

Abstract
The use of a pacifier in newborns is a common practice. Extended use of the pacifier can cause deviation of the craniofacial growth in children, as well to create oral dysfunctions such as mouth breathing and tongue thrusting. In this paper the authors present an appliance designed to stop the pacifier habit and to correct the consequences of its use, the Pediatric BioActivator DC. A clinical case of a three years old girl with an open bite associated with an anterior crossbite tendency and functional disorders is presented here. The patient was treated in the primary dentition with the BioActivator appliance discouraging the use of the pacifier and correcting the dental malocclusion and the oral dysfunctions. The treatment was delivered at an early age in primary dentition combining the BioActivator appliance with myofunctional therapy.
The pacifier use has been promoted by pediatricians and at hospitals around the world over the last +50 years to prevent sudden infant death (SIDs).1 However, the scientific literature supports that a proper breastfeeding may reduce even more the incident of SIDs in new borns.2 The continuous use of a pacifier creates a habit in the newborn deviating the craniofacial growth and development,3 and creating disturbances in the tongue posture at rest and when swallowing at a later age.4,5
The continuous use of a pacifier by a child up to the age of 2 to 3 years old frequently results in a lower position of the tongue, resting at the floor of the mouth and not elevating to the palate at rest, as well as tongue thrusting at swallowing and dental malocclusions such as an open bite.5,6 At that age, the parents struggle to stop the habit, a task very difficult to achieve, as the habit has been established as a behavioral pattern in the child.7
Early interception of a deviation in craniofacial growth and development in children, as well as intercepting developing malocclusions at an early age have been highly recommended in the scientific literature.8-12 However to start an interceptive orthodontic treatment in a young child is not easy for the dental professionals, including pediatric dentists and orthodontists, and even worse whenever a child is using a pacifier. In this paper the authors describe a new appliance used in a very young child, which have the double purpose of stopping the pacifier use and correcting the developing malocclusion.
The Pacifier Appliance
The AMCOP™ (Cranio-Occlusal-Postural Myofunctional Activator) appliance, also known as the BioActivator is a Myofucntional appliance which have specific designs for treating different malocclusions. Between the range of BioActivator appliances available, there are the Pediatric BioActivators. Those BioActivators have two models, the D Model and the DC Model. The DC model (Fig. 1) has the characteristics of a myofunctional appliance with a lingual tag, buccal and lingual shields and a construction to properly position the mandible in relation to the maxilla. Besides that, the BioActivator DC is added with an external structure similar to a pacifier to make the appliance friendly for the young patient from the psycho-emotional point of view.
Fig. 1

In that context, the Pediatric BioActivator DC is recommended for young patients three years old or older who are using a pacifier and its use causes functional disturbances and developing a dental malocclusion. It is recommended to deliver the Pediatric BioActivator in an exchange negotiation with the child. In other words, the child must bring to the dentist all the pacifiers that they have and the dentist is going to give them the new pacifier, which the child may use at leisure, even sleeping with it! The key is the child is not having other option than using the new pacifier, the Pediatric BioActivator DC.
Case Report
A three years old girl presented to the dental clinic with a anterior crossbite tendency associated with a severe open bite and a narrow and high palate. (Fig. 2A) The dental malocclusion was associated with a lower position of the tongue at rest and tongue thrusting when swallowing. (Fig. 2B) The parents reported she was still using a pacifier and they were concerned because the child was a mouth breather and having speech issues.
Fig. 2A

Fig. 2B

The patient was asked to bring the pacifiers she was using and a Pediatric BioActivator DC was given to her as the new pacifier. (Fig. 2C) The parents were referred to a Speech Language Pathologist (SLP) to do Myofunctional Therapy to help improving the nasal breathing and the tongue dysfunction, as well to start treating the speech issues. The patient used the Pediatric BioaActivator DC for 6 months at leisure during the day time and sleeping with it. After 6 months, the open bite significantly reduced and the mouth breathing and tongue thrusting have been corrected by the action of the appliance together with the myofunctional therapy exercises. (Fig. 3A) To finalize treating the dental malocclusion the Pediatric BioActivator DC was replaced by another appliance designed specifically for open bite, the BioActivator-OPEN. (Fig. 3B) The patient used the later BioActivator appliance for 18 months. At the end of the treatment, the open bite and the anterior crossbite tendency were corrected and the patient had no oral dysfunctions. (Fig. 3C) The whole treatment was completed in the primary dentition and at the end of the treatment the structure of the mouth was the ideal for her age with no functional disorders. In that context, the habit was discouraged, the developing malocclusion was corrected, both at an early age in a friendly and non-invasive way for the young patient. The patient is being followed up until the craniofacial growth and development is completed and the permanent dentition have erupted.
Fig. 2C
Fig. 3A

Fig. 3B
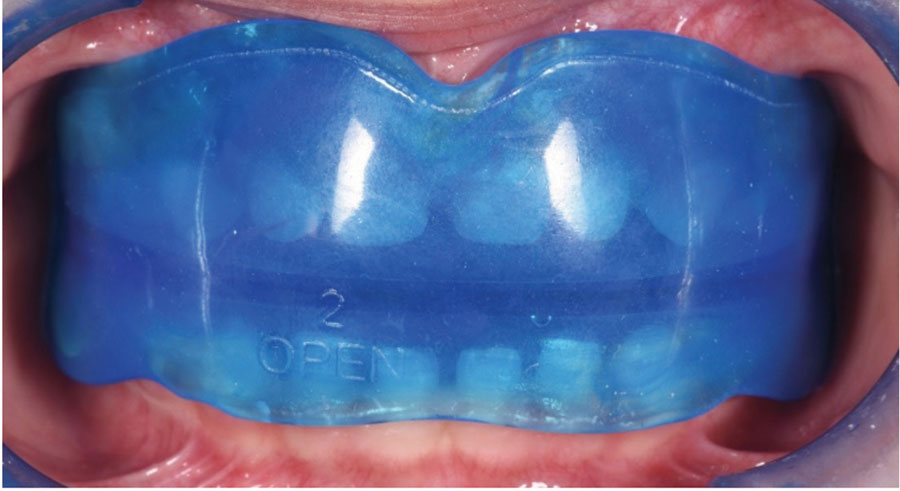
Fig. 3C

Discussion
Up to our knowledge, the myofunctional appliance presented here, the Pediatric BioActivator DC is a reliable alternative to stop the habit of using a pacifier in those patients who have continued using the pacifier to the age of three or more in a friendly way. In that context, this treatment respect the emotions of the child, who does not have to face a sudden or drastic interruption of the habit.13 It permits to the child to continue using a “pacifier” without the parents fighting with them, and at the same time start to correct the structural problems caused for the excesive use of the pacifier. The use of a myofunctional appliance must be together with myofunctional therapy exercises to facilitate nasal breathing instead of mouth breathing, as well as to correct the dysfunctions at swallowing and create a correct tongue posture at rest and lip seal.14,15
The clinical case presented here is very common in the dental clinics, but dentists and specialists did not have an appliance to deal with this habit and its consequences. The Pediatric BioActivator appliance in the models D and DC rebalance the facial and masticatory muscles and promote the correct craniofacial growth and development. In this particular case, the Pediatric BioActivator DC discouraged the pacifier use and started the correction of the severe open bite associated with the anterior crossbite tendency diagnosed initially. Then a second BioActivator indicated for open bite cases finalized correcting the dental malocclusion. The results were a combination of the effect of the appliance treating the structural and neuro-muscular problems in the patient and the guidance of the SLP with the Myofunctional exercises re-establishing correct oral functions. (Fig. 4)
Fig. 4A

Fig. 4B

Conclusions
The present report presents a clinical case of a young patient using a pacifier who was treated at an early age with the Pediatric BioActivator DC to discourage the use of the pacifier and at the same time correct the consequences correcting a severe open bite and an anterior crossbite tendency. The Pediatric BioActivator together with myofunctional therapy rises as an excellent alternative to correct structural and functional problems in young children.
Oral Health welcomes this original article.
Disclaimer: Dr. Cardarelli is the scientific adviser of Micerium SPA. (Italy) for the development of the AMCOP-BioActivator appliance. The authors declare no financial conflict of interest.
References
- Jullien, S., Sudden infant death syndrome prevention. BMC Pediatrics 2021. 21(Suppl 1): p. 320
- Hauck, F., et al., Breastfeeding and reduced risk of sudden infant death syndrome: a meta-analysis. Pediatrics, 2011. 128: p. 103-110.
- Saliba Moimaz, S., et al., Longitudinal study of habits leading to malocclusion development in childhood. BMC Oral Health, 2014. 14: p. 96.
- Nihi, V., et al., Pacifier-sucking habit duration and frequency on occlusal and myofunctional alterations in preschool children. Braz Oral Res, 2015. 29: p. 1-7.
- Verrastro, A., et al., Occlusal and orofacial myofunctional evaluation in children with primary dentition, anterior open bite and pacifier sucking habit. Int J Orofacial Myology, 2006 32: p. 7-21.
- Poyak, J., Effects of pacifiers on early oral development. Int J Orthod Milwaukee, 2006 17(4): p. 13-6.
- Pérez-Suárez, V., et al., Maternal education, dental visits and age of pacifier withdrawal: pediatric dentist role in malocclusion prevention. J Clin Pediatr Dent, 2013. 37(3): p. 315-9.
- Baccetti, T., et al., Early dentofacial features of Class II malocclusion: a longitudinal study from the deciduous through the mixed dentition. Am J Orthod Dentofacial Orthop, 1997. 111: p. 502-509.
- Ovsenik, M., et al., Follow-up study of functional and morphological malocclusion trait changes from 3 to 12 years of age. Eur J Orthod, 2007. 29: p. 523-529.
- Ramirez-Yanez, G., Is it possible to treat a malocclusion at an early age? Oral Health, 2015. 15: p. 61-62.
- Ramirez-Yañez, G., Planas direct tracks for early crossbite correction. J Clin Orthod, 2003. 37(6): p. 294-8.
- Ramirez-Yanez, G., D. Mahony, and B. Bimler, Treatment of Anterior Open Bite with the Bimler Functional Appliance: Report of Three Cases. Dentisry, 2014. 4(8): p. DOI: 10.4172/2161-1122.1000250.
- Peterson, J.J. and P. Schneider, Oral habits. A behavioral approach. Pediatr Clin North Am, 1991. 38(5): p. 1289-307.
- Van Dyck, C., et al., The effect of orofacial myofunctional treatment in children with anterior open bite and tongue dysfunction: a pilot study. Eur J Orthod, 2016. 38(3): p. 227-34.
- Marra, P., et al., Elastodontic treatment with oral bio-activators in young children. Minerva Dent Oral Sci, 2022 71(5): p. 270-276.
About the Authors:

Dr. Filippo Cardarelli graduated with honors in Dentistry and Dental Prosthetics at the University of Aquila. Specialized with honors in Orthodontics at the University of Milan. He attended numerous advanced courses in Italy and abroad.

Dr. German Ramirez-Yanez obtained his DDS degree from the Javeriana University in Colombia. He completed a Pediatric Dentistry Diploma in Mexico, and trained in Orthodontics in Brazil. He completed a Master of Dental Sciences and a PhD in Oral Biology in Australia. He also holds a Master degree focusing in Craniofacial Pain and Sleep Apnea from Tufts University, USA. Dr. Ramirez has been an academic in USA and Canada. He is a fellow of the Royal College of Dentist of Canada and has his practice in Aurora, Ontario.








