
A sialolith is a yellowish-white, hard, concretion of organic and inorganic matter formed within any of the major or minor oral salivary glands or their excretory ducts.1 They are also referred to as salivary stones. Sialoliths are usually detected when they grow to a sufficient size whereby they start occluding a duct causing post prandial swelling and discomfort distal to the impasse. This condition is referred to as sialolithiasis. It has been reported that 90% of cases present with an infection in the associated salivary gland.1 Less than 1 in 10,000 of the population suffers from this condition and 85% of salivary stones are located within the submandibular gland or duct.2 This may be a function of it producing a more viscous and alkaline saliva containing higher concentrations of hydroxyapatite and phosphates which may make this gland more prone to the formation of salivary stones compared to the parotid or sublingual salivary glands.1 Most sialoliths range in size from 1 to 10 mm in length;3 however, the largest recorded sialolith was 70 mm long.4 Men are twice as likely to develop sialoliths than women; however, some studies have shown an equal distribution between the sexes.5 The condition mainly affects those between 30 and 60 years of age.5 There is no predilection for a left or right side presentation. 1 Imaging used to detect sialolith location within a salivary gland or duct includes radiography, X-ray sialography, ultrasound, CT scan, MRI, and sialendoscopy.6
Case report
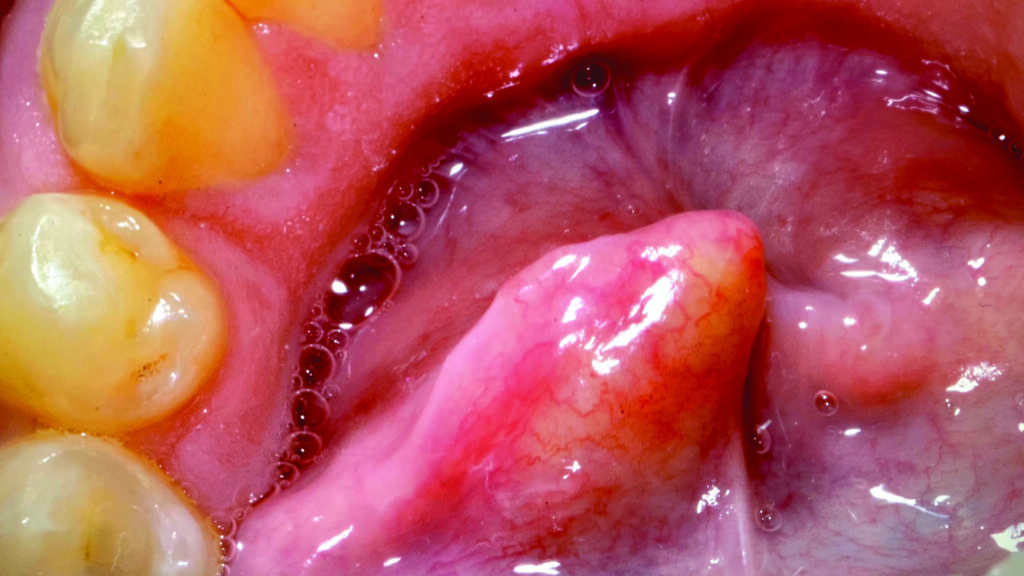
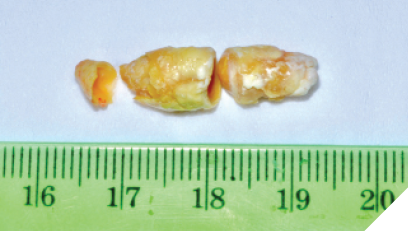
A 52-year-old male patient presented initially to the dental clinic with a non painful swelling in the left floor of his mouth. He had been previously informed by an oral surgeon that if no pain was present, then no action was required. Seven years later, however, the patient requested removal of the mass as it was uncomfortably crowding his mouth. Diagnosis was made by physical examination as the tongue was observed to be elevated and canted at forty five degrees due to a protruding, hard, yellowish mass within the left Wharton’s duct adjacent to the lingual frenum, see Figure 1. Under local anesthesia the Whartons’ duct was lanced superiorly, and the salivary stone was squeezed out through the incision. As seen in Figure 2, the fragmented, telescoping sialolith was yellowish white in appearance and measured approximately 25 mm in length. The duct proceeded to heal uneventfully by secondary intention without complication.
Fig. 1
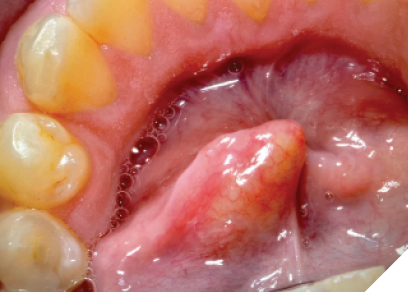
Fig. 2
Discussion
A sialolith grows by concretion of organic and inorganic matter that precipitates out of solution around a nidus. The source of the nidus could be organic debris entering through the gland duct orifice or possibly from desquamated epithelial cells or microparticles from within the gland itself. The genesis of sialolithiasis is presently a topic of research with many factors under consideration such as decreased fluid consumption, effects of prescription drugs on flow levels and tobacco use.7 The patients’ medical history was unremarkable and, therefore, no possible cause can be offered. One retrospective study found that 16.9% of patients with sialolithiasis had multiple stones8 and there was one case where a patient had more than 40 stones.2 It is, therefore, advisable to image every patient where a stone has been discovered in order that all stones be revealed and dealt with. 
Oral Health welcomes this original article.
Acknowledgement: The author would like to thank the office of Dentistry on Derry, Mississauga, Ontario for providing the details of this case.
About the Author

Stirling Moss is a fourth-year dental student at James Cook University, Australia. Stirling.moss@my.jcu.edu.au.










