Cosmetic Dentistry, Masters in the Academy of General Dentistry, and Diplomat International Academy for Dento-Facial Esthetics. He has had the honour of being published many times, contributed to product review and development, is a member of the highly respected Catapult Group of instructors, and is a clinical director for the Pacific Aesthetic Continuum.
Dr. Griffin is a full-time practitioner and has owned multiple practices in the St. Louis area for 30 years. He has earned Diplomate status with the American Board of Aesthetic Dentistry, Accreditation in the American Academy of Cosmetic Dentistry, Masters in the Academy of General Dentistry, and Diplomat International Academy for Dento-Facial Esthetics. He has had the honour of being published many times, contributed to product review and development, is a member of the highly respected Catapult Group of instructors, and is a clinical director for the Pacific Aesthetic Continuum.
RELATED ARTICLE: Low Tech Approach – High Five Results! The Beauty Of The Direct Composite Mock-Up










