The introduction of minimally invasive dentistry (MID) has revolutionized the management of dental caries by emphasizing the preservation of sound dental tissue capable of remineralization.1-3 This philosophy forms the foundation of chemo-mechanical caries removal (CMCR), which targets the selective removal of infected dentin while preserving the healthy, potentially remineralizable tissue.4 CMCR is a pain-free, conservative approach that avoids the use of drills and anesthesia, making it particularly suitable for children and anxious or medically compromised patients.5 Practitioners may decide to apply the CMCR technique to their general patient populations as well, given CMCR’s clinical and cost (materials, time and stress) benefits.
CMCR techniques involve applying chemical agents that soften carious dentin, allowing it to be removed with hand instruments. Early examples include Caridex (1986) and Carisolv (1998)6, both utilizing sodium hypochlorite. However, limitations such as high cost, longer treatment times, unpleasant taste, and the need for specialized instruments hindered their widespread adoption.
To address these drawbacks, Papacárie Duo (Oral Science, Brossard QC) was developed in Brazil in 2003. This gel-based CMCR agent combines papain (a proteolytic enzyme derived from papaya), chloramine (a disinfectant),7 and toluidine blue (a photosensitive antibacterial dye).8 (Fig. 1) Papain exhibits selective action by targeting only necrotic tissue due to the absence of plasma antiprotease in infected areas, sparing healthy tissue. Chloramine enhances disinfection, while toluidine blue binds to bacterial membranes, increasing antimicrobial efficacy. The gel is cost-effective, easy to use, and does not require specialized tools, making it a popular choice in pediatric and preventive dentistry.
Fig. 1

Papacárie Duo (Fig. 2) is a papain-based gel composed of a proteolytic enzyme that interacts with the partially degraded collagen present in the necrotic carious tissue.2 The mechanism of action involves breaking down peptide bonds in degraded collagen, facilitating the removal of infected dentin without harming sound tissue.9 Papacárie Duo also has antimicrobial properties.10-12 Preliminary findings suggest that Papacárie Duo is safe and effective, aligning the protocol with MID principles.13
Fig. 2
Studies comparing Papacárie Duo with traditional mechanical excavation methods using scanning electron microscopy (SEM) have shown that Papacárie Duo is effective in removing infected dentin in primary molars.14 Furthermore, it reduces the need for anesthesia and is associated with better patient comfort and acceptance.15-23
The evolutionary shift towards conservative and patient-friendly dental care has propelled the development and usage of CMCR agents such as Papacárie Duo. These methods offer effective alternatives to conventional drilling by selectively removing only irreversibly damaged dentin, minimizing pain and preserving tooth structure. Dental caries remain a major concern of the dental profession. Decay is globally prevalent, particularly in children, youth, young adults and the elderly. Fortunately, CMCR offers a safe, economical, and minimally invasive approach aligned with the modern goals of preventive and conservative dentistry. Despite the success of CMCR techniques in reducing bacterial load and preserving pulp vitality, their adoption still faces challenges such as clinician training and awareness. Ongoing research into innovative applications continues to assess the efficacy, safety, and biological impact of these agents, ensuring their optimal integration into routine dental practice.
Chemistry and method of action
The chemo-mechanical caries removal technique has generated great interest among dental professionals due to the concept of saving unaffected tooth structure while guaranteeing the removal of the denatured collagen stage of carious dentine. Although the two layers of infected and affected dentin can be differentiated by fuchsin staining, the removal of infected dentin is operator and technique sensitive and does not present a practical clinical solution.
It is important to note that many caries detector dyes and other traditional methods often fall short in distinguishing between infected and affected dentin, particularly in deep cavities or at the amelo-dentinal junction. CMCR methods such as Papacárie Duo address this limitation by using natural chemical agents to soften and dissolve only the decayed tissue, allowing for less invasive removal compared to traditional drilling.
Papacárie Duo is comprised of a medicinal ingredient, Papain (Carica papaya fruit 6000 FCC papain units) and non-medicinal ingredients, Polyethylene Glycol and Ammonium Chloride. Papacárie Duo is especially advantageous in selective caries removal due to papain, an enzyme extracted from papaya and similar to pepsin. Papain breaks down only infected tissue because healthy tissues contain α1-antitrypsin, which inhibits papain’s proteolytic action. Since infected dentin lacks this inhibitor, the papain effectively digests the partially degraded molecules that are more easily broken down while leaving healthy structures intact. (Fig. 3)
Fig. 3
Clinical assessment and protocol
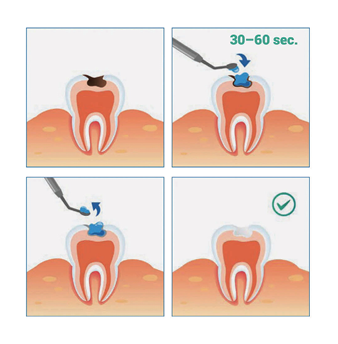
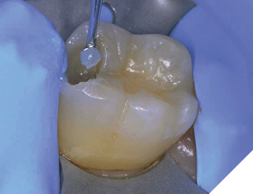
Prior to any caries removal procedure, the clinician must perform a clinical assessment, with or without radiographic evaluation. While a radiographic assessment is highly preferable, it is not always possible with young children and severely dental-phobic patients. Dental prophylaxis with pumice and water are used to remove the oral debris and dental surface films. The carious site is isolated as effectively as possible with rubber dam where feasible (Fig. 4). A single drop of the Papacárie Duo gel is applied to the carious tissue (Fig. 5) and allowed to stay in place for 30-60 seconds (Fig. 6). The surface is tapped manually to determine if the carious dentin is soft enough to be gently scooped out. The infected dentin is then removed by scraping the surface and gently scooping out the damaged tissue with blunt hand excavators (Fig. 7).
Fig. 4
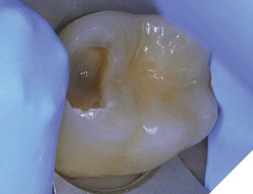
Fig. 5
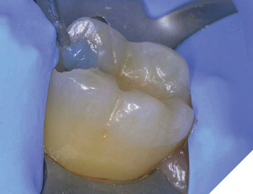
Fig. 6
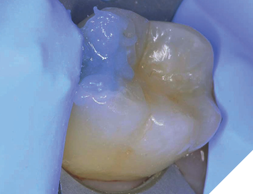
Fig. 7
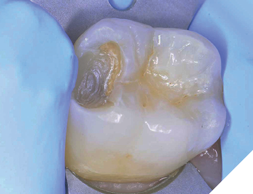
The process is repeated until there are no signs of softened tissue remaining or no further dentin shavings are present (Fig. 8). Reapplication can be done immediately if needed with no need to rinse or dry in between steps.
Fig. 8
Another case demonstrates the ease and practicality of anxiety and timesaving CMCR. The caries are readily identified and the access is direct, requiring only cotton roll isolation (Fig. 9). After simple prophylaxis, the Papacárie Duo is applied, one drop per cavity (Fig.10). The demineralized dentin is excavated without the need for anesthetic while relieving the patient of dental anxiety, leaving a hard, shiny, restorable surface (Fig.11). The cavities have been atraumatically restored in a relaxed environment (Fig. 12).
Fig. 9
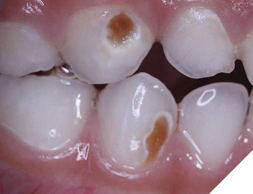
Fig. 10
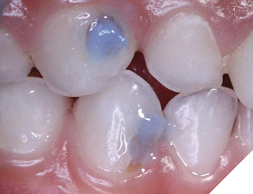
Fig. 11
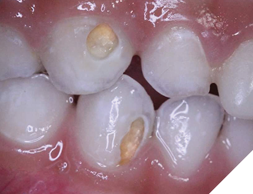
Fig. 12

Efficacy of caries removal
The completeness of caries removal is judged by visual (absence of any discoloration) and tactile (smooth passage of the explorer and absence of a catch or a tug-back sensation) methods.23,24
Bacteria are the primary cause of dental caries, making it essential to eliminate as many as possible during the removal of decayed tissue. In this study, caries removal followed the manufacturer’s guidelines, stopping once the gel turned clear (indicating a non-turbid state). Papacárie Duo excavation led to a highly significant reduction in all tested viable bacteria.8
In addition to papain, Papacárie Duo contains chloramines, which help to chemically soften carious dentin. Chloramines disrupt hydrogen bonding by altering the secondary or quaternary structure of collagen, thereby facilitating the removal of decayed tissue.9 Notably, Papacárie Duo does not affect the intact collagen fibers found in the inner affected or healthy dentin, as papain selectively reduces only necrotic tissue. Supporting this, El-Tekeya et al. reported that Papacárie Duo is significantly more effective than Carisolv in reducing residual cariogenic bacteria in the dentin of primary teeth.25
The removal of dental caries with rotary instruments often causes heat and pressure on the pulp, leading to pain. Additionally, drilling can result in the unnecessary loss of healthy tooth structure surrounding the decayed area.23,26,27 On the other hand, there was no significant difference in the presence of remaining bacterial colonies following caries removal using either Papacárie Duo or conventional drilling techniques. This suggests that Papacárie Duo may serve as a viable alternative to traditional methods, especially for highly active or anxious pediatric patients.14
Costs and benefits of chemo-mechanical caries removal
Anxiety related to dental treatment is often triggered by the use of anesthesia and drilling, both of which are highly stressful for patients. Anxiety costs the practice time and money (as well as stress). Therefore, non-traumatic treatment methods are essential to prevent fear and lack of cooperation, particularly during dental procedures.15 The chemo-mechanical method for caries removal was developed to address these concerns by providing a more comfortable experience and reducing stress, especially in children. This approach helps minimize clinical complications and contributes to adults maintaining a positive attitude toward dental care.28 Despite advancements in dental techniques, many patients—and the parents of young patients—continue to experience high levels of anxiety. Fear is a natural response that significantly impacts patient behavior and cooperation, making pediatric dental care particularly challenging for professionals.29
A Brazilian study demonstrated that the chemical-mechanical method using Papacárie Duo gel was significantly more cost-effective than the traditional drill-based technique, offering a significant reduction in cost per procedure. Cost analysis of materials used in each dental restorative procedure was conducted for both carious tissue removal methods. The calculation focused solely on the specific materials required for each technique, excluding those commonly used in both. The use of Papacárie Duo gel resulted in a 42% cost reduction compared to the traditional drilling method.30 In other words, the cost restoring a cavity prepared with Papacárie Duo gel was 58% cheaper than the cost of a traditional procedure (drilling) using local anesthesia.
Papacárie Duo proved to be an excellent, minimally invasive alternative for removing carious tissue in children, with comparable effectiveness to conventional methods. Given its cost savings and non-traumatic approach, Papacárie Duo presents an interesting option for much-needed dental services, particularly in isolated communities and undertreated populations where treatment delivery must be simplified and economical.30
Conclusion
The Papacárie Duo method is a safe, minimally invasive, and effective technique for caries removal, particularly suitable for pediatric patients. Its selectivity in targeting only infected tissue, antimicrobial properties, and pain-free application make it an excellent alternative to conventional mechanical methods. It preserves healthy tooth structure and reduces patient discomfort, which is critical in modern conservative dentistry. Papacárie Duo also offers a promising solution for public healthcare, particularly in communities with limited access to dental services and high rates of tooth decay. Its application can improve pediatric dental care while helping to alleviate the financial strain on public health systems. 
Oral Health welcomes this original article.
Key questions and answers
1. What is chemo‑mechanical caries removal?
Chemo‑mechanical caries removal (CMCR) is a minimally invasive technique that uses a chemical agent to soften decayed tooth tissue, allowing it to be gently scraped away without drilling or anesthesia. It preserves healthy dentin and reduces patient discomfort.
2. How does Papacárie Duo work to remove tooth decay?
Papacárie Duo is a gel that contains papain, a natural enzyme with antibacterial and anti-inflammatory properties. When applied to a carious lesion, it selectively breaks down infected, softened dentin while leaving healthy tissue intact, allowing for gentle manual removal.
3. What are the steps involved in chemo‑mechanical caries removal?
First, Papacárie Duo gel is applied to the decayed area. After allowing time for the gel to act, the softened carious dentin is gently removed using a blunt hand instrument. The process is repeated as needed until all decay is eliminated, followed by restorative treatment.
4. Can chemo‑mechanical methods help anxious or medically compromised patients?
Yes, CMCR is especially beneficial for anxious, pediatric, or medically compromised patients. Because it avoids the noise, vibration, and pressure of traditional drilling—and often eliminates the need for anesthesia—it significantly reduces stress and discomfort during treatment.
References
- Balciuniene I, Sabalaite R, Juskiene I. Chemomechanical caries removal for children. Stomatologija 2005;7:40-44.
- Bussadori SK, Castro LC, Galvao AC. Papain gel: a new chemo-mechanical caries removal agent. J Clin Pediatr Dent 2005;30:115-119.
- Mickenautsch S, Yengopal V, Banerjee A. Atraumatic restorative treatment versus amalgam restoration longevity: a systematic review. Clin Oral Investig 2010;14:233-240.
- Mathre S, Kumar S, Sinha S, Ahmed BMN. Chemo-Mechanical Method of Caries Removal: A Brief Review. IJCDS 2011;2:52-57.
- Bussadori SK, de Godoy CHL, Alfaya TA, Fernandes KPS, Mesquita-Ferrari RA, Motta LJ. Chemo-Mechanical Caries Removal with Papacarietm: Case Series with 84 Reports and 12 Months of Follow-up. J Contemp Dent Pract 2014;15(2):250-253.
- Freedman G. Polymer Preparation Persuades Patients: Dental Town 2003: May 4:5 22–25
- Jawa D, Singh S, Somani R, Jaidka S, Sirkar K, Jaidka R. Comparative evaluation of the efficacy of chemomechanical caries removal agent (Papacarie) and conventional method of caries removal: an in vitro study. J Indian Soc Pedod Prev Dent 2010;28:73-77.
- Bussadori SK, Castro LC, Galvão AC. Papain gel: A new chemo-mechanical caries removal agent. J Clin Pediatr Dent 2005;30:115-9.
- Sahana S, Vasa AA, Geddam D, Reddy VK, Nalluri S, Velagapudi N. Effectiveness of chemomechanical caries removal agents Papacarie® and Carie-Care™ in primary molars: An in vitro study. J Int Soc Prevent Communit Dent 2016;6:S17-22.
- Chowdhry S, Saha S, Samadi F, Jaiswal JN, Garg A, Chowdhry P. Recent vs Conventional Methods of Caries Removal: A Comparative in vivo Study in Pediatric Patients. Int J Clin Pediatr Dent 2015;8:6-11.
- Hamama HH, Yiu CK, Burrow MF. Viability of intratubular bacteria after chemomechanical caries removal. J Endo. 2014;40:1972-1976.
- Motta LJ, Bussadori SK, Campanelli AP, Silva AL, Alfaya TA, Godoy CH, et al. Efficacy of Papacarie(R) in reduction of residual bacteria in deciduous teeth: a randomized, controlled clinical trial. Clinics 2014;69:319-322.
- Laura Alves Bastos, Francine Lorencetti Silva, Joao Pedro de Queiroz Thome, Maya Fernanda Manfrin Arnez, Lucia Helena Faccioli, Francisco Wanderley Garcia Paula-Silva. Brazilian Dental Journal (2019) 30(5): 484-490
- AlHumaid J. Efficacy and efficiency of papacarie versus conventional method in caries removal in primary teeth: An SEM study. Saudi J Med Med Sci 2019;8:41-5.
- Kotb RM, Abdella AA, El Kateb MA, Ahmed AM. Clinical evaluation of Papacarie in primary teeth. J Clin Pediatr Dent 2009;34:117-123.
- Bussadori SK, Guedes CC, Bachiega JC, Santis TO, Motta LJ. Clinical and radiographic study of chemical-mechanical removal of caries using Papacárie: 24-month follow up. J Clin Pediatr Dent 2011;35:251-4.
- Singh S, Jawa D, Jaidka S, Somani R. Comparative clinical evaluation of chemomechanical caries removal agent Papacarie® with conventional method among rural population in India – In vivo study. Braz J Oral Sci 2011;10:193-98.
- Bittencourt ST, Pereira JR, Rosa AW, Oliveira KS, Ghizoni JS, Oliveira MT. Mineral content removal after Papacarie application in primary teeth: A quantitative analysis. J Clin Pediatr Dent 2010;34:229-31.
- Banerjee A, Kidd EA, Watson TF. Scanning electron microscopic observations of human dentine after mechanical caries excavation. J Dent 2000;28:179-86.
- Avinash A, Grover SD, Koul M, Nayak MT, Singhvi A, Singh RK. Comparison of mechanical and chemomechanical methods of caries removal in deciduous and permanent teeth: A SEM study. J Indian Soc Pedod Prev Dent 2012;30:115-21.
- Splieth C, Rosin M, Gellissen B. Determination of residual dentine caries after conventional mechanical and chemomechanical caries removal with Carisolv. Clin Oral Investig 2001;5:250-3.
- Yamada Y, Kimura Y, Hossain M, Kinoshita JI, Shimizu Y, Matsumoto K. Caries removal with Carisolv system: Criteria evaluation and microleakage test. J Clin Pediatr Dent 2005;30:121-6.
- Kotb RM, Elkateb MA, Ahmed AM, Kawana KY, El Meligy OA. Dentin topographic features following chemomechanical caries removal in primary teeth. J Clin Pediatr Dent 2016;40:472-9.
- Moimaz SAS, Okamura AQC, Lima DC, Saliba TA, Saliba NA. Clinical and microbiological analysis of mechanical and chemomechanical methods of caries removal in deciduous teeth. Oral Health Prev Dent 2019;17:283-288.
- El-Tekeya M, El-Habashy L, Mokhles N, El-Kimary E. Effectiveness of 2 chemomechanical caries removal methods on residual bacteria in dentin of primary teeth. Pediatr Dent 2012;34:325-30.
- Schwendicke F, Paris S, Tu YK. Effects of using different criteria for caries removal: A systematic review and network meta-analysis. J Dent 2015;43:1-5.
- Albrektsson Tomas O, Douglas B, Glantz PJ, Lindhe Jan T. Tissue Preservation in Caries Treatment. Great Britain: Quintessence Books; 2001
- Araújo, N. C., Oliveira, A. P. B., Rodrigues, V. M. S. & Andrades, P. M. M. S. Analysis of marginal microleakage in glass ionomer cement restorations after the use of Papacarie. Rev. Odonto. Ciênc. 23, 161–165 (2008).
- Massoni, A. C. L. T., Forte, F. D. S. & Sampaio, F. C. Percepção dos pais e responsáveis sobre promoção de saúde bucal. Rev. Odontol. UNESP. 34, 193–197 (2005).
- Fernanda Bottega, Sandra Kalil Bussadori, Iara Denise Endruweit Battisti, Eusélia Paveglio Vieira, Tiago Szambelan Pompeo & Eliane Roseli Winkelmann. Costs and benefits of Papacarie in pediatric dentistry: a randomized clinical trial. Scientific Reports 2018) 8:17908 | DOI:10.1038/s41598-018-36092-x
About the author

Dr. Freedman is a founder and past president, American Academy of Cosmetic Dentistry, a co-founder, Canadian Academy for Esthetic Dentistry, Regent and Fellow, International Academy for Dental Facial Esthetics, and a Diplomate and Chair of the American Board of Aesthetic Dentistry. Adjunct Professor of Dental Medicine, Western University, Pomona, California. Author of 14 textbooks and > 1000 dental articles.