Abstract
Orthodontic clinical practice has used static forces for tooth movement and to modulate osteogenesis of craniofacial sutures for more than one hundred years. However, research has demonstrated that cyclic forces at 0.2 Hz delivered for 10 min/d over 12 days (120 cycles per day) evoke more craniofacial growth and osteogenesis in the premaxillary suture than static forces of matching peak magnitude and duration.1
Mechanical forces that are transmitted as tissue-borne and cell-borne mechanical strain can, in turn, regulate gene expression, cell proliferation, differentiation, maturation, and matrix synthesis, the totality of which is growth and development.2 It has been shown that cyclical mechanical stimulation can result in osteogenic differentiation of human intraoral mesenchymal stem and progenitor cells.3
The purpose of this article is to demonstrate that a removable orthopedic/orthodontic dental appliance, the Homeoblock™, can provide both cyclical forces and mechanical strain and can generate osteogenesis and growth and development in the craniofacial region.
We will present 5 case studies, patients that have been treated with the Homeoblocktm appliance for up to 24 months.
Diagnosis and etiology
The selected patients had facial asymmetry, which was evaluated as a lack of full craniofacial development. Symptoms varied from chronic rhinosinusitis, premature facial aging to breathing disordered sleep.
Methods
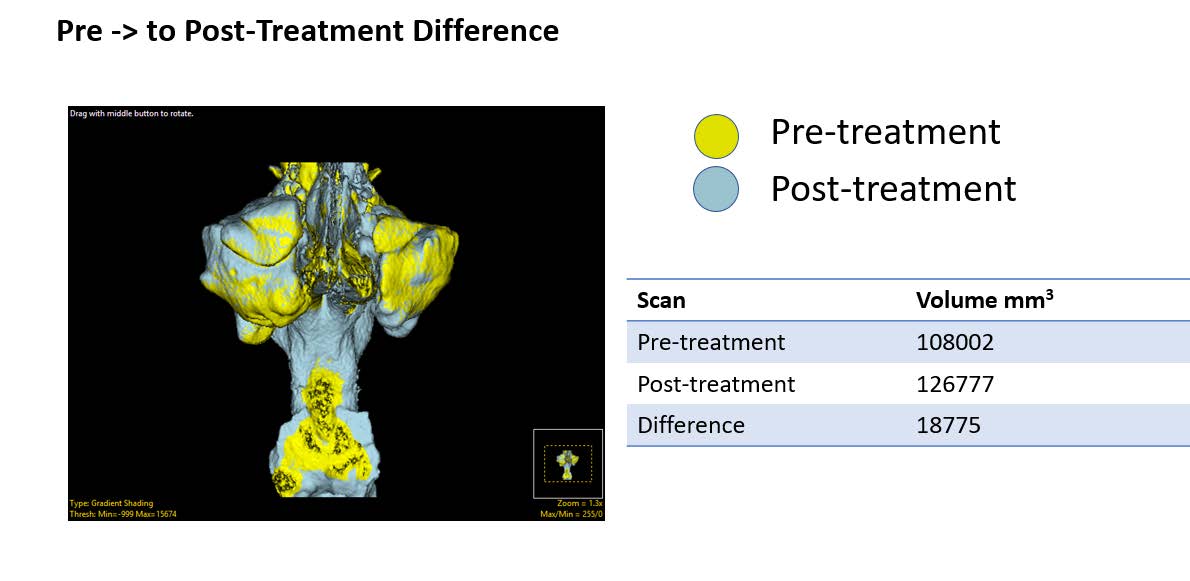
Subjects had two cone beam computed tomography (CBCT) scans acquired, one before treatment (T1) and a second after 24-months of treatment (T2). Upper and lower dental models were made and Homeoblock™ upper dental appliances were fabricated for the patient. The Homeoblock™ utilizes an orthodontic expansion screw along with Unilateral Biteblock Technology™. The unilateral 5mm bite block is placed on the second bicuspid and first molar on the less developed side of the face, which is the side which can have a deeper nasolabial depression or lower eye, thinner upper lip or deeper pre-jowl region. The appliances were worn a maximum of 10-12 hours each day (mainly during sleep) for up to 24 months. The patient was instructed to advance the expansion screw 0.125 mm (1/4 turn) each week. The patient returned periodically for minor adjustments.
Independent evaluation of the pre-treatment (T1) and post-treatment (T2) CBCT scans was performed by an analysis technician using Analyze 14.0 software (Biomedical Imaging Resource, Mayo Clinic, MN, USA). The T1 and T2 scans were first co-registered and transformed using a rigid mutual information maximization algorithm. Next, the T1 and transformed T2 scans were used as inputs for segmentation. A 3D region-growing algorithm was then utilized the isolate the pre-treatment and post- treatment airways. The resulting airway volumes were then calculated. Threshold based segmentation was then utilized to segment the bone from the T1 and transformed T2 scans to evaluate pre-post dentoskeletal difference.
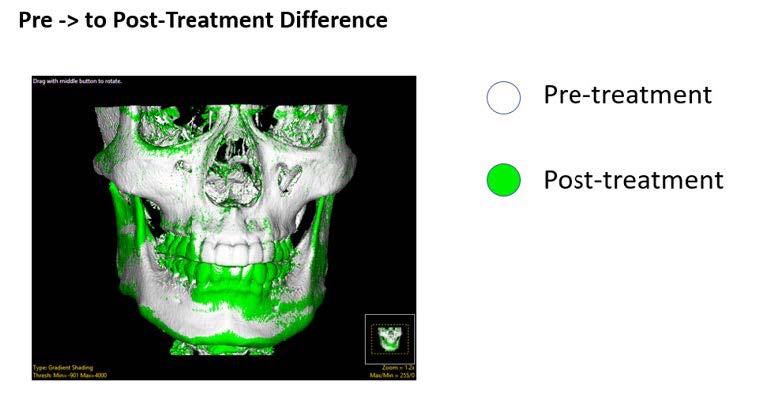
Case study I
- The green shows the teeth moving wider in the upper jaw.
- The zygoma has moved outward on the left side.
- The ramus is wider on both sides
- There are changes in the greater wing of the sphenoid in conjunction with the mandible moving downward.
- The frontal and zygomatic bones have moved outward. The mandible has moved downward and to the right side


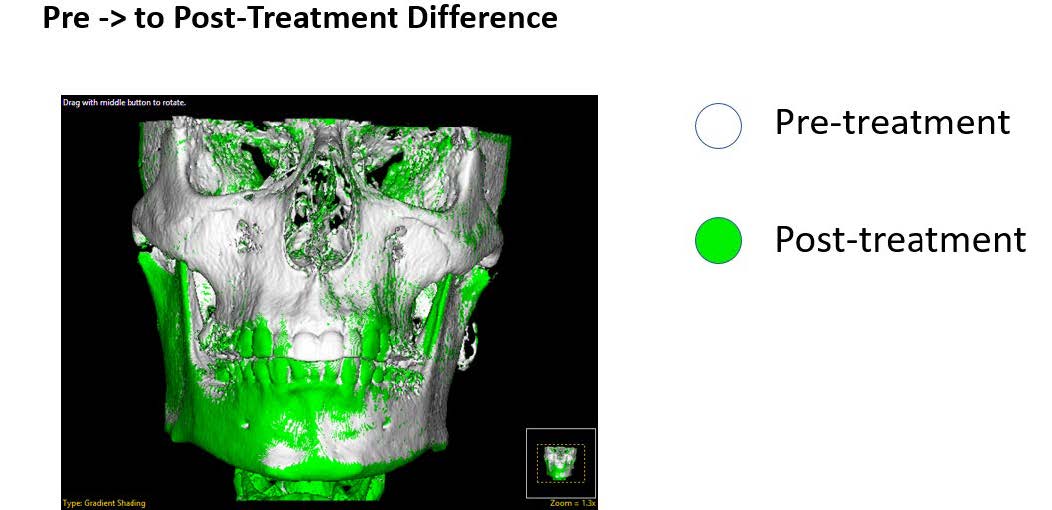
Case study II
- The green shows the teeth moving wider in the upper arch and new bone growth at the inferior border of the right orbit.
- The ramus of the mandible has moved wider on the right side and there are changes in the coronoid process on the left side.
- There are changes in the greater wing of the sphenoid on both sides and the mandible has moved downward.

Case study III
- Green shows that the teeth have moved wider.
- There is growth in the maxilla on the left side
- The mandible has come down and to the right side.
- There are changes in the greater wing of the sphenoid bone that are consistent with the mandible repositioning

Case study IV
- Green shows chnges in the greater wing of the sphenoid
- There is growth in the maxilla with new bone at the inferior border of the orbit, and a wider dental arch.
- The zygoma has moved out on the right side.
- The ramus is wider on the right side


Case study V
- The green shows maxillary bone growth additional bone at the inferior border of the orbit on the right side.
- The zygoma has moved outward on the right side. The ramus of the mandible is wider.
- There are changes in the greater wing of the sphenoid on both sides. The mandible has come downward and to the left side.

Results
These results demonstrate that changes are possible in both the face and the airway in so called non- growing adults. These results can contribute to a better understanding of strain-induced bone remodeling. What we show here is consistent and reproducible bone remodeling bone repositioning and new bone growth. All the changes are in regions that are subject to the distribution of the forces of chewing.4
DISCUSSION
Mechanotransduction, mechanical stimulation, plays a central role in the physiology of many tissues including bone. Dynamic cyclic loading is associated with fluid movement around the osteocytes and cyclic forces impact cells multiple times compared to static forces. The difference in force frequency between cyclic forces and static forces leads to drastic differences in cellular response.7,8,9
The oscillatory component of cyclic strain is a potent stimulus for osteogenesis and it has been demonstrated that both microscale tension and compression forces induce an anabolic sutural growth response.10 The application of brief doses of cyclic forces induces sutural osteogenesis more effectively than static forces with matching peak magnitude. A static force with zero frequency has much less stimulatory effects than higher frequency cyclic forces. High frequency cyclic forces in either tension or compression induce modeling and growth changes in cranial sutures. These cyclic tensile or compressive forces are transmitted as shear stresses and upregulate genes and gene products responsible for sutural growth.11 Shear stress induces osteogenic differentiation of human mesenchymal cells (MSCs) in vitro.12 Also, cyclic tension promotes osteogenic differentiation in human periodontal ligament stem cells.13 Therefore, it is possible to promote osteogenesis from mesenchymal cells, MSCs located in the periodontal ligament, PDL and the maxillary suture system in adults.14
Oral Health welcomes this original article.
References
- Mao, JJ, W. X. (2003, Jan 1). Strain induced osteogenesis of the craniofacial suture upon controlled delivery of low-frequency cyclic forces. Front Biosci(8), a10-7.
- Mao, JJ, Nah HD. Growth and development. Hereditary and mechanical modulations. Am J dentofac orthop 125: 676-689, 2004.
- Lohberger B. Kaltenegger H, Steed N, Payer M. Effect of Cyclic Mechanical Stimulation on the Expression of Osteogenesis Genes in Human Intraoral Messenchymal Stromal and Progenitor Cell Bio Res Int. 2014; 2014:189516.
- Danial E Lieberman. The Evolution of the Human Head.
- Belfor T.R. Epigenetic Orthodontics: facial and airway development. The New York State Dental Journal 76(6):18-21 Oct. 2010.
- Belfor T.R. Singh G. D. Developing dental arch symmetry using the Homeoblock device. International Journal of Orthodontics 15(3):27-30 January 2004.
- Kopher RA, M. J. (2003, Mar). Suture Growth modulated by the oscillatory component of micromechanical strain. J Bone Miner Res, 18(3), 521-8.
- Peptan AI, Lopez A, Kopher RA, Mao JJ. (2008) Responses of intramembranous bone and sutures upon in vivo cyclic tensile and compressive loading. Bone. 2008 Feb;42(2):432-8.
- Yourek G, McCormick SM, Mao JJ, Reilly GC (2010). Shear stress induces osteogenic differentiation of human mesenchymal stem cells. Regen Med. 2010 Sep:5(5):713-24.
- Shen T, Qiu K, Chang H et al (2014). Cyclic tension promotes osteogenic differentiation in human periodontal ligament stem cells. Int J Clin Exp Pathol 2014 Oct 15;7(11):7872-80.
- Kopher RA, M. J. (2003, Mar). Suture Growth modulated by the oscillatory component of micromechanical strain. J Bone Miner Res, 18(3), 521-8.
- Peptan AI, Lopez A, Kopher RA, Mao JJ. (2008) Responses of intramembranous bone and sutures upon in vivo cyclic tensile and compressive loading. Bone. 2008 Feb.
- Yourek G, McCormick SM, Mao JJ, Reilly GC (2010). Shear stress induces osteogenic differentiation of human mesenchymal stem cells. Regen Med. 2010 Sep:5(5):713-24.
- Shen T, Qiu K, Chang H et al (2014). Cyclic tension promotes osteogenic differentiation in human periodontal ligament stem cells. Int J Clin Exp Pathol 2014 Oct 15;7(11):7872-80.
About the Authors
 Theodore R. Belfor, DDS, is a graduate of New York University College of Dentistry, a Senior Certified Instructor for the International Association for Orthodontics (IAO) and has been in private practice for more than 40 years. His work is devoted to understanding the causes of sleep and breathing disorders through individual patient craniofacial analysis. He can be reached at drtheodorebelfor.com
Theodore R. Belfor, DDS, is a graduate of New York University College of Dentistry, a Senior Certified Instructor for the International Association for Orthodontics (IAO) and has been in private practice for more than 40 years. His work is devoted to understanding the causes of sleep and breathing disorders through individual patient craniofacial analysis. He can be reached at drtheodorebelfor.com
 Michael Philcock has more than 15 years of experience in the processing and analysis of biomedical imaging data for a wide range of biological applications in the healthcare, life sciences, pharmaceutical and biotech industries.
Michael Philcock has more than 15 years of experience in the processing and analysis of biomedical imaging data for a wide range of biological applications in the healthcare, life sciences, pharmaceutical and biotech industries.
 Scott Simonetti, DDS, earned his Bachelor of Science in Nutritional Sciences from Cornell University and then attended the University at Buffalo School of Dental Medicine where he earned his DDS degree. Dr. Simonetti has been in private general practice on Long Island since 2001. He is the inventor of the FDA cleared and patented custom oral orthotic, The POD®.
Scott Simonetti, DDS, earned his Bachelor of Science in Nutritional Sciences from Cornell University and then attended the University at Buffalo School of Dental Medicine where he earned his DDS degree. Dr. Simonetti has been in private general practice on Long Island since 2001. He is the inventor of the FDA cleared and patented custom oral orthotic, The POD®.
RELATED ARTICLE: COVID-19 Increases Value of Oral Appliance Therapy for Sleep Apnea