
Errors accumulate during procedures. That’s the reason botching the access at the start of an RCT is so much more devastating than say, problems that come from misfitting a gutta percha cone just before finishing the case. Miss a canal and the case is going down regardless of how brilliant the remaining procedure is carried out. Perforate the tooth and suddenly titanium starts looking better. Cut huge access cavities and expect to see relatively huge numbers of root-fractured teeth within five years of treatment. Simply cheat the access procedure by beginning the instrumentation of canals before a straight, perfectly smooth path has been cut to each canal orifice and be punished every time a file, an irrigating needle, an explorer, a gutta perch point, a paper point, or a plugger is taken into each of the canals scores of times.
This is not a critique so much as an admission of the ways that teeth and their root canal systems have taught me – usually the hard way – to spend whatever time is needed to create perfect entry paths into canals before I attempt to work in them. So why do I have to have a talk with myself before beginning every access cavity – even after doing this for 35 years – to be certain to hit the mark I know must be met before it is safe to venture further?
Zen and the Art of Endo Access
In his book, Zen and the Art of Motorcycle Maintenance 1, Robert Persig described being deeply frustrated when a bolt stripped as he was attempting to remove the side covers to the engine of his motorcycle, prior to rebuilding it. The rebuild could not continue until he was able to circumvent this problem, he had expected to spend several days completing the mission, yet he was amazed at the fury he experienced when faced with this conundrum. The more he thought about it, the more mystified he became about his instinctual response, until he realized that he was tweaked because he had grossly undervalued this part of the long rebuild procedure, thinking mostly about the more dramatic routines to follow such as cracking the cylinder case, honing the cylinder, replacing the piston, and putting it all back together afterwards. When he realized that NOTHING was going to progress until he had successfully removed the side cover, he made removing that side cover a separate and important mission, an accomplishment that would deliver satisfaction in and of itself, if it could be completed during the next several hours spent. Then, he was having fun again.
So it is with endo. When we realize how critical the quality of our access preparations is to the remainder of the case, it feels like fingernails on a chalkboard to head into a canal before securing an ideal path into it. Aristotle got it right, excellence is a habit, not a character trait, so what do the habits of access excellence look like in this 21st century?
Failing to Plan is Planning to Fail
Atul Gawande, in his book The Checklist Manifesto 2, describes the importance of planning not just which procedure to do, but how every single aspect of that procedure must be planned in detail from start to finish if consistently ideal results are the goal. Does the pre-operative imaging accurately describe the anatomical challenges, does the clinician have adequate magnification and light, are the cutting tools adequate and well chosen, are the locations, angles, and depths of entry determined before beginning the procedure, have maximal safe cutting lengths been marked on access burs, are there procedures in place to deal with calcified canals that defy location, and so on. In other words, the Alfred E. Neumann attitude of, “what, me worry?” is not appropriate during this critical event. Conversely, when each of these critical elements is included in the treatment planning and execution of an ideal access cavity preparation, the rest of the procedure becomes progressively simpler as the finish is approached.
Radiographic Imaging
We wouldn’t even attempt RCT without Roentgen’s invention of the dental radiograph, so it’s not much of a stretch to claim the critical necessity of ideal pre-operative radiography. Ideal preoperative X-ray imaging must include a straight-on angle that splits the mesial and distal contacts perfectly – taken either as a periapical or as a bitewing X-ray image, then at least one ideal off-angle view in order to capture data from the Z-plane (bucco-lingual) of the tooth in question.
In my practice, a mesial off-angle view of anteriors and premolars works well because it is much easier to capture than a distal angle and in anteriors and premolars the mesial view reveals as much radicular anatomy as a distal view. In molars it is different, in molars a distal view is far preferable to a mesial off-angle view, as the mesial view superimposes the body of both roots over the distally-curved root structure, while the distal view casts the apical root end sideways where it can be more easily seen on the radiographic image.
Of course Cone Beam CT (CBCT) imaging is the unfair endodontic imaging advantage. If told I could have either a microscope or a CT machine, but not both, I would choose 3D imaging every time. Only CBCT imaging can capture the mesial view of root structure – the view in which we see “The Secret Life of Root Canals”– the bucco-lingual plane containing the greatest degree of anatomic complexity. One of the greatest joys of having a CT machine in practice is knowing, for sure, before the access procedure is begun, that there is only a single canal in the mesiobuccal root of an upper molar. Conversely, one of the few negative experiences to be had with this technology is when the reconstructed volume shows two or three canals in a root that has given up only one to the clinician’s exhaustive search.
The first gift of CBCT imaging to the field of endodontics has been the gift of finding all canals in a given tooth. Its second gift is the great diminution of access size possible because the access cavity is no longer the primary viewing port into the pulp chamber and beyond – in fact, CT imaging is the ONLY view needed into the anatomic verities of root canal spaces, allowing access cavities to be used exclusively as treatment, rather than as exploratory portals. Ultimately, RCT access procedures will be done with dynamic CT-guidance, allowing molars to be treated through three to four 1 mm pea-holes, rather than the 2-4 mm access cavities used today. 3
Outline Form
So, what are the objectives we consider when planning the invasion of a root canal space? Basically, all the best access cavities are cut in a precise balance between conservation and convenience form. We cut as little tooth structure as possible while ensuring ideal pathways into each canal. Access outline form objectives become fairly simple then; we demand convenience form otherwise we cannot complete our task, yet we strive at all times to preserve the structural integrity of the tooth. This boils down to three easily remembered objectives:
1. In anteriors and premolars, conservation form is found in the mesial-to-distal dimension. Traditionally, anterior access cavity outline form has been triangular because of the mesial and distal pulp horns in these teeth – logical until we consider the structural consequences, a needless weakening of coronal tooth structure to insure these lateral pulp horns are cleaned out, when the smallest undercut with a #2 Mueller Bur or Buc-1 ultrasonic tip (Spartan) could suffice as well. Premolars have pulp chambers like the shape of a hand which is fortunately arranged in a bucco-lingual direction – the angle of the recommended slot-like access cavity outline form is bucco-lingual as well, simultaneously combining convenience conservation form.
In anterior teeth, convenience form is harder won as the incisal edge is to be avoided out of respect for post-endodontic esthetic objectives, thus requiring a deeper cut under the cingulum to allow a more straight-line entry path while minding the “no-fly zone” of the incisal edge. The most dangerous anterior access cavity error is not cutting adequately through what Dr. Schilder called the “lingual dentinal triangle” under the cingulum and this can be accomplished with minimal structural weakening when the mesio-distal dimension is kept to 1-1.5 mm width (Fig. 1).
2. In posterior teeth – premolars and molars – it is important to remember that their occlusal surfaces are not centered over the root structure, but are skewed towards the idling cusp side of the root structure. As pulp chambers are centered in the root structure, not centered under the occlusal surface, access in posterior teeth is best accomplished by cutting near working cusps while staying 1-2 mm away from idling cusps (Fig. 2).
3. In molars conservation form is held by avoiding the distal half of the occlusal plane, as ideal file paths from the distal canals of upper and lower molars are canted severely to the mesial – so much so that distal canals of lower molars are best referenced to MB or ML cusp tips and disto-buccal canals of upper molars are best referenced to palatal cusp tips. Convenience form is achieved by cutting the mesial wall of molar access cavities parallel to the mesial surface of the tooth (Fig. 3).
Back from the Abyss
Fig. 1
Maxillary central incisor with slot-like access cavity that is cut short of the incisal edge, adequately under the cingulum, and has been kept narrow in its mesial-to-dimension.
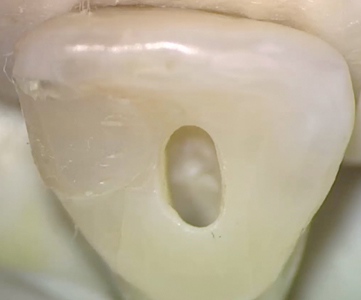
Fig. 2
Mandibular premolar with slot-like access cavity for a single canal root. Note how the access cavity is skewed toward the working buccal cusp tip and shy of the idling lingual cusp, yet is centered above the root structure.

Fig. 3
Sagitally-dissected maxillary molar with mesially-inclined access cavity – parallel to the mesial surface of the tooth and shy of the distal half of the tooth.

I was taught the Schilder technique at UOP by Dr. Michael Scianamblo, and after grad school by Dr. Cliff Ruddle, I understood the clinical imperative Dr. Schilder had placed on cutting an access cavity adequate to treat the entire root canal system in a predictable manner. I enjoyed working through the large access cavities and the generous coronal canal shapes he recommended, until I was brought up short by Dr. Carl Reider – a well-known prosthodontic lecturer from Southern California. When I asked what he most wanted from the endodontists he referred his patients to, he said he wished we could “just suck the pulp out without cutting any tooth structure”, and as we talked I came to better understand the structural imperative of saving teeth in the long-term, setting me on a quest for tools and methods that would allow us to achieve the same consistently ideal endodontic outcomes through smaller access openings and coronal canal shapes – ultimately the inspiration for my invention of the Maximum Flute Diameter (MFD) limitations on GT and GTX rotary files (Dentsply/Tulsa Dental Specialties), the LAX (line angle extension) Guided Access Diamond Burs by SybronEndo, as well as obturation methods using flexible condensation devices, such as System-B Continuous Wave electric heat pluggers (SybronEndo) and GT/GTX Obturators (Dentsply/Tulsa Dental Specialties).
The Itty-Bitty Access Committee
Since that initial awakening in the 80s, it has felt like being a lone voice in the wilderness until the last ten years until a new generation of dentists and endodontists, steeped in the new reality of implant dentistry as an alternative to RCT, have taken up the cry for longer term outcomes through improved post-treatment structural preservation, becoming a group I call The Itty-Bitty Access Committee. As so often happens, somebody outside of our specialty, a general dentist named Dr. David Clark started lecturing on the access elephant in the endodontic living room, he got my buddy Dr. John Khademi turned on by the possibilities that more conservative access cavities could offer the specialty 4, and one-by-one a group of young endodontists joined the game of who can do a perfect RCT through the smallest access cavity? and became the IBAC club.
The cases shown in Figures 4 through 10 – mostly done by IBAC members – make me very happy and afraid at the same time. Anybody can understand the advantage of conserving tooth structure during RCT, however, few clinicians can operate at the high, high levels seen in these amazing cases. Fortunately, when the endodontist is ready, new tech provides clinical solutions, namely in this case, dynamically-guided endodontic procedures.
Fig. 4
Mandibular molar with nearly total calcification of the pulp chamber prior to RCT accomplished through two perfectly dead-on access entry ports, leaving a .75 mm high pulp chamber isthmus between. Note the definitive treatment results in the apical thirds of each canal (courtesy Dr. N. Pushpak).

Fig. 5
Post-operative radiograph of a mandibular molar treated through the mesial carious defect and a second small entry cut through the central fossa. Preserving dentin between entry points is referred to as a “truss” access configuration (courtesy Dr. John Khademi).

Fig. 6
This post-operative radiograph shows a very diminutive access cavity opening with both mesial and distal lateral pulp horns unroofed during the RCT procedure and filled during the post-endodontic restorative effort – this appearance is a matter of pride among those in the “IBAC” club (courtesy Dr. Jeff Pafford).

Fig. 7
Access cavities cut in a mandibular molar requiring RCT (left). Post-operative radiograph (right) showing beautiful management of root canal shaping, cleaning, and filling – despite the minimal size of entry. Note the largely remaining pulp chamber roof (courtesy Dr. Steve Baerg).

Fig. 8
This restored access cavity design was opportunistic in the best sense of the word. This patient’s endodontic disease state was resolved with almost no tooth structure being cut and the post-operative structural integrity of a tooth with only a mesial operative restoration – no need for a full-coverage crown (courtesy Dr. Michael Trudeau).

Fig. 9
This lower molar was treated through an access opening that was less than 2 mm square, cut just behind the MB triangular ridge. Note the definitive treatment of the apical thirds of all four canals, despite the narrow entry portal (courtesy Dr. Charles Maupin).

Fig. 10
Post-operative radiograph of a mandibular molar treated through an alternative to the truss configuration – an “X-entry” access cavity – a design that minimizes removal of tooth structure in the critical trunk of the tooth (author’s case).

Dynamic CT-Guidance
Dynamic CT-guidance is the perfect answer to the harsh requirements of minimally-invasive RCT (MIE) procedures. The author’s experiences with static drill guides as used in implant surgery revealed their damning limitations for conventional access procedures, namely: 1) The insufficient inter-occlusal space for the occlusal guide and the extended length of guided drills, 2) Their guide rings are sufficient for slow speed implant drills but totally inadequate for guiding a high speed handpiece drill, 3) Static guides require days to receive from the lab but endo has immediate procedural requirements, and 4) Static guides cannot be changed during the procedure to take advantage of the additional information gained during the procedure.
Dynamic guidance, as seen with the X-Nav system (X-Nav Tech, Yorktown, PA), changes everything about how we treat calcified cases, how we pursue clinical MIE objectives, and ultimately, how we will perform endodontic surgery (Figs. 11 & 12).
Fig. 11 A, B, C
Totally calcified lateral incisor accessed with dynamic guidance.



Fig. 12 A, B, C, D, E, F
Independent access entry ports cut with dynamic guidance in this severely calcified molar.






And morning breaks over the field of endodontics. OH
Oral Health welcomes this original article.
References
- Persig, R, Zen and the Art of Motorcycle Maintenance: An Inquiry into Values, William and Morrow and Co., 1974.
- Gawande, A, The Checklist Manifesto, Metropolitan Books, 2009.
- Buchanan, LS, Digital Endodontics, The Sino-Anglo Dental Congress Beijing, China, 2014.
- Clark, D, Khademi, J, Herbranson, E. The New Science of Strong Endo Teeth, Dentistry Today, April, 2013.
About the Author
 Dr. Buchanan is a Diplomate of the American Board of Endodontics, he is a fellow of the American and International Colleges of Dentists, and he serves as part-time faculty to the UCLA and USC graduate endodontic programs. Dr. Buchanan holds patents on the Endobender Plier (SybronEndo), System-B and Continuous Wave obturation tools and methods (SybronEndo), GT and GTX file systems (Dentsply/Tulsa Dental Specialties), LA Axxess Burs (SybronEndo), and Buc ultrasonic tips (Spartan/Obtura). Dr. Buchanan lives in Santa Barbara, California where he enjoys practice limited to conventional and microsurgical endodontics and dental implant surgery. He is the founder of Dental Education Laboratories, a hands-on training facility in Santa Barbara he has directed for 28 years.
Dr. Buchanan is a Diplomate of the American Board of Endodontics, he is a fellow of the American and International Colleges of Dentists, and he serves as part-time faculty to the UCLA and USC graduate endodontic programs. Dr. Buchanan holds patents on the Endobender Plier (SybronEndo), System-B and Continuous Wave obturation tools and methods (SybronEndo), GT and GTX file systems (Dentsply/Tulsa Dental Specialties), LA Axxess Burs (SybronEndo), and Buc ultrasonic tips (Spartan/Obtura). Dr. Buchanan lives in Santa Barbara, California where he enjoys practice limited to conventional and microsurgical endodontics and dental implant surgery. He is the founder of Dental Education Laboratories, a hands-on training facility in Santa Barbara he has directed for 28 years.
RELATED ARTICLE: Dynamic Navigation For Orthograde And Retrograde Endodontics
Follow the Oral Health Group on Facebook, Instagram, Twitter and LinkedIn for the latest updates on news, clinical articles, practice management and more!










