Implant treatment for full arch fixed restorations have been around for decades now.1, 2, 4 The treatment usually involves 4-6 implants placed in either the maxilla or mandible which is then restored with a fixed partial denture.5 One of the benefits of this treatment is the ability to achieve a new fixed temporary set of teeth on the same day as implant surgery is completed.1-5 This temporary restoration is commonly known as a “conversion prosthesis” as it relates to the process of how the prosthesis is fabricated.3
Traditionally, an immediate denture prosthesis is “converted” to an implant supported temporary restoration after the implants are placed. The process of converting a denture to an immediate implant restoration can be tedious and requires significant chair time. Briefly, the steps involved in a traditional pick-up conversion prosthesis requires locating the implants relative to the denture, drilling holes in the denture at the implant locations, and attaching the temporary cylinders to the denture.3, 6 Once the implant cylinders are luted to the denture, it is removed from the mouth. Flanges are cut, voids are filled, and the intaglio adjusted for any bone reduction that may have occurred and to mold the tissues in a certain shape depending on the design of the prosthesis. Afterwards, the prosthesis is then inserted in the mouth. This entire process can be very tedious, messy, and time consuming.7
With digital technology in modern day dentistry, the process of fabricating an immediate conversion prosthesis can be much improved – both in terms of patient comfort and also clinical efficiency. This article will present 2 cases to showcase a digital workflow for dentate and edentulous patients using intraoral scanning and digital software to fabricate the conversion prosthesis.
Case 1: Partially dentate
The digital process starts with a digital wax-up long before the day of surgery. Proper planning for any case is vital to the success of a case and it applies here as well. Once the teeth positioning is finalized, a surgical plan can be put in place for implant placement. The virtual wax-up is saved and will be needed later on the day of surgery for the digital conversion.
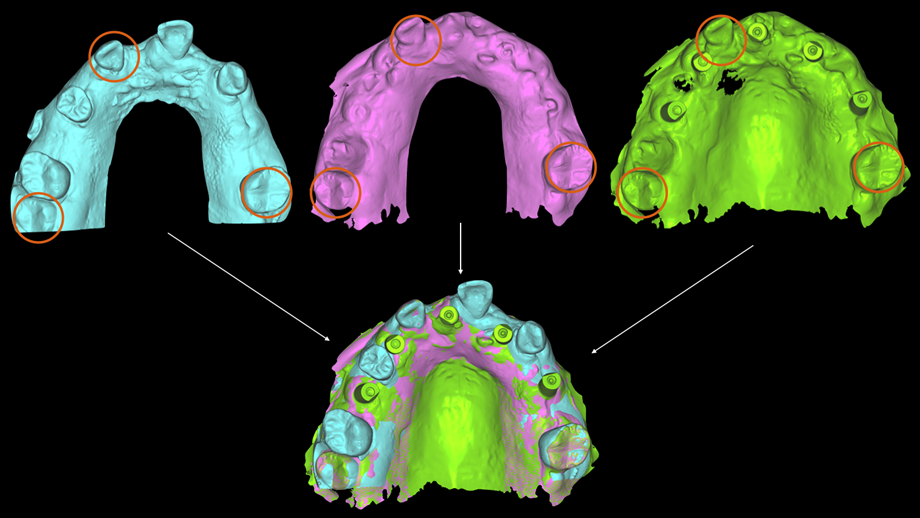
An important factor when it comes to digital conversion on the day of surgery is sequencing of both the surgery (extractions and implant placement) and intraoral scans. One of the benefits of digital technology is the ability to merge common points from one scan to the next. The basis of the conversion is to be able to merge the implant scan on the day of surgery back to the pre-surgical scan and thus have the original wax-up on the new implant scan. If no reference points exist between the original scan and the implant scan, then there will be difficulty in merging the two scans together and the new implant scan will be lost in 3D space with no way to reference it back. Thus, it is important to determine the reference points prior to surgery with a proper plan. For cases where the patient is still dentate or partially dentate, selective extractions while keeping specific teeth for reference is an easy way to be able to merge scans back to the pre-op scan.
Once the scans have been merged (Fig.3), the original wax-up can now be referenced to the new implant scan. Using dental software (Exocad DentalCAD), the conversion prosthesis can be designed by connecting the teeth in the wax-up to the implants. This process usually takes approximately 30 minutes as most of the time had already been spent prior to surgery when the wax-up was designed. After the digital conversion, the prosthesis is then 3D printed, processed, and inserted on the immediately placed implants.
Fig. 1

Fig. 2
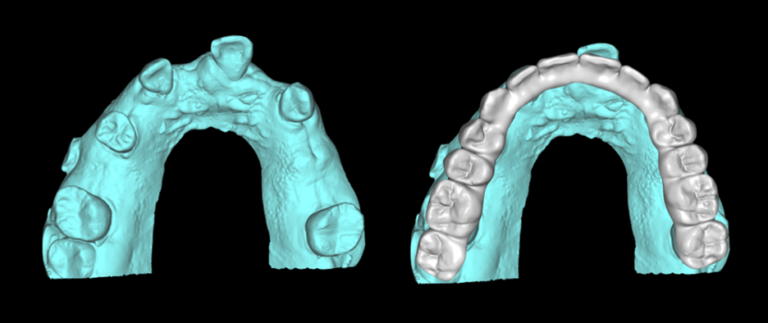
Fig. 3
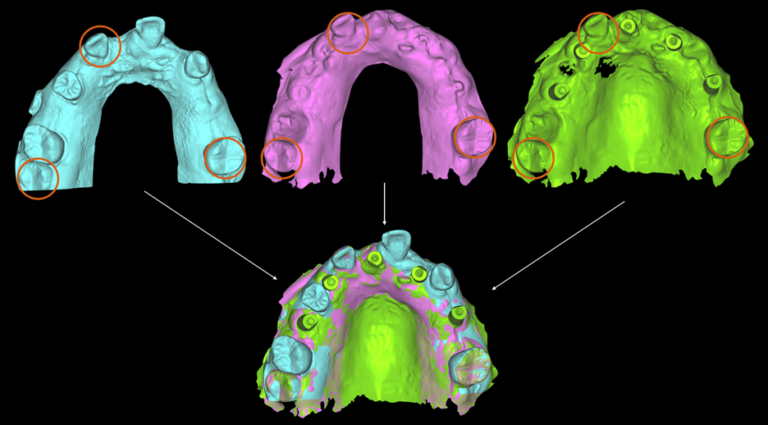
Fig. 4
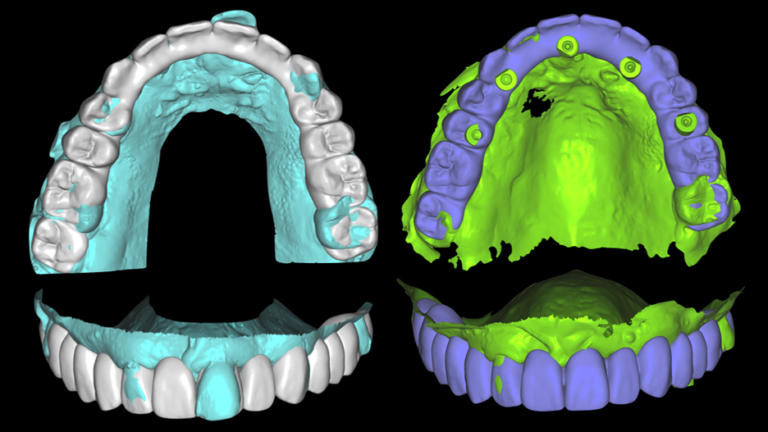
Fig. 5

Fig. 6

Case 2: Edentulous
For edentulous cases, a trial prosthesis is still necessary in order to test tooth positioning and vertical dimension prior to surgery as you would do with any other edentulous case. This trial prosthesis (which is fabricated from the digital waxup), also doubles as a way to connect the implant scan back to the digital waxup.
Since soft tissue is generally not reliable as a reference, especially during/after full arch implant surgery, reference points must be placed for the purpose of merging. These reference points can be any form of temporary screw that can be embedded in the bone for surgery. Examples include temporary anchorage devices (TADs) or tenting screws.
As seen in both Figures 8 and 9, the teeth of the trial prosthesis are able to be merged to the second interim scan. The TADs in the second scan are able to be merged to the third final implant scan. Thus, the third implant scan is now able to be related back to the original. Then, the same digital process is repeated as for the dentate patient and the prosthesis is 3D printed and inserted on the same day as surgery.
Fig. 7
Fig. 8
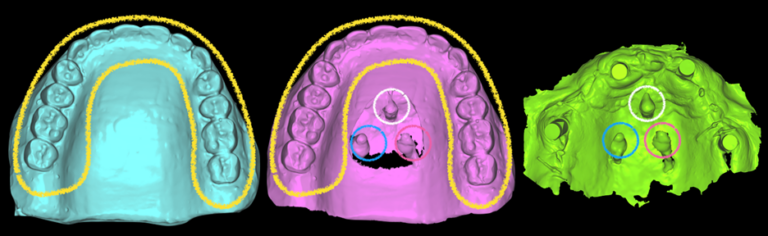
Fig. 9

Fig. 10
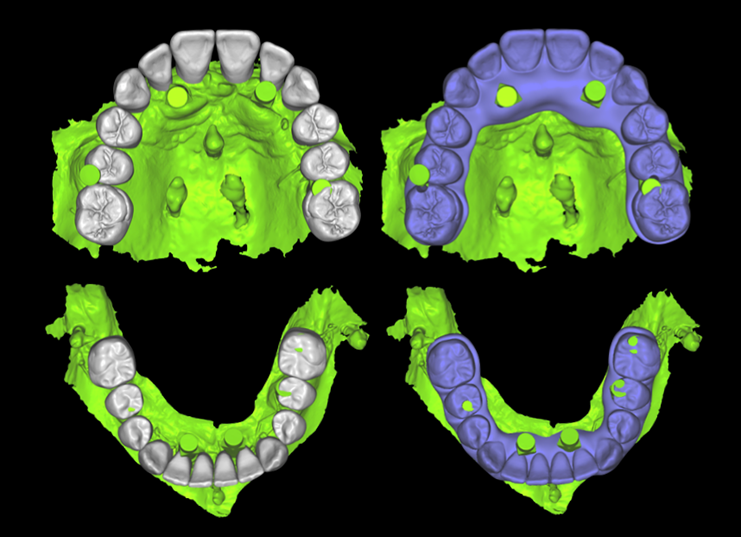
Fig. 11

Conclusion
The advancement of new digital technologies has enabled the conversion process to be cleaner, more streamlined, and more predictable. The increased accuracy in intraoral scanners, improved capabilities of dental software, and increased strength of 3D printed materials all play a role in these advancements. As the digital landscape continues to change, it is an exciting time to see which significant improvements in both patient comfort and care as well as dental clinical proficiency can be achieved. 
Oral Health welcomes this original article.
References
- Maló, P., Rangert, B., & Nobre, M. (2003). “All-on-Four” immediate-function concept with Brånemark System implants for completely edentulous mandibles: a retrospective clinical study. Clinical implant dentistry and related research, 5 Suppl 1, 2–9. https://doi.org/10.1111/j.1708-8208.2003.tb00010.x
- Maló, P., de Araújo Nobre, M., Lopes, A., Ferro, A., & Botto, J. (2019). The All‐on‐4 treatment concept for the rehabilitation of the completely edentulous mandible: A longitudinal study with 10 to 18 years of follow‐up. Clinical implant dentistry and related research, 21(4), 565-577.
- Balshi, T. J., & Wolfinger, G. J. (1996). Conversion prosthesis: a transitional fixed implant-supported prosthesis for an edentulous arch–a technical note. The International journal of oral & maxillofacial implants, 11(1), 106–111.
- Francetti, L., Agliardi, E., Testori, T., Romeo, D., Taschieri, S., & Fabbro, M. D. (2008). Immediate rehabilitation of the mandible with fixed full prosthesis supported by axial and tilted implants: interim results of a single cohort prospective study. Clinical implant dentistry and related research, 10(4), 255-263.
- Weber, H. P., Morton, D., Gallucci, G. O., Roccuzzo, M., Cordaro, L., & Grütter, L. (2009). Consensus statements and recommended clinical procedures regarding loading protocols. International Journal of Oral & Maxillofacial Implants, 24.
- Bidra, A. S. (2012). Chair-side fabrication of a fixed implant-supported prosthesis in an edentulous mandible from a diagnostic wax-up: a clinical report. The Journal of Oral Implantology, 38(3), 291–297. https://doi.org/10.1563/AAID-JOI-D-10-00079
- M. Taruna, B. Chittaranjan, N. Sudheer, S. Tella, M. Abusaad, Prosthodontic perspective to all-on-4® concept for dental implants, Journal of clinical and diagnostic research: JCDR 8(10) (2014) ZE16.
About the Author

Dr. Max Li is a Board Certified Specialist in Prosthodontics and a Fellow of the Royal College. Dr. Li focuses his practice around creating a healthy and functional dentition along with esthetic smiles. He currently maintains a full-time specialty practice in Toronto.