
INTRODUCTON
As dental practitioners, we are continuously challenged to rely on our knowledge and experience to guide us when making recommendations to our patients. A thorough clinical exam is essential to narrowing in on a diagnosis. Additionally, an appropriately timed radiograph can prevent undesired sequala. The following case illustrates the value of routine orthodontic radiography in determining the appropriate timing for orthodontic treatment.
THE CASE
Upon clinical exam, it was noted that this exhibited mixed dentition occluding in a moderate Class III molar relationship associated with a straight profile, mild mandibular asymmetry (to the patient’s left), moderate mandibular Curve of Spee, a narrow upper arch, mild-to-moderate anterior crowding, a cross bite at tooth 12 and slim 12 and 22 teeth (ie. upper anterior Bolton deficiency). Tooth 23 was noted to be delayed in erupting, with no notable buccal or palatal bulge on palpation. (Fig. 1)
Fig. 1

Radiographic examination determined that the etiology of his Class III malocclusion was a mildly prognathic, asymmetric and long mandible with lower incisors in a retrusive position and upper incisors in a proclined orientation (thereby camouflaging the degree of underlying Class III relationship). (Figs. 2,3)
Fig. 2

Fig. 3
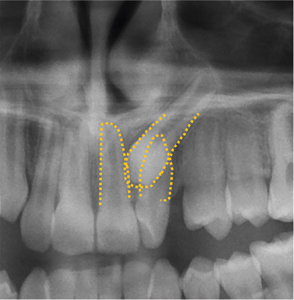
Panoramic radiography showed that Tooth 23 exhibited almost complete root formation and was impacted and partially transposed, with its crown past the mesial aspect of tooth 22 and with ~40° angulation.
Further radiographic investigation was pursued with a CBCT. Tooth 23 was labially positioned to tooth 22 with the crown of 23 abutting the disto-buccal root surface of 21. No root resorption was noted on either 21 or 22. (Fig. 4)
Fig. 4

DIAGNOSIS
The patient’s diagnosis was one of a Class III malocclusion of skeletal and dental etiology associated with a straight profile, prognathic, long and asymmetric mandible, narrow maxilla, moderate lower arch Curve of Spee, retruded lower incisors, proclined upper incisors, mild-moderate crowding, impacted tooth 23 and cross bite at tooth 12.

TREATMENT
After reviewing the above treatment concerns, it was agreed that comprehensive treatment of the Class III malocclusion would be deferred until after further growth had occurred. Treatment in the upper arch was pursued to correct tooth 23, comprising of the following steps:
1. Upper Expander (Fig. 5):
- to increase the width of the maxilla and relieve crowding.
- to provide cross-arch stabilization and facilitate the orthodontic mechanics needed for the retrieval of tooth 23.
Fig. 5

2. Surgical exposure of tooth 23 (Fig. 6):
- an exposure with gold chain attachment was performed by a periodontist with considerations towards the preservation of the gingival attachment of tooth 22.
Fig. 6

3. A ballista spring extending from the RPE (Fig. 7):
- to move tooth 23 first labially then distally to avoid contact with 22, thereby reducing the risk of root resorption.
Fig. 7

4. Segmental fixed appliances (Fig. 8):
- to continue the retraction of tooth 23 away from tooth 22 and into position. Tooth 22 was not manipulated at this time to reduce the risk of root resorption.
Fig. 8

5. Full upper arch fixed, edgewise appliances:
- to correct the 12 crossbite and prepare spaces about teeth 12 and 22 for possible future buildups.
6. Retention:
- both fixed and removable retention were employed to protect the treatment results. (Fig. 9) Depending on the degree of growth, this patient may be treated with lower +/- upper orthodontic therapy. If growth is favorable, the completion of his comprehensive orthodontic treatment may be possible without a discussion of orthognathic surgery.
Fig. 9

DISCUSSION
Class III malocclusions account for between 0-26% of malocclusions, depending on the population of interest. Generally, caution regarding the treatment of patients with Class III malocclusions stems from the risk of a persistent or recurring underbite due to progressive mandibular prognathism or maxillary retrognathism. Therefore, comprehensive treatment must consider these risks and often the comprehensive treatment for moderate to severe Class III presentations will be deferred until growth is complete or near completion. If non-bone anchored orthopedic intervention is to be pursued via maxillary protraction, it is best completed before the age of 10 years of age.1,2
In the above case the use of a lateral cephalogram was essentially in identifying the etiology of the Class III malocclusion, namely mandibular prognathism. It also clarified that the extraoral finding of a chin point to the patient’s left (Fig. 1) was secondary to an asymmetric mandible rather than soft tissue variations. (Fig. 2)
Due to his stage of growth and development, comprehensive orthodontic management of his Class III malocclusion was deferred until a later stage of development. However, the finding of an impacted and transposed tooth 23, undertaking interceptive treatment was beneficial.
Although various permanent tooth eruption sequences exist, the upper canines will typically erupt by age 12. In this case, at first glance the absence of tooth 23 was not surprising. However, the degree of delay of the eruption of tooth 23 combined by the inability to palpate any canine bulge and the displacement of tooth 22 (showing mild proclination and rotation secondary to the ectopic eruption of 23 position) promoted a radiographic investigation, yielding the finding of an impacted 23.
Impacted canines occur in 2% of the general population with a 2:1 occurrence in females vs males with a 2:1 occurrence in the palate vs labially.3 Appreciating the orientation of the canine and the degree of overlap of adjacent teeth (often the lateral incisor), interventions may include no treatment, extraction of the primary canine or surgical exposure of the canine.4,5
CONCLUSION
The above case illustrated the challenge of when to begin treatment when two atypical findings (i.e. both Class III malocclusion and canine impaction) presented at the same time.
The management of the Class III malocclusion would ideally be reviewed by 7-9 years of age to be able to explore the possibility of interceptive treatment options.
The comprehensive management of a Class III malocclusion must consider the risk of late mandibular growth.
Canine impaction can be detected by a delay in eruption, the absence of a canine bulge on a clinical exam and concurrent radiography.
Management of canine impaction(s) depends on the degree of impaction and must be considerate of potential iatrogenic damage to adjacent teeth.
Oral Health welcomes this original article.
References
- Clemente R, Contardo L, Greco C, Di Lenarda R, Perinetti G. Class III Treatment with Skeletal and Dental Anchorage: A Review of Comparative Effects. Biomed Res Int. 2018 Jul 2;2018:7946019. doi: 10.1155/2018/7946019. PMID: 30057910; PMCID: PMC6051274.
- Ngan P, Moon W. Evolution of Class III treatment in orthodontics. Am J Orthod Dentofacial Orthop. 2015 Jul;148(1):22-36. doi: 10.1016/j.ajodo.2015.04.012. PMID: 26124025.
- Becker A, Chaushu S. Etiology of maxillary canine impaction: a review. Am J Orthod Dentofacial Orthop. 2015 Oct;148(4):557-67. doi: 10.1016/j.ajodo.2015.06.013. PMID: 26432311.
- Naoumova J, Kjellberg H. The use of panoramic radiographs to decide when interceptive extraction is beneficial in children with palatally displaced canines based on a randomized clinical trial. Eur J Orthod. 2018 Nov 30;40(6):565-574. doi: 10.1093/ejo/cjy002. PMID: 29462471.
- Ericson S, Kurol J. Early treatment of palatally erupting maxillary canines by extraction of the primary canines. Eur J Orthod. 1988 Nov;10(4):283-95. doi: 10.1093/ejo/10.4.283. PMID: 3208843.
About the Author
 Dr. Sean Chung completed his DMD (’09) and GPR (’10) at the University of British Columbia and MSc (Ortho), FRCD(C) (‘13) at the University of Toronto. He maintains his private practise, North Toronto Orthodontists, and is an instructor in the Graduate Orthodontics and Pediatric Dentistry departments at the University of Toronto, Faculty of Dentistry. He can be reached at schung@NorthTorontoOrtho.com
Dr. Sean Chung completed his DMD (’09) and GPR (’10) at the University of British Columbia and MSc (Ortho), FRCD(C) (‘13) at the University of Toronto. He maintains his private practise, North Toronto Orthodontists, and is an instructor in the Graduate Orthodontics and Pediatric Dentistry departments at the University of Toronto, Faculty of Dentistry. He can be reached at schung@NorthTorontoOrtho.com
RELATED ARTICLE: Periodontal And Prosthodontic Management Of Class III Malocclusion: A Case Report










