
Resin infiltration is a technique that has been available as a commercial product since 2010. The procedure consists of etching the tooth with a 15% hydrochloric acid, drying with an ethanol solution, and applying a TEGDMA-based resin infiltrant. The product (ICON, DMG) was initially developed as a treatment for incipient interproximal caries and anterior white spot lesions. Clinical experience with this technique, however, revealed that it is also effective in masking enamel discoloration of non-carious origin. This article will summarize the diagnosis of discolorations that may be treated with resin infiltration, the mechanism of action of the resin infiltration product, and a clinical protocol for the use of resin infiltration to treat an anterior tooth discoloration of developmental origin.
Diagnosis Of Lesions Treatable With Resin Infiltration
Discolorations seen on dental enamel can be attributed to either a caries-induced or non-carious etiology. Discoloration from changes in enamel formation initiated by caries are known as “white spot lesions” or “decalcification lesions.” Decalcification lesions typically are located at the cervical aspect of the tooth or surrounding orthodontic brackets because these surfaces are more likely to accumulate acid-producing plaque.1 The incidence of decalcification lesions during orthodontic treatment has been reported to be as high as 50%-97%.2,3 Decalcification lesions also may be suspected based on the patient’s caries risk. Patients with poor oral hygiene, a diet that lowers intraoral pH, a lack of fluoride, or a history of orthodontic treatment may be more likely to acquire decalcification lesions seen as white spots.4
Diagnosing the true etiology of a non-carious tooth discoloration is often difficult. Some clinicians (and patients) will attribute all non-carious tooth discolorations to fluorosis. Fluorotic lesions are brown or white discolorations caused by exposure to excess fluoride during the years of amelogenesis.
According to the Centers for Disease Control and Prevention, the prevalence of some form of fluorosis affected about 23% of Americans during period from 1999 to 2004.5 Severity and manifestation of the fluorosis stain vary, and about 7% of the population were categorized with a form of fluorosis with visibly apparent lesions (mild, moderate, or severe).2 Many discolorations are not caused by fluorosis, and some may be idiopathic white or brown enamel discolorations formed during development. Croll has coined the term “dysmineralization” to describe these disturbances in the formation of the inorganic component of enamel.6 A history of trauma, high fever episodes, or medications taken during childhood may be responsible for altering the enamel mineralization process and lead to discoloration.7 Discolorations attributed to systemic conditions should be present on all teeth mineralizing at the same time during development, whereas those caused by trauma may be limited to a single tooth. Common components of our diet can be extrinsic causes of stains, such as coffee, tea, soy sauce, red wine, or an iron supplement in vitamins, as well as some dental products such as chlorhexidine and stannous fluoride. The clinician should ask the patient about the onset of appearance of the discoloration. A discoloration that has developed during the patient’s span of memory is more likely to be extrinsic staining than is one that has to do with tooth development. In the author’s experience, treatment of extrinsic staining from diet or dental products may be accomplished with a dental cleaning or enamel microabrasion.
Resin infiltration has been shown to be able to mask discoloration from both decalcification lesions8-12 and those of developmental non-carious etiology.8,9,13-16 In the clinical trials examining resin infiltration of decalcification lesions following orthodontic brackets, lesions were infiltrated at an average time of 5 months,11 12 months,12 or 21 months9 after removal of orthodontic brackets depending on the trial. One of the trials reported that there was no association between time from debonding to infiltration with the improvement in appearance of the lesion.12
In a clinical trial, 11 out of 18 teeth (61%) with decalcification lesions were completely masked, whereas, only five out of 20 teeth (25%) with non-carious discolorations were completely masked.9 In a laboratory study, resin infiltration was shown to have variable results with different hypomineralized enamel lesions of developmental origin.17 Another clinical trial reported better masking effects for lesions attributed to fluorosis than those attributed to hypomineralization.13 A practical consideration for treating non-carious discolorations is determining the thickness of the discoloration. A thicker discoloration is more visually apparent18 and will be more difficult to infiltrate and mask. A method to help determine the thickness of a stain is to transilluminate the tooth with a dental transilluminator or light-curing unit (with proper eye protection). If the lesion becomes significantly darker with transillumination, the lesion is likely deeper within the enamel.19,20
Mechanism Of Action Of Resin Infiltration
Resin infiltration was developed as a technique to treat enamel caries. The histopathology of enamel caries occurs as acid dissolves inter-crystalline spaces within enamel.21 Since the outermost 10-30 microns of enamel is more resistant to dissolution from the presence of fluorapatite, a more porous subsurface forms.22 The principle of resin infiltration for caries arrest is to occlude the porosity formed during the caries process and prevent pathways for acid to further dissolve the tooth structure.23
The two basic steps to achieve this goal are to remove the less-porous surface layer of enamel and allow resin to infiltrate the internal enamel porosities through capillary movement. As the surface of a carious lesion may act as a barrier to resin infiltration, several preliminary studies evaluated different acid solutions for removal of the surface layer. A solution of 15% hydrochloric acid applied for 90-120 seconds was shown to almost completely remove the 45-micron thick surface layer of the lesion.24 After removing the surface layer of the carious lesion, the next step is to infiltrate resin into the porosities created during dissolution of intercrystalline enamel. Unfilled resin infiltrants have been shown to penetrate deeper into carious lesions than dental adhesives25 and a TEGDMA resin infiltrant was shown to penetrate deeper than other formulations of infiltrants.26 When applied for three minutes, the ICON TEGDMA-based infiltrant was shown to penetrate 414 microns into non-cavitated interproximal caries lesions.27
The visual change in enamel that arises from enamel caries is due to the air present in the subsurface porosities. The opaque appearance of the white spot lesion occurs because light is scattered within the body of the white spot lesion. Light scattering is caused when light interacts with two substances with different refractive indices. The refractive index of enamel (1.62-1.65) is different than that of air (1.00). Infiltration of the lesions with an infiltrant that has a refractive index of 1.52 is able to mask the lesion.28
Resin infiltration has also been shown to infiltrate hypomineralized enamel of non-carious developmental origin.17,29 A laboratory study reported infiltration to an average depth of 0.67 +/- 0.39 mm in hypomineralized enamel lesions.17
Clinical Protocol For Treatment Of An Anterior Tooth Discoloration Of Developmental Origin
A patient presented to the UAB faculty practice with esthetic concerns of white discoloration on her maxillary central incisors (Fig. 1). An exam revealed that the only discolorations on her teeth were present on her maxillary central incisors. Based on the location and appearance of the lesions, they were determined to be non-carious discolorations caused either by fluorosis or an idiopathic dysmineralization of developmental origin. A transilluminator (Microlux, Addent) was placed on the lingual aspect of the central incisors and the lesions were viewed through transillumination (Fig. 2). The lesions did not appear to become darker, and therefore were determined to be relatively shallow lesions capable of treatment with resin infiltration. The patient was presented with alternative options, including no treatment, bleaching and enamel microabrasion. The patient was given the option to bleach her teeth prior to infiltration as the use of bleaching prior to infiltration has been reported to improve the masking effect.30 The patient refused. The patient was also informed that the chance of complete or partial masking of the lesion was estimated as 25% and 35% respectively.9
Fig. 1

Fig. 2

A latex rubber dam was placed on the patient (Fig. 3). Non-latex rubber dams may also be used for the latex allergic patient or clinician, however, prolonged exposure of the infiltrant to non-latex rubber dams may cause partial dissolution of the dam. The use of isolation is critical as salivary contamination of the infiltration process decreased its effectiveness27 and exposure of hydrochloric acid to soft tissue may cause temporary bleaching and chemical burn.6
Fig. 3

The hydrochloric acid etchant from the resin infiltration system (ICON-Etch) was applied for two-minutes with a gentle scrubbing motion (Fig. 4).
Fig. 4

Afterwards, the etchant was rinsed, the tooth was dried (Fig. 5) and the ICON-dry ethanol solvent was placed on the tooth (Fig. 6). At this point the tooth was observed to determine if an acceptable color change had occurred. A clinical trial reported that re-wetting the etched lesion with ethanol (after three seconds of waiting) was able to predict the color change that would occur once the lesion was ultimately infiltrated.31 As the desired color change was not achieved, an additional two minutes of etching was performed. The lesion was dried and re-viewed (Fig. 7). Following re-wetting, the desired color change was still not achieved. A third 2 minute etching was performed. Following air drying and re-wetting, an acceptable color change was achieved (Fig. 8).
Fig. 5

Fig. 6

Fig. 7

Fig. 8

The lesions were infiltrated with the ICON-infiltrant for three minutes (Fig. 9), air dried, flossed, and light cured for 40 seconds (Fig.10). The lesion was infiltrated for an additional 1 minute and light cured for 40 seconds. The esthetic masking effect of the treatment was evident immediately upon completing the treatment (Fig. 11). Prior to removing the rubber dam, the patient was shown her teeth and she accepted the treatment outcome. In the case of more extensive staining that would not have been entirely removed, resin infiltration improves the bond to composite resin of demineralized enamel and has no negative effect on bonding to sound enamel.32,33 A clinical trial reported improved masking at one-week following treatment.9 The patient returned one-week following treatment and the masking effect looked similar to immediately after treatment (Fig. 12).
Fig. 9

Fig. 10
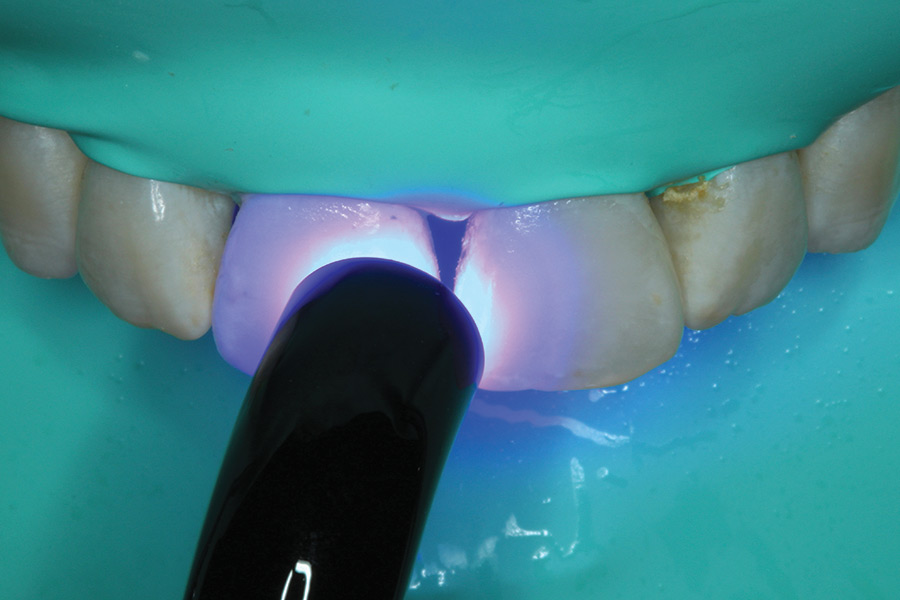
Fig. 11

Fig. 12

Conclusion
Resin infiltration may be an effective method of treatment for anterior tooth discolorations of developmental origin assuming their depth is not too great. Multiple etching steps may be needed in order to achieve the desired outcome. Several clinical trials have reported the masking effects of resin infiltration have remained unchanged at follow up times up to 12 months for non-carious lesions16 and 24-45 months for carious lesions.12
Oral Health welcomes this original article.
References
- Mizrahi E. Enamel demineralization following orthodontic treatment. Am J Orthod. 1982 Jul;82(1):62-7.
- Gorelick L, Geiger AM, Gwinnett AJ. Incidence of white spot formation after bonding and banding. Am J Orthod. 1982 Feb;81(2):93-8.
- Boersma JG, van der Veen MH, Lagerweij MD, Bokhout B, Prahl-Andersen B. Caries prevalence measured with QLF after treatment with fixed orthodontic appliances: influencing factors. Caries Res. 2005 Jan-Feb;39(1):41-7.
- Khalaf K. Factors Affecting the Formation, Severity and Location of White Spot Lesions during Orthodontic Treatment with Fixed Appliances. J Oral Maxillofac Res. 2014 Apr 1;5(1):e4.
- Beltrán-Aguilar ED, Barker L, Dye BA. Prevalence and severity of dental fluorosis in the United States, 1999-2004. NCHS Data Brief. 2010 Nov;(53):1-8.
- Croll TP. Enamel microabrasion. Hanover Park (IL): Quintessence Pub.; 1991.
- Anthonappa RP, King N. Enamel defects in the permanent dentition: prevalence and etiology. In: Drummond BK, Kilpatrick N, editors. Planning and care for children and adolescents with dental enamel defects: etiology, research and contemporary management. Berlin: Springer-Verlag; 2015. p. 15-30.
- Borges AB, Caneppele TM, Masterson D, Maia LC. Is resin infiltration an effective esthetic treatment for enamel development defects and white spot lesions? A systematic review. J Dent. 2017 [epub ahead of print]
- Kim S, Kim EY, Jeong TS, Kim JW. The evaluation of resin infiltration for masking labial enamel white spot lesions. Int J Paediatr Dent. 2011; Mar;21(4):241-248.
- Hammad SM, El Banna M, El Zayat I, Mohsen MA. Effect of resin infiltration on white spot lesions after debonding orthodontic brackets. Am J Dent. 2012 Feb;25(1):3-8
- Knösel M, Eckstein A, Helms HJ. Long-term follow-up of camouflage effects following resin infiltration of post orthodontic white-spot lesions in vivo. Angle Orthod. 2019 Jan;89(1):33-39.
- Senestraro SV, Crowe JJ, Wang M, Vo A, Huang G, Ferracane J, Covell DA Jr. Minimally invasive resin infiltration of arrested white-spot lesions: a randomized clinical trial. J Am Dent Assoc. 2013 Sep;144(9):997-1005.
- Gençer MDG, Kirzioğlu Z. A comparison of the effectiveness of resin infiltration and microabrasion treatments applied to developmental enamel defects in color masking. Dent Mater J. 2019 Mar 31;38(2):295-302.
- Mazur M, Westland S, Guerra F, Corridore D, Vichi M, Maruotti A, Nardi GM, Ottolenghi L. Objective and subjective aesthetic performance of icon® treatment for enamel hypomineralization lesions in young adolescents: A retrospective single center study. J Dent. 2018 Jan;68:104-108.
- Pan Z, Que K, Liu J, Sun G, Chen Y, Wang L, Liu Y, Wu J, Lou Y, Zhao M. Effects of at-home bleaching and resin infiltration treatments on the aesthetic and psychological status of patients with dental fluorosis: A prospective study. J Dent. 2019 [Epub ahead of print]
- Garg SA, Chavda SM. Color Masking White Fluorotic Spots by Resin Infiltration and Its Quantitation by Computerized Photographic Analysis: A 12-month Follow-up Study. Oper Dent. 2019 [Epub ahead of print]
- Crombie F, Manton D, Palamara J, Reynolds E. Resin infiltration of developmentally hypomineralised enamel. Int J Paediatr Dent. 2014 Jan;24(1):51-5.
- Abbas BA, Marzouk ES, Zaher AR. Treatment of various degrees of white spot lesions using resin infiltration-in vitro study. Prog Orthod. 2018 Aug 6;19(1):27.
- Pini NI, Sundfeld-Neto D, Aguiar FH, Sundfeld RH, Martins LR, Lovadino JR, Lima DA. Enamel microabrasion: an overview of clinical and scientific considerations. World J Clin Cases. 2015 Jan 16;3(1):34-41.
- Sundfeld RH, Sundfeld-Neto D, Machado LS, Franco LM, Fagundes TC, Briso ALF. Microabrasion in tooth enamel discoloration defects: three cases with long-term follow-ups. J Appl Oral Sci. 2014 Jul-Aug;22(4):347-54.
- Kidd EA, Fejerskov O. What constitutes dental caries? Histopathology of carious enamel and dentin related to the action of cariogenic biofilms. J Dent Res. 2004;83 Spec No C:C35-8.
- Larsen MJ. Chemical events during tooth dissolution. J Dent Res. 1990 Feb;69 Spec No:575-80; discussion 634-6.
- Paris S, Meyer-Lueckel H, Kielbassa AM. Resin infiltration of natural caries lesions. J Dent Res. 2007 Jul;86(7):662-6.
- Meyer-Lueckel H, Paris S, Kielbassa AM. Surface layer erosion of natural caries lesions with phosphoric and hydrochloric acid gels in preparation for resin infiltration. Caries Res. 2007;41(3):223-30.
- Meyer-Lueckel H, Paris S. Improved resin infiltration of natural caries lesions. J Dent Res. 2008 Dec;87(12):1112-6.
- Meyer-Lueckel H, Paris S. Infiltration of natural caries lesions with experimental resins differing in penetration coefficients and ethanol addition. Caries Res. 2010;44(4):408-14.
- Meyer-Lueckel H, Chatzidakis A, Naumann M, Dörfer CE, Paris S. Influence of application time on penetration of an infiltrant into natural enamel caries. J Dent. 2011 Jul;39(7):465-9.
- Paris S, Schwendicke F, Keltsch J, Dörfer C, Meyer-Lueckel H. Masking of white spot lesions by resin infiltration in vitro. J Dent. 2013 Nov;41 Suppl 5:e28-34. doi: 10.1016/j.jdent.2013.04.003.
- Schnabl D, Dudasne-Orosz V, Glueckert R, Handschuh S, Kapferer-Seebacher I, Dumfahrt H. Testing the Clinical Applicability of Resin Infiltration of Developmental Enamel Hypomineralization Lesions Using an In Vitro Model. Int J Clin Pediatr Dent. 2019 Mar-Apr;12(2):126-132.
- Schoppmeier CM, Derman SHM, Noack MJ, Wicht MJ. Power bleaching enhances resin infiltration masking effect of dental fluorosis. A randomized clinical trial. J Dent. 2018 Dec;79:77-84.
- Kobbe C, Fritz U, Wierichs RJ, Meyer-Lueckel H. Evaluation of the value of re-wetting prior to resin infiltration of post-orthodontic caries lesions. J Dent. 2019 [epub ahead of print]
- Borges AB, Abu Hasna A, Matuda AGN, Lopes SR, Mafetano APVP, Arantes A, Duarte AF, Barcellos DC, Torres CRG, Pucci CR. Adhesive systems effect over bond strength of resin-infiltrated and de/remineralized enamel. F1000Res. 2019 Oct 11;8:1743.
- Wiegand A, Stawarczyk B, Kolakovic M, Hämmerle CH, Attin T, Schmidlin PR. Adhesive performance of a caries infiltrant on sound and demineralised enamel. J Dent. 2011 Feb;39(2):117-121.
About the Authors
 Nathaniel C. Lawson is the Director of the Division of Biomaterials at the University of Alabama at Birmingham School of Dentistry and the program director of the Biomaterials residency program. He works as a general dentist in the UAB Faculty Practice.
Nathaniel C. Lawson is the Director of the Division of Biomaterials at the University of Alabama at Birmingham School of Dentistry and the program director of the Biomaterials residency program. He works as a general dentist in the UAB Faculty Practice.
 Dr. Celin Arce is a board certified prosthodontist. He received his dental degree from University Latina of Costa Rica and completed residency in Advanced Prosthodontics at the University of Alabama at Birmingham, and Master of Science in Clinical Dentistry. He is a Diplomate of the ABP and Fellow of the American College of Prosthodontists. He is currently Assistant Professor of the Restorative Sciences Department at the University of Alabama at Birmingham School of Dentistry.
Dr. Celin Arce is a board certified prosthodontist. He received his dental degree from University Latina of Costa Rica and completed residency in Advanced Prosthodontics at the University of Alabama at Birmingham, and Master of Science in Clinical Dentistry. He is a Diplomate of the ABP and Fellow of the American College of Prosthodontists. He is currently Assistant Professor of the Restorative Sciences Department at the University of Alabama at Birmingham School of Dentistry.










