
Irrigation of root canal systems is the most important aspect of RCTT 1,2,3, yet it may also be the least understood thing we do inside these complex spaces.4 Evidence for that statement is the fact that, to this day, very few endodontists understand how the introduction of rotary shaping files caused an increase in our irrigation failures,5 not to mention the facts that a large proportion of endodontists instrument with NaOCl 6,7 and still think we clean canals with files. 5,8
Does this lack of understanding about irrigation fundamentals translate into RCT failures? The answer is YES, although these cases are seldom correctly diagnosed after the fact. A randomized multi-center study done by Nixdorf et al. 9 showed that 11% of patients in pain–seen by endodontists–were not pain-free 6 months later! Half of these patients were misdiagnosed myofascial pain cases–they didn’t need RCT. The other half did need RCT, but 40% of this group received RCT on an adjacent tooth–so much for pulp testing–leaving the remaining cases that did need RCT, had the correct tooth treated, but remained symptomatic.
Virtually all of these cases had a history of severe pulpitis or partial necrosis before RCT, indicating to the authors that the most likely etiology for those teeth to continue to be symptomatic was due to pulp remnants left by the irrigation procedure; said irrigation failure rate being 3.3% of those patients presenting in pain.
11% of those in pain weren’t better six months later. Half of those–5.5% didn’t need RCT, 40% of the other half had the wrong tooth treated, leaving 60% of 5.5% which maths out at 3.3 of our cases. That’s not a small issue if you consider the fact that 25 million RCTs 10 are done in the US alone every year, revealing something like 825,000 RCT irrigation failures per year. A number that closely relates to the findings in a previous study by Nixdorf et al. on persistent tooth pain after RCT. 11
The Challenge of Irrigating Anatomic Complexities
Complete removal of pulp tissue during RCT is not a simple job due to the anatomic complexity of root canal systems and the fact that NaOCl dissolves pulp tissue in a linear fashion, not as a catalytic reaction (Fig. 2).7,8 While a broached pulp can be completely dissolved in a minute or two when dropped into a Dappen dish of bleach, it can take 40 minutes of passive positive pressure irrigation to digest the same volume of pulp tissue out of an MB canal system contained inside an upper molar. Fortunately, irrigation technology is rapidly improving our ability to eliminate lateral pulp remnants in spite of the current trend toward minimally-invasive instrumentation.
Fig. 1A: This tooth continued to refer pain (in the endodontic zone) to its owner for 18 months after RCT. Two different endodontists recommended apicoectomy to remove the overextended filling material beyond the MB and D roots. Instead the patient was told the case could be cut at any time in the future, but that surgery might be avoided by simply retreating the underfilled ML canal.

Fig. 1B: Post-op radiography revealed a mid-mesial canal with its own blood supply.

Fig. 1C: Cleared mesial root of an extracted lower molar illustrates the impossibility of cleaning this root canal system with instruments and the necessity of irrigating effectively.

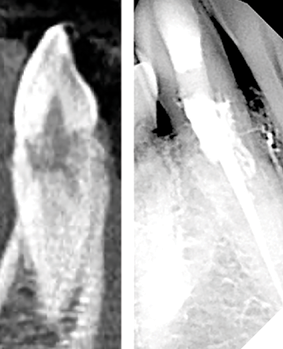
Fig. 2A: MicroCT reconstruction of an upper first molar, highlighting the complexity of the MB canal system.

Fig. 2B: By segmenting the root canal space from the root, the lateral morphology is more apparent.

Fig. 2C: Superimposition of typical MIE canal shaping reveals the very narrow interface of lateral pulp remnants exposed to irrigating solutions, requiring linear dissolution rather than circumferential dissolution.

Stojicic et al., in 2010, looked at the effects of concentration, temperature, and agitation on NaOCl efficacy and found that dissolution efficacy increased almost linearly with the concentration of NaOCl. Higher temperatures and agitation considerably enhanced the efficacy of NaOCl, although agitation had a greater effect than temperature and continuous agitation resulted in the fastest tissue dissolution. Their comment that “Optimizing the concentration, temperature, flow, and surface tension can improve the tissue dissolving effectiveness of NaOCl even 50-fold” seemed a bit far-fetched when first read,12 however, our own research (unpublished data) on the rates of pulp dissolution from isthmus spaces have confirmed that this is possible.
New Irrigation Technologies
There are many ways to intermittently agitate (cavitate) NaOCl in root canal systems; sonic, ultrasonic, and laser activation, but GentleWave® irrigation (GW), developed by Sonendo (Sonendo Inc. Laguna Hills, Ca, US), is one of the few irrigation methods that delivers continuous agitation to all canals simultaneously. They pump the irrigating fluids up to 9000 psi, and blast them into and out of the access cavity past creating a negative pressure Bernoulli effect in the RCS to prevent NaOCl from escaping into peri-radicular tissues. Much is made of the sonic energy GW imparts to the solutions, but the greatest mechanism of action is more likely the 250 ml of NaOCl shot through the tooth during the 5-minute NaOCl cycle, allowing accelerated dissolution of pulp tissue in canals (Fig. 4).13
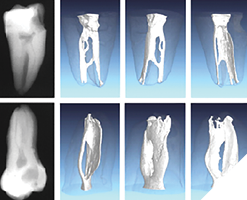
Fig. 3A: This MIE RCT was cleaned with conventional positive pressure irrigation with 6% NaOCl, delivered with a 12cc syringe and a 30 Ga. closed-end side-vented cannula. Simple, inexpensive, but uni-canular and very time dependent (20-40 mins).

Fig. 3B: The lower molar RCT was treated by Filippo Santarcangelo using EndoVac by Kerr Endodontics. This tooth was irrigated continuously for 45 minutes because he could not negotiate the last 3mm of the distal canal. Post-op radiography reveals the distal primary canal cleaned and filled 3mm beyond the apical extent of instrumentation with multiple microscopic lateral canals filled in both roots.
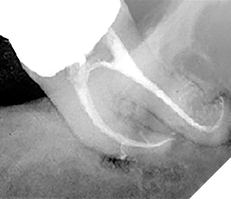
Fig. 3C: The complete healing seen at the 4-month recall is testament to the thoroughness of the irrigation. Like conventional irrigation, EndoVac is uni-canular, but completely safe due to the cannula being used for suction instead of irrigants delivery.
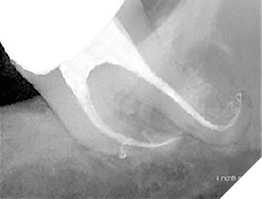
Fig. 4: Lower cuspid with extensive internal resorption treated with GentleWave® irrigation. Note the myriad of resorptive lacuna trails filled post-operatively after the vital tissue causing them was dissolved during two complete cycles of GW (Case by Buchanan).
After forty to fifty RCT procedures successfully done with GW, the senior author had his first case failure in a red-hot C-shaped lower molar that remained symptomatic after RCT was completed (Fig. 5). The case looked pretty nice when finished–several filled lateral aberrations were seen post-operatively, but the patient complained about pain that continued to be referred to his right endo zone (below the malar eminence, above the lower border of the mandible). This being a C-shaped molar, the best hypothesis for the etiology of this failure was incomplete debridement of pulp tissue in the large isthmus spaces (Fig. 6).
Fig. 5: This lower C-shaped molar presented with a severely inflamed pulp. 5B. Post-op radiographs show abrupt mesial and distal apical canal curvatures as well as significant isthmus morphology. 5C. Extending toward the centreline from MB and D primary canals. 5D. This CBCT view shows the MB canal possibly treated short of terminal length.
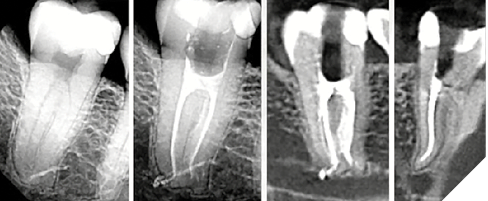
Fig. 6A: Axial CBCT views, originally published in: Fan B, Cheung GSP, Fan M, Gutmann JL, Bian Z. C-shaped canal systems In mandibular second molars: part 1- Anatomical features.
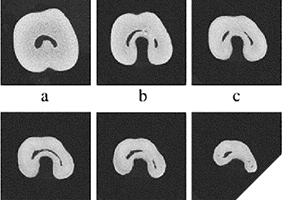
Fig. 6B: J Endod. 2004 Dec; 30(12): 899-903) and computer reconstructions. Originally published in Solomon M, Piqué F, Fan B, Eilat Y, Berman LH. The challenge of C-shaped canal systems: A comparative study of the Self-Adjusting File and ProTaper. J Endod. 2012 Feb; 38(2): 209-214) of C-shaped molars, showing isthmus spaces extending from MB to D canals. Generally impossible to instrument, some of these isthmus spaces are wider than 5mm’s presenting the ultimate challenge to any irrigation procedure.
A Novel Isthmus Replica
To test this hypothesis, a research device was designed to replicate the isthmus morphology seen in these molars. This was 3D-printed in two halves so a pulp replica (porcine muscle tissue) could be inserted into the isthmus form before they were assembled with light-cure adhesive (Fig. 7). This novel in vitro device was capable of displaying how pulp dissolution occurs in isthmus spaces when a number of variables are compared, said variables being NaOCl concentration, temperature, fluid flow, and agitation.
Fig. 7A: Isthmus research block half after printing with UV-cured clear polymer.

Fig. 7B: A cut and dyed pulp replica (prosciutto) after placement in the isthmus space.

Fig. 7C: . A second block half is bonded over this, trapping the isthmus replica inside.

Fig. 7D: Isthmus block assembled, prior to cutting pulp replica out of the two canal paths.

Fig. 7E: Isthmus block mounted in a PanaVise in front of a operating microscope connected to a digital video recorder.

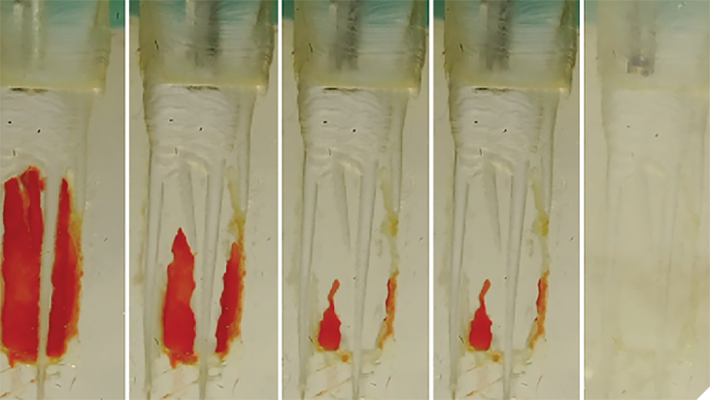
The first irrigation method tested in the isthmus block was of course GW, and it confirmed my hypothesis about the cause of my C-shaped molar failure–at the end of the 5-minute NaOCl cycle significant amounts of pulp replica remained. Also confirmed by this test was the fact that EDTA–even when activated by multi-sonic energy–has zero ability to digest organic tissue, so it could be said that GW’s primary mechanism of action (MOA) for pulp dissolution is hosing root canal systems with enormous volumes of NaOCl (Fig. 8).
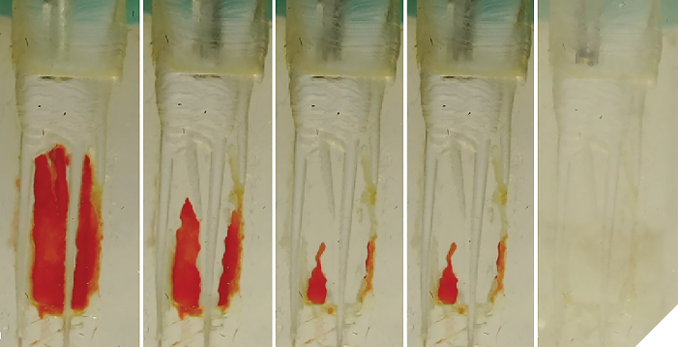
Fig. 8: 8A. Isthmus research block after the 30-second distilled water cycle–no pulp replica dissolved. 8B. The block after 2.5 minutes of the NaOCl cycle. 8C. The block after the end of the 5-minute NaOCl cycle. 8D. The block after the 2-minutes EDTA cycle. 8E. Another GW procedure instrument was installed in the console and after an additional 2.5 minutes of the NaOCl cycle all remaining tissue was gone, revealing that although GW greatly accelerates NaoCl tissue dissolution, it is still a linear process needing adequate time to do its job.comparative study of the Self-Adjusting File and ProTaper. J Endod. 2012 Feb; 38(2): 209-214) of C-shaped molars, showing isthmus spaces extending from MB to D canals. Generally impossible to instrument, some of these isthmus spaces are wider than 5mm’s presenting the ultimate challenge to any irrigation procedure.
Negative Pressure Irrigation (NPI) VS Positive Pressure Irrigation (PPI)
The isthmus research blocks were then used to investigate NPI because the literature shows excellent cleaning of isthmus spaces with EndoVac (EV) by Kerr Endodontics.14, 15, 16 Is it the direction the solutions are moving through the canal? Is it successful because EV eliminates “vapor lock”–the gas bubbles liberated during pulp saponification?17 Isthmus block studies showed the only difference between PPI and NPI was that the latter requires constant replenishing of solutions whereas dentists using PPI tend to irrigate and let the solutions soak in the patient’s tooth–radically decreasing the volume of solutions run through root canals. When constant irrigation was used for both NPI and PPI the results were identical (Fig. 9).
Fig. 9: Isthmus research blocks showing no difference between PPI and NPI when constant irrigation was done (Buchanan).

Therefore, while EV is 100% safe from irrigation accidents,18,19 it was poorly designed and was pedantic to use because of the constant attention needed and because of its propensity to clog up every 5 minutes of use. Worse than that, EV is uni-canular, meaning it only irrigates a single canal at a time so a four-canal molar requires 20 minutes of intensive hands-on work.
Investigating Closed-System Negative Pressure Irrigation (CSNPI)
Eliminating intensive hands-on requirements was simple in a closed system as the solutions could then be pulled into the pulp chamber by the vacuum coming through the micro-cannulas from the chairside evac system (Fig. 10). The results from the extracted tooth experiment (Fig. 11) as seen in SEM imaging were exceptional but it took 30 minutes due to the repeated clogging of the microcannula.
Fig. 10A: Illustration of experimental closed system EV. The irrigating canula is the vacuum source pulling the NaOCl from an IV bag through an inlet sealed into the access cavity.
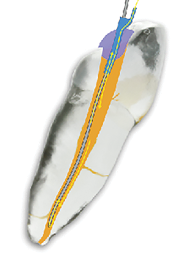
Fig. 10B: This was run for 30 minutes, unclogging the cannula every 5 minutes.

Fig. 10C: The ultimate objective for this irrigating system was to have manifolds and cannulae for each canal so multi-canalar irrigation can happen. Originally the vacuum was connected to the cannula and the irrigants inlet was placed just inside the of the access cavity.
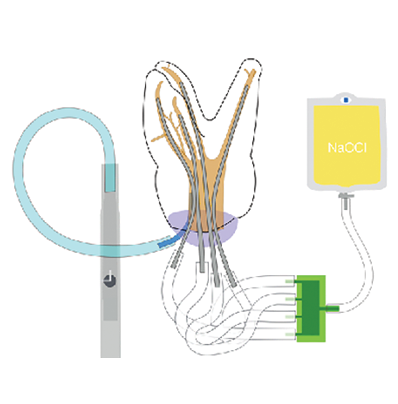
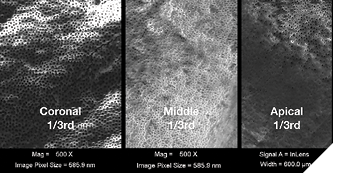
Fig. 11: SEM imaging of root canal walls in the coronal, middle, and apical thirds (from the experimental tooth in Fig. 10) showing exceptional cleaning results (Buchanan).
The Reversal
The senior author then had the epiphany that clogging would never be an issue if the direction of vacuum were reversed, so that change was made and another isthmus block study was kicked off. Shortly after beginning, it became apparent that not only was the cannula blockage issue solved, but that the vacuum-drawn outflow of NaOCl through the end of the blunt-cut cannula was dissolving pulp replica at a remarkable rate (Fig.12), most likely due to the constant, rapid fluid flow of sodium hypochlorite exiting the cannula ends.
Fig. 12: The isthmus block result after just 13 minutes when the vacuum was reversed to prevent cannula blockage, and found that the constant vacuum-drawn outflow through the end of the cannula radically increased dissolution speed.

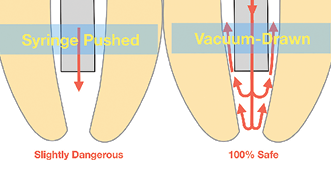
There was initial concern about the inherent safety of NaOCl flowing out of an open-ended cannula, until it was realized that vacuum-drawn irrigation immediately ceased the moment an open-ended needle was locked in a canal, rendering it impossible to cause a hypochlorite accident with this MOA (Fig. 13).
Fig. 13: Illustration showing the safety difference between NaOCl being pushed out the end of an irrigating cannula by a syringe (the reason to only use closed-end side-vented irrigating cannulas for PPI) and NaOCl being drawn out by resident vacuum pressures. Vacuum-drawn irrigant flow ceases the moment a cannula binds circumferential canal walls.
The Forward Effect
Then, as the studies continued, it became apparent that drawing the NaOCl out the end of the cannula with vacuum pressure was having its effect at least 5mm forward of the cannula end. This was very providential as it meant that irrigating cannulae had only to be placed to mid-root in most canals, a definite advantage when dealing with severely curved canals, especially when cutting minimally-invasive canal preparations.20 EV, by comparison, requires a .35mm 4 % apical preparation diameter, 21 a shaping objective that invites apical damage in curved canals.5
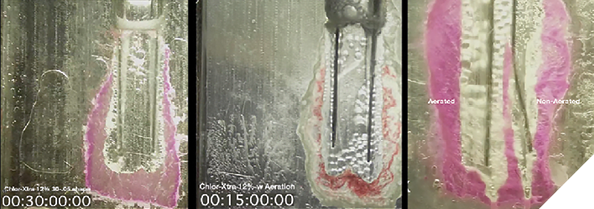
Over the following months the isthmus research block was used to compare the effects of different irrigation variables. Simply choosing a higher NaOCl concentration (Fig. 10) has significant effects on the speed of dissolution (Fig. 14). Raising the irrigants temperature from 70°F (21,1°C) to 100°F (37,7°C) increased the speed of dissolution by 33% (Fig. 15), and the shear forces of agitation–provided in this case by aerating the solution to cause gas bubble cavitation–DOUBLED the speed of dissolution (Fig. 16), confirming Stojicic et al. findings12 that agitation brought more effect than temperature. All irrigation tests were done with a constant flow of solutions–another variable critical to GW’s MOA.
Fig. 14: This isthmus block shows the Forward Effect that occurs because NaOCl is being drawn straight out the end of the blunt-cut cannula. EV only irrigates to the depth the micro-cannula fits in the canal, requiring a larger apical shape.
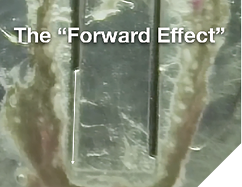
Fig. 14ABC: Isthmus research blocks displaying increases in dissolution time with increases in NaOCl concentration.
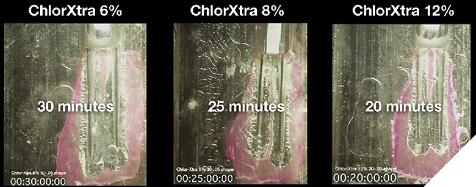
Fig. 15AB: Isthmus research blocks showing a 33% increase in speed of dissolution when the temperature of the solution was raised from room temperature to body temperature.
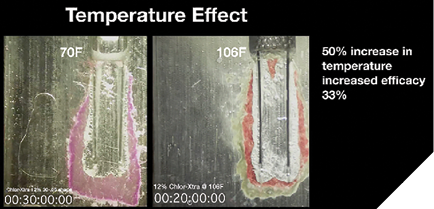
Fig. 16ABC: 16AB. Isthmus research blocks showed a dramatic 100% increase in effect when NaOCl was aerated vs non-aerated. 16C. The replica canal on the left was irrigated with aerated NaOCl, the canal on the right with non-aerated NaOCl.
Finally, a study was done with 12% NaOCl irrigant that was aerated and heated to 120° F (48,9°C) and the isthmus pulp replica was gone in just over 7 minutes (Fig. 17).
Fig. 17ABC: Isthmus research blocks showing the isthmus pulp replica completely dissolved in 7 minutes with higher NaOCl concentrations, temperatures, and continuous agitation from aeration bubbles.
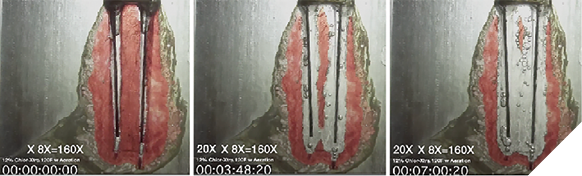
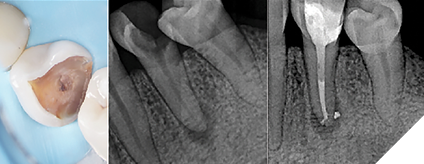
Fig. 18ABC: 18A. Closed-System Negative Pressure Irrigation device staged on a lower molar (PulpSucker by PlanB Dental). 18B. Post-op radiograph showing a 7mm long mid-mesial canal that was never touched with a file but was cleaned of vital tissue. 18C. Close-up shows an apical delta system of lateral canals in the apical third of the distal canal.
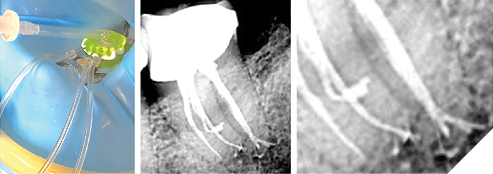
Fig. 19ABCDE: 19A. Recent clinical case that presented with severe irreversible pulpitis. 19B. Cone fit radiograph, after PulpSucker irrigation in a single-visit procedure, showing perfect cone fit in the mesial canals, but inadequate cone fitting in the very complex distal canal. 19C. Multiple impediments at the end of the virtually non-instrumented distal canal were the ideal indication for carrier-based obturation. 19D. Post-obturation image shows a loop off the distal canal that is hidden in all the other radiographs. 19E. A post-operative radiograph showing the independent MIE access entries for mesial and distal canals and the multiplicity of lateral canals in both roots.
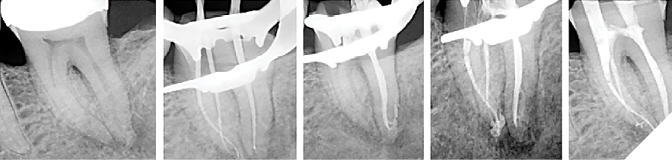
Fig. 20ABC: 20AB. Pre-op. situation showing sever broken down lower left premolar with a partial necrosis of the pulp. 20C. Post-op. image showing complete obturation of the apical pulp space and delta after PulpSucker irrigation in a single-visit treatment. Immediate placement of a fibrepost was done for future indirect restoration.
Features, Advantages, and Benefits of CSNPI
Closed-system negative pressure irrigation (CSNPI) has several advantages over conventional open-system irrigation (PPI or NPI):
1. CSNPI can be multi-cannular. Multi-cannular means that it can clean all of the canals in a given tooth at the same time. Only laser-driven PIPS (photo-induced photo-acoustic streaming), GentleWave, and PulpSucker irrigation can do this. Why is this important? Because endodontists treat mostly multi-cannular molars, so any irrigation method that is uni-cannular is a non-optimal time-suck.
2. CSNPI is more effective than open system irrigation. Open-system NPI can have constant irrigation flow but only in a single canal at a time, so even though EV ads say they can reduce a 40 minute irrigation time to 5 minutes, clinicians have to hang onto an EV syringe for 20 minutes in a 4-canal molar. That is just untenable for specialists doing 4-8 cases a day.
3. CSNPI can be hands-free. CSNPI can do its work without dentist or assistant in the operatory. GentleWave irrigation is fast, but operators must hold onto the GW procedure instrument in a very focussed manner for 8 minutes after the preparatory 3-5 minutes of hands-on work. PulpSucker irrigation can be staged in less than 5 minutes, after which it is entirely hands-off.
4. CSNPI decreases immediate post-op systems. All pain of endodontic origin is a pressure phenomena (think about it…it’s true). “Hot teeth” are exquisitely tender to touch because of the peri-radicular tissue pressure induced by severe inflammation. Closed-system irrigation applies vacuum pressures to the RCS but also to PA tissues beyond the root, and although evidenced-based clinical trials have not been completed yet, clinical experiences indicate that patients who had RCT with CSNPI experience much less post-op pain when the anesthesia wears off than patients who had RCT in teeth irrigated conventionally.
Key Points
- To avoid complications or failures of treated endodontic cases, It is important to understand that mechanical/rotary instruments do not clean canals. They are merely an aid for better irrigation of the complex root canal system.
- NaOCl is still the irrigant of choice
- Irrigation can only come from coronal directions. Although NaOCl is capable of dissolving organic tissue in under 2 minutes in a dappen dish, the complexity of the root canal system prevents this rapid break down. Further developments in irrigation technology are trying to improve this obstacle.
- The efficacy of tissue dissolution can be enhanced by concentration, temperature and agitation of NaOCl. A higher or constant volume/time will give the best results.
- The reader should be able to distinguish between the mechanism of action, benefits, drawbacks and safety issues of Positive Pressure Irrigation (PPI), Negative Pressure Irrigation (NPI), Closed System Negative Pressure Irrigation (CSNPI) and Multisonic Ultracleaning Systems (MUS).
- Understanding the concept and advantages of ‘ The Forward effect’ caused by the vacuum on multi-cannular drawn NaOCl-irrigation in MIE preparations.
Reprinted with permission from Endodontic Practice US (endopracticeus.com)
Disclosure: Dr. L. Stephen Buchanan is a co-founder of PlanB Dental.
References
- Gu LS, Kim JR, Choi KK, Pashley DH, Tay FR. Review of contemporary irritant agitation techniques and devices. J Endod. 2009; 35: 791-804.
- Liu H, Shen Y, Haapasalo M. Effectiveness of six irrigation techniques with sodium hypochlorite in tissue dissolution. Cureus 2023 May; 15(5): e39208. DOI 10.7759/cureus.39208.
- Gulabivala K, Y-L Ng, Gilberts M, Eames I. The fluid mechanics of root canal irrigation. Physiol. Meas. 2010; 31: R49-R84
- Boutsioukis C, Arias-Moliz MT. Present status and future directions – irrigants and irrigation methods. Int Endod J 2022; 55 (supply. 3): 588-612.
- Buchanan LS, Verbanck CLM. Root canal shaping in the age of minimally invasive endodontics (MIE). Endod. Practice US 2023; 16(1): 24-27.
- McComb D, Smith DC. A preliminary scanning electron microscopic study of root canals after Endodontic procedures. J Endod. 1975; 1(7) 238-242.
- Zehnder M. Root Canal Irrigants. J Endod. 2006 May; 32(5): 389-398.
- Peters OA. Current challenges and concepts in the preparation of root canal systems: a review. J endod. 2004; 30: 559-567.
- Nixdorf DR, Law AS, John MT, Sobieh RM, Kohli R, Nguyen RHN. Differential diagnoses for persistent pain after root canal treatment: A study in the national dental practice-based research network. J Endod 2015 Apr; 41(4): 457-463.
- AAE Root canal safety talking points
- Nixdorf DR, Moana-Filho EJ, Law AS, McGuire LA, Hodges JS, John MT. Frequency of persistent tooth pain following root canal therapy: a systematic review and meta-analysis. J Endod 2010 Feb; 36(2): 224-230.
- Stojicic S, Zivkovic S, Qian W, Zhang H, Haapasalo M. Tissue dissolution by sodium hypochlorite: Effect of concentration, Temperature, Agitation, and surfactant. J Endod 2010 Sep; 36(9): 1558-1562.
- Haapasalo M, Wang Z, Shen Y, Curtis A, Patel P, Khakpour M. Tissue dissolution by a novel multisonic ultracleaning system and sodium hypochlorite. J Endod. 2014 Aug; 40(8): 1178-1181.
- Versiani MA, Alves FRF, Andrade-Junuior CV, Marceliano-Alves MF, Provenzano JC, Rôças IN, Sousa-Neto MD, Siquera Jr. JF. Micro-CT evaluation of the efficacy of hard-tissue removal from the root canal and isthmus area by positive and negative pressure irrigation systems. Int Endod J 2016 Nov; 49(11): 1079-1087.
- Yoo Y-J, Lee WC, Kim H-C, Shon W-J, Baek S-H. Multivariate analysis of the cleaning efficacy of different final irrigation techniques in the canal and isthmus of mandibular posterior teeth. Restor Dent Endod 2013 Aug; 38(3): 154-159.
- Siu C, Baumgartner JC. Comparison of the debridement efficacy of the EndoVac irrigation system and conventional needle root canal irrigation in vivo. J Endod 2010 Nov; 36(11): 1782-1785.
- Estrela C, Estrela CRA, Barbin EL, Spanó JCE, Marchesan MA, Pécora JD. Mechanism of action of sodium hypochlorite. Braz Dent J. 2002; 13(2): 113-117.
- Desai P, Van Himel. Comparative safety of various intracranial irrigation systems. J Endod. 2009 Apr; 35(4): 545-549.
- Azim AA, Aksel H, Jefferson MM, Huang GT-J. Clin Oral Invest 2018 Mar;22(2):1055-1061.
- Buchanan LS. Closed-system negative pressure irrigation: A serious inflection point in root canal cleaning. Dentistry Today 2020, Apr; Published on-line.
- Kerr Endodontics. EndoVac Apical Negative Pressure Irrigation System Instructions for use.
About the Authors

Dr. Stephen Buchanan currently serves as a part-time faculty member in the endodontic departments at the University of the Pacific’s Arthur Dugoni School of Dentistry and the University of California at Los Angeles. He also maintains a private practice limited to Endodontics in Santa Barbara, California.

Dr. Christophe Verbanck has worked in several multidisciplinary and endodontic referral practices all over Flanders. In January 2016, he and his wife started their own referral practice for Endodontics, Lovendo, in Lovendegem (Belgium). He regularly teaches endodontics to general dentists and holds workshops on the application of endodontic techniques.










