
Introduction: The present study aims to assess the link between the features of the dental follicle and the resorption of the incisors close to the impacted canines using three-dimensional imaging.
Methods: The study was conducted on 79 patients with 102 impacted maxillary canines. The age range was 12-48 years, with an average of 20.09 years ± 7.26 and a median of 18 years. All computed tomography data collections for extended diagnostic purposes, from the submental area to the orbital roofs, were performed using a new generation multi-slice helical scanner with 64 continuously revolving bars, Hitachi’s “Scenaria” Multislice CT model Medical Holding Systems.
Results and discussion: For the distribution of cases based on follicle width, we discovered a considerable variance in follicle width ranging from 0.5 to 8 mm, with 44 percent of the follicles falling within the normal width limits.
The link between follicular closeness and resorption was statistically meaningful. There was no significant correlation discovered between follicle width and the gender factors, side of impaction, and location of maxillary impacted canines.
Dental eruption is connected to the dental follicle and is influenced by environmental, metabolic, and cellular activities.1,2 The pericoronal pocket, also known as the dental follicle, is the region around the crowns of impacted teeth. (Fig. 1) On periapical or panoramic radiographs, the thickness of the dental follicle can exceed 5.6 mm. The epithelial structures of the dental follicle constantly release epidermal growth factor (EGF, red arrows) into the connective tissue, promoting pericoronal bone resorption, which is required for the dental eruption to occur. (Fig. 2) The cementoblasts die in place and the root is resorbed (RR) when the course of an uneven tooth compresses the vasculature of the surrounding teeth’s periodontal ligament (PL).3
Fig. 1

Fig. 2

The image, thickness, contour, and boundaries of the follicle should be homogeneous, with borders with adjacent bone defined by a uniform and continuous radiopaque line, as these may indicate an odontogenic tumor, and a contour and uniform thickness distributed symmetrically around the dental crown ranging from 1 mm to less than 5.6 mm.
Beyond these boundaries, a dentigerous cyst or other follicular lesions should be suspected. Some computed tomography (CT) investigations suggest that the size of the dental follicles of maxillary impacted canines may be responsible for the resorption of neighboring teeth, particularly the incisors.4,5 Bishara et al6 discovered that the canine follicle was 3 to 5 mm broad in 19% of cases, smaller than 3.0 mm in 81% of cases, and greater than 3.0 mm in 23% of participants with root resorptions. However, the study was unable to demonstrate a link between follicle width and resorption. They believe that while closeness may not induce surface resorption in and of itself, it may be sufficient to activate osteoclastic processes, and that crown-root contact may be the cause of cement necrosis. (Fig. 3)
Fig. 3

According to Ericson et al.7, there is no connection between the width or shape of the dental follicle and the resorption of adjacent permanent incisors, and root resorption of maxillary permanent incisors is most likely caused by physical contact between the incisor and canine during the eruption process. However, there was a substantial link between the existence of resorption and the canines’ closeness to the central and lateral incisors. (Fig. 4)
Fig. 4

A distance of less than 1 mm between the affected canine and a nearby root, according to Yan et al.12 is a risk factor for root resorption, and the canine’s migration throughout the root formation process is likely to exacerbate this risk.
Hence, the present research aims to check if there was a link between the follicular features of the impacted maxillary canines (size, position, shape, and proximity) and the resorption of the incisors close to the impacted canines using three-dimensional CT imaging.
Methods
This prospective study was based on CT scans of 79 people and a total of 102 impacted canines. Patients were picked from the department of dental surgery (dentofacial orthopedic department CHU of Oran) and the department of stomatology at the regional military university hospital of Oran. All CT scans were collected using the same CT device and assessed by a single investigator in all three planes (sagittal, axial, and coronal). According to Cernochová et al.,6 the descriptive information of the samples (age, sex), the side affected by the inclusion (right or left), location (vestibular, central, or palatal), and the size of the follicle (distance in mm measured from the crown to the periphery of the follicle) must be less than 3 mm for normal size and equal to or greater than 3 mm for follicles considered hypertrophied.6 On the CT scans, the degrees of root resorption of the lateral or central incisors were evaluated (the categorization of resorption was recognized by the numbers 1 to 4, as described in the literature). Grade 1 shows no resorption, grade 2 represents mild resorption (up to half the dentin thickness) while grade 3 indicates moderate resorption (very close to the pulp), and grade 4 shows severe resorption (the pulp is exposed).
The statistical tests applied in the present study were as follows:
- For the descriptive variables, we used percentages; for the qualitative variables, we used percentages.
- The percentages were compared
- using the chi-squared test (χ2) and Fisher’s exact test, with a risk a = 5%.
- The Spearman correlation test was used to determine the relationship between two quantitative variables.
Results
The resorption of teeth adjacent to impacted canines was noted at 57% including 39 lateral incisors (67.24%) and seven central incisors (12.06%). Simultaneous resorption of the lateral and central incisors was observed in 8.62%, and that of the lateral incisor and the first premolar in 3.44%. We discovered a positive and significant connection (p < 0.01) between the degree of canine closeness and the degree of neighboring tooth resorption.
The distribution of neighboring tooth resorptions was mostly at the apical third (41.38%), followed by the middle third (32.75%). In five cases, resorption damaged both the cervical and middle thirds, and in four cases, both the middle and apical thirds.
The asymmetric form of the canine follicle is found in 52.95% of the distributions based on the shape of the canine follicle. (Fig. 5)
Fig. 5A

Fig. 5B

Table 1: Distribution according to the proximity of the canine follicle to the adjacent teeth.
| The proximity of the follicle to the adjacent tooth | Cases | Pourcentage |
| In close contact with the lateral incisor | 45 | 65.2% |
| In close contact with the central incisor | 10 | 14.5% |
| In contact with the central and lateral incisors | 9 | 13% |
| In contact with the lateral incisor and premolar | 4 | 5.8% |
| In close contact with the premolar | 1 | 1.5% |
| Total | 69 | 100.0% |
There was no follicle or the follicles were not assessable in four cases (3.92%). Approximately 44% of canine follicles studied were within acceptable width limits ranging from 0.5 to 8 mm, while the rest 56% were deemed enlarged (≥ 3mm). (Fig. 6)
Fig. 6
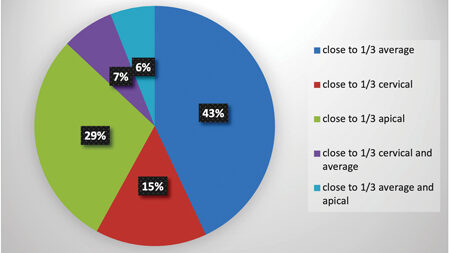
The closeness of the follicle to the neighboring tooth was discovered in 69 cases, with the lateral and central incisors accounting for 65.2% and 14.5% of the cases, respectively. In 13% of cases, it was simultaneous at the level of the central and lateral incisors. This closeness was at the level of the average third of the neighboring tooth in 43% of total cases.
The follicles were separated from the neighboring teeth in 33 cases (including the four absent follicles).
The present study revealed that 45 (65.2%) of the teeth near the follicles had root resorptions. The closeness of the canine follicle and the resorption of the neighboring tooth have a statistically significant correlation (p = 0.02 and x2 = 4.76).
We note that the asymmetric form of the follicle was associated with resorptions was estimated to be 63.6% while the symmetrical form was associated with resorptions is 51.2%, but there is no statistically significant correlation (p= 0.2 and x2 = 1.54) between the shape of the canine follicle and the presence of resorption.
We note that 61.8% of the 57 cases of root resorptions were near a follicle of a size greater than or equal to 3 mm, but there is no statistically significant correlation (p = 0.4 and x2 = 0.68) between the relative width of canine follicles and root resorption.
Fig. 7
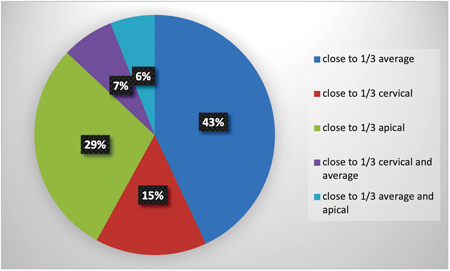
Table 2: The correlation between follicular proximity and resorption
| Proximity | Root resorption | Root resorption | Total | p |
| Yes | No | |||
| Yes | 45 (65.2%) | 24 (34.8%) | 69 | 0.02 |
| No | 12 (41.38%) | 17 (58.62%) | 29 | 0.02 |
| Total | 57 | 41 | 98 | 0.02 |
Discussion
The width of the follicles varied greatly in our research, with 56 % classified as hypertrophied (≥ 3 mm). According to the findings, there is no statistically significant correlation between the relative width of canine follicles and root resorption, which is consistent with earlier research.7,10-14 The tooth follicle width of impacted maxillary canines did not provide a danger of resorption on neighboring incisors in our investigation.
The asymmetric form of the follicle was more commonly linked with resorptions, although the correlation between the shape of the canine follicle and the incidence of resorption was not statistically significant.
We discovered a significant correlation between the closeness of the canine follicle and neighboring tooth resorption, which correlates to the findings of Yan et al.12 The strong connection found in this study between incisor root resorption and contact with the erupting canine supports the theory7 that physical pressure on hard tissue induces cellular activity in the periodontal membrane and the formation of dentinoclasts and osteoclasts, triggering incisor root resorption.
Fig. 8A

Fig. 8B

Fig. 9

Table 3: The correlation of canine follicle morphology and the prevalence of resorption
| Canine follicle shape | Root resorption | Root resorption | Total |
| Yes n (%) | No n (%) | ||
| Symmetric shape | 22 (51.2) | 21 (48.8) | 43 |
| Asymmetrical shape | 35 (63.6) | 20 (36.4) | 55 |
| Total | 57 | 41 | 98 |
Table 4: Correlation between canine follicle size and root resorption
| Canine follicle size | Root resorption | Root resorption | Total |
| Yes n (%) | No n (%) | ||
| Less than 3mm | 23 (53.5) | 20 (46.5) | 43 |
| Greater than or equal to 3mm | 34 (61.8) | 21 (38.2) | 55 |
| Total | 57 | 41 | 98 |
Conclusion
The mechanism of root resorption linked with inclusion, as well as the components involved in the process, remain unknown. The close physical contact between the incisor and the canine, as well as the imposed pressure, are likely to promote root resorption of the central and lateral incisors during the eruption of the maxillary canines. Despite the radiation and added cost, three-dimensional imaging might be a viable technique for assessing impacted tooth location and distance from neighboring structures to aid in later treatment planning.
Oral Health welcomes this original article.
Conflicts of Interest: In this work, the authors declare no conflicts of interest.
References
- S. Ericson and K. Bjerklin, “The dental follicle in normally and ectopically erupting maxillary canines: a computed tomography study,” The Angle Orthodontist 2001; 71(5) : 333-42.
- Ruiye Bi and al . Function of Dental Follicle Progenitor/Stem Cells and Their .Potential in Regenerative Medicine: From Mechanisms to Applications . Biomolecules 2021; 11: 1-18.
- A .Consolaro Orthodontic traction : Possible consequences for maxillary canines and adjacent teeth Part 1: Root resorption in lateral incisors and premolars. Dental Press J Orthod 2010; 15(4):15-23.
- S. Ericson and P. J. Kurol, “Resorption of incisors after ectopic eruption of maxillary canines : a CT study ”The Angle Orthodontist, 2000 ; 70 (6) : 415–23.
- S. Ericson and J. Kurol, “Resorption of maxillary lateral incisors caused by ectopic eruption of the canines. A clinical and radiographic analysis of predisposing factors, American Journal of Orthodontics and Dentofacial Orthopedics, 1988 ; 94 (6) 503-13.
- P. Cernochová, P. Krupa, L.Izakovicova-Holla. Root resorption associated with ectopically erupting maxillary permanent canines : a computed tomography study. Eur J Orthod 2011;33:483-91.
- S Ericson, K. Bjerklin, and B. Falahat . Does the Canine Dental Follicle Cause Resorption of Permanent Incisor Roots ? A Computed Tomographic Study of Erupting Maxillary Canines, The Angle Orthodontist 2002 ; 72(2) : 95–104.
- Peteris Sosars, Gundega Jakobsone . Precise Assessment of Incisor Root Resorption Caused by Maxillary Impacted Canines. Stomatology Papers / RSU ; 2015 : 85-7.
- Liu D. G., Zhang W. L., Zhang Z. Y.et al . Localization of impacted maxillary canines and observation of adjacent incisor resorption with cone-beam computed tomography. Oral Surg Oral Med Oral Path Oral Radio Endod, 2008; 105 (1): 91-8.
- Alqerban A., Jacobs R., Lambrechts P., Loozen G., Willems G. Root resorption of the maxillary lateral incisor caused by impacted canine: a literature review. Clin Oral Investig, 2009;13(3): 247-55.
- Elhan Metin Dalsuyu And Al The Relationship Between Dental Follicle Width And Maxillary Impacted Canines Descriptive And Resorptive Features Using Cone-Beam Computed Tomography Bio Med Research International Volume 2017, ID 2938691, 5.
- Yan B., Sun Z., Fields H., Wang L. Maxillary canine impaction increases root resorption risk of adjacent teeth: a problem of physical proximity. Am J Orthod Dentofac Orthop 2012; 142 (6): 750–57.
- A. Consolaro, O. Hadaya, T. Maeshiro Estorce.. Why canines induce resorption of neighboring roots? An imaging correlation. Dental Press J Orthod. 2019 ; 24(1):27-33.
- Walker L., Enciso R., Mah J. Three-dimensional localization of maxillary canines with cone-beam computed tomography. Am J Orthod Dentofac Orthop 2005;128 (4): 418–23.
About the Authors

Sonia Terbeche is associate professor in dentofacial orthopedics at the military regional university hospital of Oran (HMRUO). E-mail: soniaterbeche@yahoo.fr Address: Military hospital city; block 3 App 6, Almond trees Oran.

Yousfi Kheira is associate professor in periodontics. Stomatology Service/ Regional Military University Hospital of Oran.

Saidi Messaoud is assistant professor in dentofacial orthopedics. Stomatology Service / Regional Military University Hospital of Oran.

Ahmed Fouatih Noureddine is head of the Dentofacial Orthopedics Department and Head of the Dental Medicine Department, CHU Oran. Dentofacial orthopedic service / University Hospital of Oran.










