
Introduction
Over the past 40 years, dental ceramics have evolved dramatically. Ceramics are defined as non-metallic, inorganic materials manufactured by heating crystals at high temperatures. They are widely used for dental prosthetic treatments because their high resistance to compression and abrasion allows them to mimic the function of the teeth, while resisting both wear and fracture from the forces that occur during mastication. Additionally, the color stability and color versatility of ceramics allow for restorations that maintain esthetics over a long functional lifetime.1,2,3
The increased use of ceramics in dentistry has inspired research and development resulting in a range of products with varied properties such as different translucency and bending stiffness. Dental porcelains can be classified by chemical composition, fusion temperature, or manufacturing technique.
In the 18th century, the Italian dentist Giuseppangelo Fonzi, looked for the most efficient method for manufacturing porcelain crowns that were resistant to torque and lever forces, retentive and esthetic, and did not lose their shape or dimension in the heat of the ceramic oven. Over time, increasingly more effective manufacturing techniques were established.1,3
Dental ceramic manufacturing techniques are classified into two categories: manual techniques, requiring the manual skills and critical eye of a dental technician, and digital techniques, still requiring the critical eye of a dental technician but replacing the manual work with a digital milling machine (Fig 1).
Fig. 1

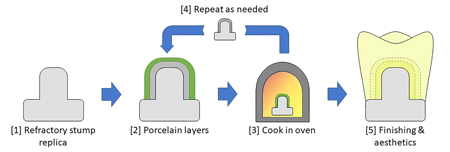
One common manual manufacturing technique is known as the “ceramic build-up”. The technique consists of directly applying porcelain layers onto a refractory material stump. The refractory stump with porcelain layers is inserted into an oven to bake the porcelain, and the layering process is repeated until the ideal dimensions, characteristics, and
esthetics of the prosthetic restoration are completed (Fig 2).1,3,4
Fig. 2
Porcelain injection, also known as the “hot-press” technique, is another manual manufacturing technique. The hot-press technique requires creating a wax pattern of the finished crown, which is then invested (surrounded and filled) with refractory material. The refractory is then heated to burn out the wax pattern. Then, the fluid porcelain is injected into the resulting refractory cavity under pressure. Once cooled, the porcelain is removed from the refractory mold, resulting in an accurate ceramic reproduction of the wax pattern (Fig 3).1,3,4
Fig. 3

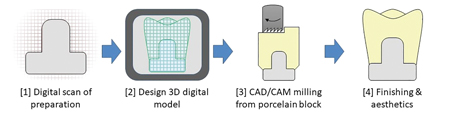
Digital techniques utilize CAD/CAM fabrication systems. The first step is a digital three-dimensional scan of the patient’s intraoral preparation or a model thereof. The technician designs the desired prosthetic on this model with the CAD software program. The finished design file is sent to the CAM machine which mills the crown from a prefabricated porcelain block. A more recently developed technique utilizes 3D printing to produce the prosthetic from the design file (Fig 4).1,3,4
Fig. 4
The next step is to compare the different crown fabrication techniques to determine which is better. A widely adopted metric to assess crown quality is to measure the marginal gap between the tooth preparation and the prosthetic restoration. There is a direct relationship between the marginal discrepancy of a fixed restoration and its longevity.5,6 In 1989, Dr. Robert Holmes recognized the importance of standardizing the terminology and reference points for measurements of marginal discrepancy to facilitate accurate measurements and comparisons, and to homogenize knowledge among health professionals. Over time, his definitions have been adopted by the dental research community.6
Marginal discrepancy is defined as the distance between the termination of the tooth preparation and the marginal termination of the prosthetic restoration6 (Fig 5). According to the Guide to Dental Materials and Devices of the American Dental Association (ADA), the marginal discrepancy of a restoration must be less than 120 µm.7 If the marginal discrepancy is greater, it can cause detrimental consequences for the health of support tissues, periodontal tissues and the remaining dental structures of the abutment tooth.
Fig. 5

Discussion
PubMed was searched for scientific papers on the marginal gaps of porcelain crowns manufactured using various techniques. The initial search returned 233 results and was refined to 7 publications by accepting only articles that (1) were published within the last 3 years, (2) analyzed the marginal gaps of full ceramic crowns, and (3) used proven or conventional processing techniques.
Two 2019 studies (Cunali8 and Meirowitz5) found that the marginal gaps of pure porcelain crowns manufactured with CAD/CAM systems were within the ADA specifications (53-78 µm).
Elrashid, in 2019, compared the average marginal discrepancy of a group of porcelain crowns manufactured with CAD/CAM (27 µm) to a group manufactured with hot-press injection (39 µm), and found that both techniques were within ADA specifications, but the CAD/CAM system produced a smaller marginal gap (p<0.001)9. Similarly, in 2018, Riccitello10 compared CAD/CAM to hot-press, also finding that both techniques resulted in a marginal gap within ADA specifications; the CAD/CAM technique again produced a smaller marginal gap than the hot-press technique (p<0.05).
In 2019, Dolev11 compared the marginal gaps of crowns fabricated by the hot-press technique (90 µm) and CAD/CAM (87 µm), observing marginal gaps within ADA guidelines, with no significant difference between the fabrication methods (p>0.05).
Finally, in 2018, Azar12 compared CAD/CAM to hot-press injection, finding that marginal discrepancies of crowns produced with these techniques were within ADA limits. However, this study found that the hot-press technique had a significantly smaller marginal discrepancy (38 µm vs. 45 µm, p=0.006). A systematic review carried out in the same year by Papadiochou13 came to the same conclusion and indicated that most crowns manufactured by the hot-press technique had equal or smaller marginal gaps than those made with CAD/CAM systems.
Results
This literature overview indicates that currently there is no scientific consensus as to whether manual or digital techniques result in better marginal gaps for ceramic prosthetics. Results in the surveyed articles varied in both direction and magnitude.
All articles agreed, however, that both porcelain injection and CAD/CAM techniques produced full ceramic crowns with marginal gaps well within ADA standards.
The survey did not identify recent articles which measured the marginal discrepancy of crowns produced with the manual build-up technique.
Conclusions
It is very important for practitioners to deliver the most favorable results, both short and long term. Knowing the best techniques for optimizing marginal gaps helps dental professionals produce long lasting prosthetics by providing the necessary marginal fit that will promote support tissue health and protect the remaining dental structures of the prepared tooth.
At present, there does not seem to be a significant difference in the marginal gaps of full ceramic crowns that is specifically dependent on the various manufacturing techniques examined. The latest literature provides no consensus about which manufacturing system results in smaller marginal gaps. It is essential that new ceramics and new crown fabrication techniques continue to be analyzed for their compatibility with dental restorative health.
Oral Health welcomes this original article.
References
- Nevarez A. Características de los Materiales Cerámicos Empleados en la Práctica Odontológica Actual. ADM. 2012;69(4):157-163.
- Jorquera G, Merino N, Walls S, Mahn E, Fernandez E. Simplified Classification for Dental Ceramics. J. Dent. Sci. Ther. 2016;1(2):22-25.
- Hammerle C, et al. Dental Ceramics: Essential Aspects for Clinical Practice. Zurich: Quintessence Books; 2008.
- Martínez F, Pradíes RG, Suárez MJ, Rivera B. Cerámicas Dentales: Clasificación y Criterios de Selección. RCOE. 2007;12(4):253-263.
- Meirowitz A, Bitterman Y, Levy S, Mijiritsky E, Dolev E. An in Vitro Evaluation of Marginal Fit Zirconia Crowns Fabricated by a CAD-CAM Dental Laboratory and a Milling Center. BMC Oral Health. 2019;19(1):103.
- Holmes JR, Bayne SC, Holland GA, Sulik WD. Considerations in Measurement of Marginal Fit. J Prosthet Dent 1989;62(4):405-408.
- American Dental Association. Guide to Dental Materials and Devices. 5th ed. Chicago: ADA; 1970. ANSI/ADA Specification No. 8 for Zinc Phosphate Cement; p.87–88.
- Cunali RS, Saab RC, Correr GM, Cunha LF, Ornaghi BP, et al. Marginal and Internal Adaptation of Zirconia Crowns: A Comparative Study of Assessment Methods. Braz Dent J. 2017;28(4):467-473.
- Elrashid AH, AlKahtani AH, Alqahtani SJ, Alajmi NB, Alsultan FH. Stereomicroscopic Evaluation of Marginal Fit of E.Max Press and E.Max Computer-Aided Design and Computer-Assisted Manufacturing Lithium Disilicate Ceramic Crowns: An In vitro Study. J Int Soc Prev Community Dent. 2019;9(2):178–184.
- Riccitiello F, Amato M, Leone R, Spagnuolo G, Sorrentino R. In vitro Evaluation of the Marginal Fit and Internal Adaptation of Zirconia and Lithium Disilicate Single Crowns: Micro-CT Comparison Between Different Manufacturing Procedures. Open Dent J. 2018;12:160–172.
- Dolev E, et al. Comparison of Marginal Fit Between CAD-CAM and Hot-Press Lithium Disilicate Crowns. Journal of Prosthetic Dentistry. 2018;121(1):124-128.
- Azar B, Eckert S, Kunkela J, Ingr T, Mounajjed R. The Marginal Fit of Lithium Disilicate Crowns: Press vs. CAD/CAM. Braz. oral res. 2018;32:e001.
- Papadiochou S, Pissiotis A. Marginal Adaptation and CAD-CAM Technology: A Systematic Review of Restorative Material and Fabrication Techniques. JPD. 2018;119(4):545-551.
About the Author
 Fernanda Zegarra graduates from the DDS program at UPC in Lima, Peru in the summer of 2020. Her family has been in the dental profession for 65 years. She is a third-generation dentist and the first female dentist in her family. Her interests include prosthodontics, evidence-based dentistry, and the practical application of modern research and technology to the dental practice.
Fernanda Zegarra graduates from the DDS program at UPC in Lima, Peru in the summer of 2020. Her family has been in the dental profession for 65 years. She is a third-generation dentist and the first female dentist in her family. Her interests include prosthodontics, evidence-based dentistry, and the practical application of modern research and technology to the dental practice.
To see more articles from the July/August 2020 issue, please click here!










