
Early orthodontic treatment refers to orthodontic intervention before the eruption of permanent dentition (except third molars) is complete.1 In orthodontic literature, the benefits of early orthodontic treatment have been a topic of much debate.2-10 Some clinicians may prefer to defer orthodontic treatment to the adolescent age period, however many others attempt to intervene in the mixed dentition to eliminate or reduce skeletal, dento-alveolar and neuro-muscular disharmonies. As in all clinical disciplines of dentistry, a thorough examination of a patient’s orofacial structures, along with the stage of skeletal and social maturity, is required to identify the best cases for early orthodontic intervention.
Treatment Timing
The timing of orthodontic treatment is crucial and depends on a variety of interactive factors. The patient’s maturation level, nature of malocclusion, estimated duration of treatment and required level of patient compliance are all determining factors in deciding whether early intervention is at all beneficial for the case. Table 1 shows a simple guideline for available orthodontic treatment options at different dental maturation stages.
Table 1

Advantages of Early Orthodontic Treatment
There are many benefits to providing early orthodontic treatment in select cases. The most important benefit would be elimination of destructive environmental factors such as non-nutritive sucking habits or functional mandibular shifts that affect the normal growth and development of facial and dento-alveolar structures. If not treated, functional issues become skeletal issues as the patient matures. Fixed appliance therapies to address skeletal issues in adolescent years are often much more demanding in nature and take longer to achieve the desired treatment outcome.
Other benefits include prevention of unwanted tooth movement or improvement of alignment of a drifted molar in the case of a local dento-alveolar problem, such as early loss of a primary molar. If left untreated, available arch space for premolars becomes insufficient. Initiating early orthodontic treatment before second molar eruption prevents the need for more complicated orthodontic treatment in adolescent years.
In some cases, early orthodontic treatment of excessively protruded upper incisors will boost the self confidence of the patient, as well as reduce the risk of trauma to those teeth.11 These young patients are either aware or made aware of their protruding upper incisors. In my clinical experience, they have the best compliance with the treatment requirements and get super motivated as their appearance improves.
Disadvantages of Early Orthodontic Treatment
It is imperative to understand that providing early orthodontic treatment may reduce a patient’s capacity to comply with the requirements of comprehensive orthodontic treatment that may need to be done later. Treatment objectives and time frame should be established clearly in order to prevent unnecessarily prolonged early orthodontic treatment that may “burn out” the patient for future orthodontic treatment.
In some cases, a patient may not be emotionally ready for early treatment and may benefit from orthodontic treatment at a later age. This is commonly observed in patients with non-nutritive sucking habits, where mom is ready to start treatment but little Johnny has other plans. Early orthodontic treatment fails regardless of the appliance choice as little Johnny will get creative to find a way to suck his thumb.
For the parent’s perspective, it is important to highlight that there is no guarantee that the results of early treatment will be maintained and that the orthodontic treatment will be provided in multiple phases, thus will take longer to complete and cost more than a single-phase treatment.
In order to do a “differential diagnosis” of the malocclusion, it is essential to do a comprehensive orthodontic exam that is not limited to dento-alveolar relations only but also includes facial appearance, dental maturation, functions and family history. For instance, a case with anterior cross-bite caused by retroclined upper incisors would benefit more from early treatment than a case with anterior cross-bite caused by true mandibular prognathism with a positive family history.
In this article, I will be presenting a few cases that benefited from early orthodontic treatment. All cases were in early mixed dentition stage at the beginning of treatment. You will be seeing similar dento-alveolar relations in the initial orthodontic records of some cases but different treatment approaches due to the different etiology of the malocclusions.
Case #1
This male patient was seven years and six months old when he was referred by his dentist for initial orthodontic examination. Patient had his bitewing X-rays taken at the last dental check-up appointment, where his dentist diagnosed ectopically erupting upper first molars (Fig. 1A). It was elected to extract upper second baby molars to let upper first molars erupt, and patient was booked for orthodontic records in eight months. Upon reviewing his initial orthodontic records, it was observed that his upper first molars erupted with a mesial drift and mesio-lingual rotation, reducing the available arch space for upper second bicuspids. His bite was further complicated by a forward mandibular shift due to retroclined upper incisors (Fig. 1B). Early orthodontic treatment was planned to distalize upper first molars bilaterally and procline upper central incisors. Treatment objectives were to increase the arch space available for upper second bicuspids and eliminate functional mandibular shift. Treatment was done with a series of upper removable orthodontic appliances (Figs. 1C & D). Treatment duration was one-year and three months. Treatment results have been stabilized by an upper removable retainer. Patient was placed on a recall schedule to monitor changes in his bite. In his last recall visit, his occlusion was in good Cl I buccal relation with good overbite and overjet. Mild dental crowding in the lower anterior teeth was observed, but it was decided to monitor the case for another 12 months (Figs. 1E & F).
Fig. 1A

Fig. 1B

Fig. 1C

Fig. 1D

Fig. 1E

Fig. 1F

Case #2
This eight-year nine-month-old female patient presented for an initial orthodontic examination with the desire to correct her under-bite. She was in mixed dentition stage with an ectopically erupting upper left canine (#23) and three missing bicuspids (#14, #24, #25) in the maxilla. Patient had anterior and posterior crossbites and lower jaw shifts to the front upon closure. There is no family history of under-bite (Fig. 2A). Her occlusion was monitored for 12 months to assess the growth and development of jaws. In her second cephalometric evaluation, it was observed that skeletal ratios in sagittal and vertical planes changed minimally (Fig. 2B). It was proposed to do growth modification treatment to stimulate maxillary growth in transversal and sagittal planes. Patient had a rapid maxillary expander followed by reverse pull headgear (Fig. 2C). Treatment duration was one-year and two months. Treatment results have been stabilized by an upper removable retainer while patient transitions into permanent dentition. The improvements in her bite and profile were satisfactory and stable as seen in progress orthodontic records (Figs. 2D-F).
Fig. 2A

Fig. 2B

Fig. 2C

Fig. 2D

Fig. 2E

Fig. 2F

Early treatment of Cl III cases is challenging, as the stability of treatment results depends on the amount and direction of jaw growth and development. It is imperative that parents should clearly understand the treatment objectives of early orthodontic treatment. Before initiating early orthodontic treatment for this case, parents were informed about the need for a second phase of orthodontic treatment with braces on the upper and lower teeth and the prosthetic rehabilitation of missing teeth after braces come off. The possibility of jaw surgery once patient stops growing
in case of poor response to treatment and/or unfavorable growth amount was also reviewed with parents before early treatment was initiated.
Case #3
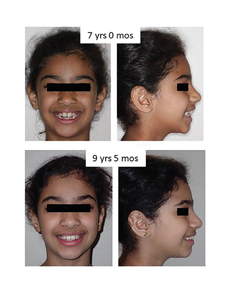
The patient was nine years and 10 months old at the initial orthodontic examination, referred by her dentist for excessive overjet. Initial orthodontic records demonstrated a Class II div 1 malocclusion of skeletal and dentoalveolar etiology, prognathic average maxilla and retrognathic small mandible, convex profile, reduced anterior lower face height, protruded and proclined upper and lower incisors, moderate to severe overjet, missing lower left central incisor (#31) and retained lower left central primary incisor (#71), moderate spacing in the maxillary arch and mesially tipped eruption pathways of upper canines (Fig. 3A). Patient was conscious that her upper teeth were “sticking out” too much. Patient’s mom also had a similar bite and had orthodontic treatment.
Fig. 3A

Early orthodontic treatment with growth modification appliances was proposed. Treatment objective was to reduce proclination of upper incisors and reduce maxillary spacing without compromising available space for upper canines. Cervical headgear and an upper removable orthodontic appliance were used for the treatment (Fig. 3B). Fixed appliance therapy with braces on the upper and lower teeth would be required to address missing #31. Treatment duration was only seven months because of excellent compliance with appliances. Progress orthodontic records showed good improvement in facial balance and lip competence and significant reduction in overjet (Figs. 3C & D). Treatment results were stabilized by an upper removable retainer and occasional use of cervical headgear. Patient’s mom was extremely satisfied with the treatment results, especially her daughter’s remarkable boost in self-confidence.
Fig. 3B

Fig. 3C


Fig. 3D

Case #4
This female patient was seven years old when she presented for initial orthodontic examination due to her mother’s concern of open bite. Initial orthodontic records showed Class II div 1 malocclusion of skeletal, dento-alveolar and neuromuscular etiology associated with convex profile, orthognathic maxilla and retrognathic mandible, increased mandibular plane angle, protruded and proclined upper incisors, anterior open bite, moderate overjet, missing #35,45 and persistent thumb sucking habit (Fig. 4A). Patient was motivated to stop the habit. Early orthodontic treatment with removable orthodontic appliances was proposed. Treatment objective was to improve anterior open bite by eliminating thumb sucking habit and controlling vertical growth of posterior teeth. Before initiating early orthodontic treatment, parents were informed that fixed appliance therapy will be required to address missing #35 and #45. Treatment duration was two years and five months. Progress orthodontic records show a positive overbite and significant improvement in patient’s facial appearance (Figs. 4B &C). Treatment results were stabilized by an upper removable retainer modified to control posterior vertical growth.
Fig. 4A

Fig. 4B

Fig. 4C
Case #5
This female patient was eight years old when she was referred for initial orthodontic examination by her dentist. Her initial orthodontic records showed slight mandibular asymmetry to the left side at maximum inter-cuspation, good profile and unilateral posterior cross bite on the left side with functional mandibular shift following a premature contact at #63 and #73 (Fig. 5A). Early orthodontic treatment with removable orthodontic appliances was proposed to eliminate mandibular shift. Treatment duration was one-year and four months. Progress orthodontic records show significant improvement in facial and dental symmetry and elimination of posterior cross bite (Figs. 5B & C). Treatment results were stabilized by an upper removable retainer.
Early orthodontic treatment of lateral mandibular shift is strongly recommended because a simple orthodontic treatment could prevent the development of skeletal mandibular asymmetry, which could not be corrected satisfactorily without orthognathic surgery.
Fig. 5A

Fig. 5B

Fig. 5C

Summary
The timing of orthodontic and orthopedic treatment depends on the nature of the malocclusion. Some cases respond very well to early treatment, while for other cases it is best to defer treatment to a later age. It is our duty to perform a comprehensive orthodontic examination to identify the orthodontic needs of our patients and the best timing for treatment. I would like to emphasize that early orthodontic treatment is not always necessary; good clinical judgement is required to weigh the benefits and risks in each individual case.
Oral Health welcomes this original article.
Acknowledgement:
I would like to dedicate this article to one of my mentors, the late Dr. Howard Tile, for showing us how to inspire the next generation of dentists by being kind, caring and compassionate to one another. In his 50 years of teaching in the graduate department of orthodontics at University of Toronto, he had passed his love of orthodontics and his zest for life to all his students. He will be dearly missed.
References:
- Orthodontics: Current principles and techniques, sixth edition. Graber L.W.; Vanarsdall R.L; Vig K.W.L.; Huang G.J. Part 3, Chapter 16, 403-433.
- Early orthodontic treatment: what are the imperatives? Kluemper GT, Beeman CS, Hicks EP. J Am Dent Assoc. 2000 May;131(5):613-20.
- Comparison of early treatment outcomes rendered in three different types of malocclusions. Pangrazio-Kulbersh V, Kang HK, Dhawan A, Al-Qawasmi R, Pacheco RR. Angle Orthod. 2018 May;88(3):253-258.
- Early vs late orthodontic treatment of tooth crowding by first premolar extraction: A systematic review. Lopes Filho H1, Maia LH, Lau TC, de Souza MM, Maia LC. Angle Orthod. 2015 May;85(3):510-7.
- Effectiveness of the open bite treatment in growing children and adolescents. A systematic review. Feres MF, Abreu LG, Insabralde NM, Almeida MR, Flores-Mir C. Eur J Orthod. 2016 Jun;38(3):237-50.
- Retrospective 25-year follow-up of treatment outcomes in angle Class III patients : Early versus late treatment. Wendl B, Muchitsch AP, Winsauer H, Walter A, Droschl H, Jakse N, Wendl M, Wendl T. J Orofac Orthop. 2017 May;78(3):201-210.
- Early orthodontic treatment for Class III malocclusion: A systematic review and meta-analysis. Woon SC, Thiruvenkatachari B. Am J Orthod Dentofacial Orthop. 2017 Jan;151(1):28-52.
- Early treatment of Class III malocclusion with facemask. Smyth RSD, Ryan FS. Evid Based Dent. 2017 Dec 22;18(4):107-108.
- Effectiveness of early orthopaedic treatment with headgear: a systematic review and meta-analysis. Papageorgiou SN, Kutschera E, Memmert S, Gölz L, Jäger A, Bourauel C, Eliades T. Eur J Orthod. 2017 Apr 1;39(2):176-187.
- One phase or two phase orthodontic treatment for Class II division 1 malocclusion? Veitz-Keenan A, Liu N. Evid Based Dent. 2019 Sep;20(3):72-73.
- Early orthodontic treatment for Class II malocclusion reduces the chance of incisal trauma: Results of a Cochrane systematic review. Thiruvenkatachari B, Harrison J, Worthington H, O’Brien K. Am J Orthod Dentofacial Orthop. 2015 Jul;148(1):47-59.
About the Author
 Dr. Emel Arat is an Assistant Professor at the University of Toronto, immediate past president of Ontario Association of Orthodontists and is in private practice in Leaside, Toronto, Ontario. She can be reached at emel.arat@dentistry.utoronto.ca
Dr. Emel Arat is an Assistant Professor at the University of Toronto, immediate past president of Ontario Association of Orthodontists and is in private practice in Leaside, Toronto, Ontario. She can be reached at emel.arat@dentistry.utoronto.ca










