
Introduction
Provisional restorations, by definition, have a limited lifespan of utilization in fixed prosthodontic treatments. They have alternatively been referred to as “interim” or “transitional” restorations. Some clinicians and patients alike, may be tempted to minimize and devalue their importance specifically due to their transitional nature.1 By extension, it can be inappropriate to refer to provisional restorations as “temporary” restorations, a term that tends to minimize their therapeutic value and strategic role. Nothing could be further from the truth. The provisional restoration stage is an essential step in achieving consistently predictable success in the functional and esthetic outcomes in fixed prosthodontics. This article will discuss the strategic role and practical utilization of provisional restorations in a contemporary practice of prosthodontics which can help the clinician enhance his/her fixed prosthodontic therapy. Techniques of fabrication are briefly presented although more possibilities have become available to the clinician with digital technology. However, it is beyond the scope of this article to cover the provisional materials, their properties and comparisons.
Contemporary Use of Provisional Restorations & Esthetic demands
Traditionally, a fixed provisional restoration was required to protect the prepared tooth and provide basic occlusal function and esthetics, if an anterior sextant was involved. However, the contemporary requirements of provisional restorations have expanded goals in enhancing diagnostics and meeting the esthetic demands of the patient, risk management and patient education.
The addition of dental implants to a treatment plan sometimes requires an extended lifespan of provisional restorations from a few weeks to a few months. Implants in the esthetic zone often require fixed provisional restorations to optimize peri-implant soft tissue architecture and ultimately the esthetic result. In spite of significant improvement in materials and digital technology, the pressure on the clinician to achieve better, high performance and more esthetic final restorations have never been higher.
In that respect, the clinician’s skill and knowledge in diagnosis, treatment planning and expert technical execution of the provisional has become more important to meet the demands of today’s patients.2 Unfortunately, today’s high exposure to social media and “enhanced” posted images have often unreasonably increased patients’ esthetic expectations.
CLINICAL CASE 1
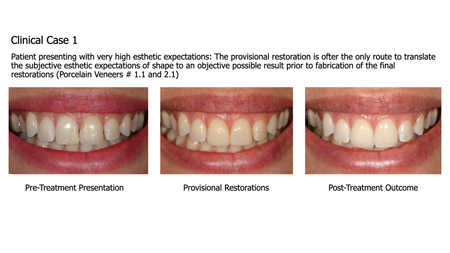
It is not unusual to observe that the quality of the provisional directly impacts the outcome of the case. In other words, the provisional is often the only route to translate the subjective esthetic expectations of the patient to a possible objective result prior to fabrication of the final restorations.
There are very few clinical situations in fixed prosthodontics that may allow the clinician to bypass a provisional restoration such as a single chairside fabrication of a porcelain restoration utilizing on site CAD-CAM technology or a single posterior implant restoration with little to no functional/esthetic risks. In most other clinical scenarios and more complex treatment plans, carefully executed provisional restorations become an essential part of treatment success.
Methods and Techniques of Fabrication
Multiple techniques exist for the fabrication of interim restorations on teeth and implants.3,4 Essentially, a matrix is required to form the external contours of the interim restoration. The internal adaptation of the interim restoration can be formed directly on the prepared tooth or teeth (the direct technique) or on a stone cast of the prepared tooth or teeth in the dental laboratory (the indirect technique). For both direct and indirect techniques, a form of matrix is required to create the external contours of the provisional restoration. The use of a custom matrix is preferable for the fabrication of multi-unit and complex provisional restorations. These matrices are fabricated from thin vacuum-formed materials or elastomeric impression materials (PVS putty). When using a vacuum-formed material is used, a duplicate stone cast of the diagnostic wax-up is required whereas a PVS putty material is convenient to use and can be adapted directly to the diagnostic wax-up. The author routinely advises the use of PVS putty for both techniques. The one cited advantage of a vacuum-form material is its transparency and ease of seating the matrix shell while visualizing positional placement. When using PVS putty, a marked reference of the midline can be very helpful especially when a full arch of prepared teeth is being provisionalized.
Direct technique: The direct technique involves the use of a mold or matrix that is related intraorally to the prepared teeth. The provisional material is mixed and placed into the matrix which is then seated over the prepared teeth and allowed to polymerize. Following working and setting times of the material being used the removal of the matrix and provisional restoration must be well timed to avoid locking. The provisional is then trimmed of any excess. It is most often necessary to reline and add to the margins of the provisional with this technique to compensate for polymerization shrinkage. The advantage of the direct technique is that it is the most efficient use of time and materials because no intermediate impression or stone cast is required. The disadvantages of the direct technique are that the freshly cut dentin and the vital pulpal tissues are exposed to the heat generated during the exothermic polymerization reaction.
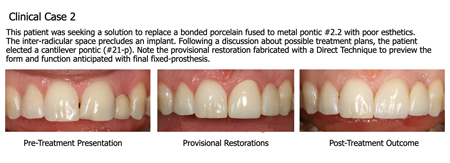
CLINICAL CASE 2
Indirect technique: This protocol is followed when the indirect technique for interim restoration fabrication is planned. After tooth preparation, an irreversible hydrocolloid impression of the prepared teeth is completed to fabricate a cast with fast setting stone or plaster. The impression is poured in fast setting plaster or stone. The silicone matrix is trial fitted to the cast, and modifications are made to the matrix or cast until complete seating of the matrix is achieved. A separating medium (petroleum jelly) is coated on the prepared teeth, adjacent teeth, and tissues on the cast. The desired provisional material is mixed and loaded into the matrix. The matrix is then positioned and seated onto the cast until complete seating of the matrix is achieved. The matrix can be stabilized with elastic bands and placed in warm water in a pressure pot to increase density and to optimize the physical properties of the provisional material. The indirect technique has the advantage of not do not polymerizing intraorally and therefore the pulpal tissues are not exposed to the exothermic polymerization reaction and free monomer. Although the indirect technique has been described as more accurate, it is not uncommon to require a reline of the restoration intraorally to adapt the margins. The main disadvantage of the indirect technique is that an intermediate impression and stone cast are required to fabricate the interim restoration, resulting in increased time and materials required for fabrication.
Indirect-direct technique (Shell provisional): A combination of the two techniques is proposed to provide a relatively atraumatic means to achieve the most accurate fitting interim prosthesis. This technique involves the fabrication of a thin shell indirectly on a minimally reduced cast of the proposed restorations. These shells are subsequently relined with the provisional restorative material intraorally over the prepared teeth. The shell provisional technique used to demand sophisticated laboratory support and was pre-operatively intensive and time consuming. In many situations, the shell was too thin or the outline overbulked to provide minimal thickness of the acrylic material to avoid fractures. However digital technology has made this approach more predictable and less intensive. Today, the modern protocol starts with the diagnostic casts, used to complete an ideal digital wax-up based on esthetics and occlusion. Then the “waxed-up” teeth are minimally “prepared digitally and the reduced amount of the wax-up is used as a quantified template to mill the provisional shells. Recent developments suggest that 3-D printing technology5 continues to improve and could soon become more predictable and accessible in daily practice. In general, reductive (milled) techniques currently offer superior finishes and physical properties over additive (3-D printed) modalities.
Periodontal versus Peri-implant tissue management.
The contours of periodontal soft tissues around natural teeth in fixed prosthodontics are significantly more predictable than around dental implant restorations. Provisional restorations can facilitate access to periodontal surgical procedures such as crown lengthening.2 The same provisional restorations may also be used as a template/reference for added accuracy in pre-prosthetic surgeries. It is common in complex fixed prosthodontic treatment to carefully plan provisional restoration selected teeth in preparation for periodontal procedures.
The advent of dental implants brings an ounce of complexity/sophistication to peri-implant soft tissue esthetic outcomes. It used to be a time when the “success “of an implant was measured based on whether it remained osseo-integrated and functional. In the mid-2000, esthetic criteria6,7 were presented as objective measures of success particularly in the esthetic zone.
Provisional restorations on dental implants allow the clinician to properly develop the adequate soft tissue architecture and the so-called Emergence Profile of the subsequent restoration. The emergence profile is not only important to achieve an acceptable pink esthetic score (PES), manage the esthetic demands of the patient but also to provide long-term health and stability of the peri-implant tissues.
CLINICAL CASE 3

For maxillary anterior implants, particularly, the provisional allows the alteration of the soft tissue to emerge from a circular cross-section of the implant platform to a truncated pseudo shape of the crown through the 3-4 mm of transgingival distance. This “developed gingival emergence profile” via a provisional restoration can then be transferred directly to the final abutment and restoration. In this regard, whenever possible, the immediate provisional restoration of implants in the esthetic zone is encouraged when conditions of primary stability are met. This approach allows the tissue to heal favorably to the desired profile around the provisional restoration acting as a scaffold. When planning implants in the esthetic zone, a simple reference rule can be applied to relate the implant platform position in relation to the esthetic gingival zenith to achieve predictable esthetic results.8 There is evidence suggesting that the use of provisional restorations on implants in the esthetic zone improves the esthetic outcome.8
High Level Esthetics: The synergized collaboration of the clinician and dental technician
It is true that an effective and sophisticated communication must exist between the clinician and technician to achieve high level esthetic results that meet or exceed the patient’s expectations. One often neglected modality at the clinician’s disposal to aid in this communication starts between the dentist and patient at the provisional stage of treatment. These provisional restorations can often be used before any irreversible treatment to preview potential esthetic outcomes and discover the limitations of specific restorative therapies. Provisional restorations can be placed and readily modified after tooth preparation but before fabrication of the definitive restoration.
In addition, the provisional can be modified until the patient is satisfied, and then the modified provisional restoration serves as the blueprint for the technician.10 It is important to note that this communication is specified to be between the clinician and his/her technician. Besides customized shade matching for anterior restorations, the technician/patient interaction should be minimized regarding form/esthetics and function which is a domain the clinician should assume the major responsibility. First, the clinician must achieve the proper form, function and esthetics with the provisional restoration: this refers essentially to occlusion and the desired three-dimensional shape/size of the restoration. With an adequate shape-approved provisional, the clinician provides valuable outline form reference on which the technician can rely to create the final restoration(s).
CLINICAL CASE 4

In the author’s opinion, dimensions and shape ought to be as accurate as possible at the provisional stage rather than allowing for subjective guesswork by the technician which may lead to less desired outcomes, costly remakes, dissatisfied patients and unshared responsibilities of who is in charge for the desired outcome. It is therefore critical that the clinician ensures he/she has the clinical expertise and skill to the provide the various methods and protocols to fabricate simple and complex provisional restorations depending on the demand of each case undertaken.
Regarding high level esthetics, the shape/form/dimension of the provisional is one significantly important step. The final elements of transition from provisional to final involves the proper choice and artistic manipulation of the definitive material in which the final restoration will be fabricated to meet the esthetic demands of hue, chroma, texture, translucency to provide the final improvement expected delivering he final restoration. At this stage, the clinician can ascertain the possibilities and limitations with the patient while discussing and confirming the same with the technician. Advising a patient that the final restoration will be “much improved” compared to the provisional is not appropriate, often leading to unreasonable patient expectations and disagreement. As a general rule, the provisional should meet the patient’s esthetic demands of the case while leaving some room for some detailed improvement when the definitive restorations are completed. Even when restorations are placed primarily for functional reasons, it is critical to address the patient’s esthetic concerns and goals. The restorative dentist must clearly understand the esthetic expectations of the patient, and the patient must understand the inherent limitations of any type of restorative therapy (both functional and esthetic). The most predictable medium for this mutual understanding is the provisional stage. When implants form part of a comprehensive plan, especially in the anterior esthetic zone, objective esthetic criteria must be used to plan and execute treatment.11,12
Communication tool between clinician and technician: practical application
A provisional restoration can provide the basic information from the clinic to the lab technician: this can be the as simple as defining the size and contour of posterior implant restorations. This approach virtually eliminates any risk of oversizing and under contouring which can result in food entrapment issues, size intolerance, cheek/tongue biting which happen to account for the broad majority of patient dissatisfaction with posterior implant crowns.
In more advanced cases, the provisional can be used to communicate the occlusal relationships and positional references essential to the case. This can be the various dimensions of adjacent teeth within a sextant as well as the esthetic midline location if the teeth being restored or missing are situated in the maxillary anterior sextant. The anterior sextant provisional also allows the clinician to evaluate the occlusion, envelope of function and phonetics while the patient test-drives the provisional.
Once functionally and esthetically approved, the information contained in the provisional can be predicably transferred to the technician via a cross-articulated cast of the provisional.
It was discussed earlier that the provisional can help transfer the emergence profile around implant-supported restorations. Today, this can be completed using a custom-impression transfer that replicated the 3-4 mm of transgingival profile or via digital scan technology to capture the emergence of the provisional when it is removed from the patient’s mouth. Using a triple-level scan (implant level, emergence profile level/soft tissue level and the provisional restoration level), the desired emergence profile can be accurately copied from the provisional and reproduced in the final abutment/crown. More sophisticated uses of the provisional restoration are their application to shape and develop pontic sites under fixed partial dentures. The intaglio surfaces related to those pontics can be copied and replicated in the final restorations without any guesswork: what you achieve and see in the provisional can be accurately reproduced within the final restoration, saving valuable time and multiple adjustments between laboratory and clinic.
CLINICAL CASE 5
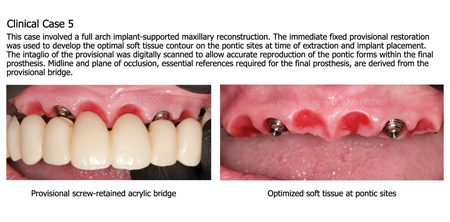
In very complex and/or full mouth reconstructions, the provisional is an accurate tool that enables cross-articulation of maxillary and mandibular master casts versus the casts of the provisional restorations at the corresponding vertical dimension and centric-relation position. Strategic segmentation of the full arch provisional restoration must be planned to allow for accurate cross-articulation. This cross-articulation reference is essential for the technician to fabricate the final restorations not only in shape/form/dimension but also in the exact location in relation to the dimensional and esthetic references, while replicating the occlusal scheme imparted/verified by the provisional restorations.
In effect, comprehensive fixed full mouth rehabilitations have many similarities to complete denture therapy13 which begins with the determination of the facial esthetic midline, followed by the maxillary incisal edge position, sagittal and frontal orientation of the plane of occlusion. With these references in place, the teeth can be positioned adequately within the arches.
Continuum of care, Practicality, Time and Cost Factors
Fixed prosthodontic treatments can have extended durations from weeks to months. Provisional restorations play a supportive role in the continuum of care by improving oral heath quality of life during active care. Provisional restorations can also improve he patient’s confidence while waiting for the definitive restorations. A common application of the continuum of care relates to fixed full arch implant reconstructions following full mouth extractions, immediate implant placement and a fixed screw-retained provisional bridges while the implants require several months for osseo-integration prior to fabrication of the definitive bridges.
The utilization and choice of provisional materials and techniques should always be as practical as possible. In other words, the clinician should elect the simple proven techniques and materials whenever possible to achieve comparably optimal results. One should not be dogmatically bound to one technique but rather be flexible to choose the most appropriate, time efficient and cost-effective technique to fabricate a provisional restoration for a given clinical case. For example, milled provisional restorations can be more costly and logistically demanding than provisionals fabricated with the direct technique matrix and hence should not be applied universally for every case.14
Fabrication and management of good provisional restorations take much of the clinician time and dedication, time well spent to set the case for predictable success. Part of treatment planning a complex case should include accounting for the significant time needed to incorporate the provisional restorations. It is often fair and necessary to add the cost of the provisional within the treatment plan as complexity increases for the case at hand.
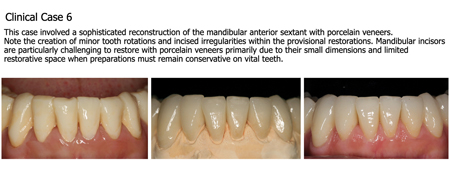
CLINICAL CASE 6
Conclusion
The important purpose and practical application of provisional restorations in fixed prosthodontics was discussed. Whether the treatment plan involves teeth supported restorations, solely implant supported restorations or a combination of both, provisional restorations are essential to achieve functional and esthetic success. The clinician must consider utilizing the provisional stage to improve and refine the final outcome: this applies to less complex to full mouth rehabilitations in which the provisional can be used effectively as a diagnostic, functional, risk management, esthetic, communication tool at different levels. Finally, provisional restorations form part of a continuum of care where the patient sees a progressive improvement from the beginning to completion of prosthodontic treatment. This continuum, in turn, can improve patient satisfaction, clinician/patient rapport and confidence leading to predictable success.
Oral Health welcomes this original article.
References
- Burns DR, Beck DA, Nelson SK; Committee on Research in Fixed Prosthodontics of the Academy of Fixed Prosthodontics. A review of selected dental literature on contemporary provisional fixed prosthodontic treatment: report of the Committee on Research in Fixed Prosthodontics of the Academy of Fixed Prosthodontics. J Prosthet Dent. 2003 Nov;90(5):474-97.
- Derbabian K, Marzola R, Donovan TE, Cho GC, Arcidiacono A. The science of communicating the art of esthetic dentistry. Part II: Diagnostic provisional restorations. J Esthet Dent. 2000;12(5):238-47.
- Gratton DG, Aquilino SA. Interim restorations. Dent Clin North Am. 2004 Apr;48(2):vii, 487-97.
- Castellon P, Casadaban M, Block MS. Techniques to facilitate provisionalization of implant restorations. J Oral Maxillofac Surg. 2005 Sep;63(9 Suppl 2):72-9.Tahayeri A, Morgan M, Fugolin AP, Bompolaki D, Athirasala A, Pfeifer CS, Ferracane JL, Bertassoni LE. 3D printed versus conventionally cured provisional crown and bridge dental materials. Dent Mater. 2018 Feb;34(2):192-200.
- Meijer HJ, Stellingsma K, Meijndert L, Raghoebar GM. A new index for rating aesthetics of implant-supported single crowns and adjacent soft tissues – the Implant Crown Aesthetic Index. Clin Oral Implants Res. 2005 Dec;16(6):645-9.
- Fürhauser R, Florescu D, Benesch T, Haas R, Mailath G, Watzek G. Evaluation of soft tissue around single-tooth implant crowns: the pink esthetic score. Clin Oral Implants Res. 2005 Dec;16(6):639-44.
- Cooper LF, Pin-Harry OC. “Rules of Six” – diagnostic and therapeutic guidelines for single-tooth implant success. Compend Contin Educ Dent. 2013 Feb;34(2):94-8.
- Furze D, Byrne A, Alam S, Wittneben JG. Esthetic Outcome of Implant Supported Crowns With and Without Peri-Implant Conditioning Using Provisional Fixed Prosthesis: A Randomized Controlled Clinical Trial. Clin Implant Dent Relat Res. 2016 Dec;18(6):1153-1162.
- Donovan TE, Cho GC. Diagnostic provisional restorations in restorative dentistry: the blueprint for success. J Can Dent Assoc. 1999 May;65(5):272-5.
- Cooper LF. Objective criteria: guiding and evaluating dental implant esthetics. J Esthet Restor Dent. 2008;20(3):195-205.
- Cosyn J, Thoma DS, Hämmerle CH, De Bruyn H. Esthetic assessments in implant dentistry: objective and subjective criteria for clinicians and patients. Periodontol 2000. 2017 Feb;73(1):193-202.
- Murrell GA. Complete denture esthetics. Dent Clin North Am. 1989 Apr;33(2):145-55.
- Strassler HE. Fixed prosthodontics provisional materials: making the right selection. Compend Contin Educ Dent. 2013 Jan;34(1):22-4.
About the Author
 Dr. Oliver Pin-Harry earned his DDS from L’Université de Montpellier, France and his MS & Certificate in Prosthodontics from the University of North Carolina at Chapel Hill, where he serves as Adjunct Assistant Professor. He is a Diplomate of the American Board of Prosthodontics, Fellow and Research Award recipient of the American College of Prosthodontists, a published author and international speaker on implants and esthetics. He maintains full-time specialty clinics at Burlington Prosthodontics & M Prosthodontics in the Greater Toronto Area.
Dr. Oliver Pin-Harry earned his DDS from L’Université de Montpellier, France and his MS & Certificate in Prosthodontics from the University of North Carolina at Chapel Hill, where he serves as Adjunct Assistant Professor. He is a Diplomate of the American Board of Prosthodontics, Fellow and Research Award recipient of the American College of Prosthodontists, a published author and international speaker on implants and esthetics. He maintains full-time specialty clinics at Burlington Prosthodontics & M Prosthodontics in the Greater Toronto Area.










