
Introduction
Er,Cr:YSGG laser has been chosen to perform the apicoectomy1,9,13 as an alternative for the use of a scalpel and rotary instruments due to the laser’s precision, lack of vibration16,17 and lack of microfracture occurrence on hard tissues, such as bone and root. Additionally, laser apicoectomy had the benefit of less post-operative discomfort1, capability to remove smear2,4 and to effectively reduce bacterial accumulation.3-5,7,7,11-14 For both patients and doctors, use of the Er,Cr:YSGG laser offers less stress during the procedure, as the laser surgical site results in less bleeding and provides a cleaner and clearer surgical field to allow the procedure to be performed with more efficiency and less time.
Case Report
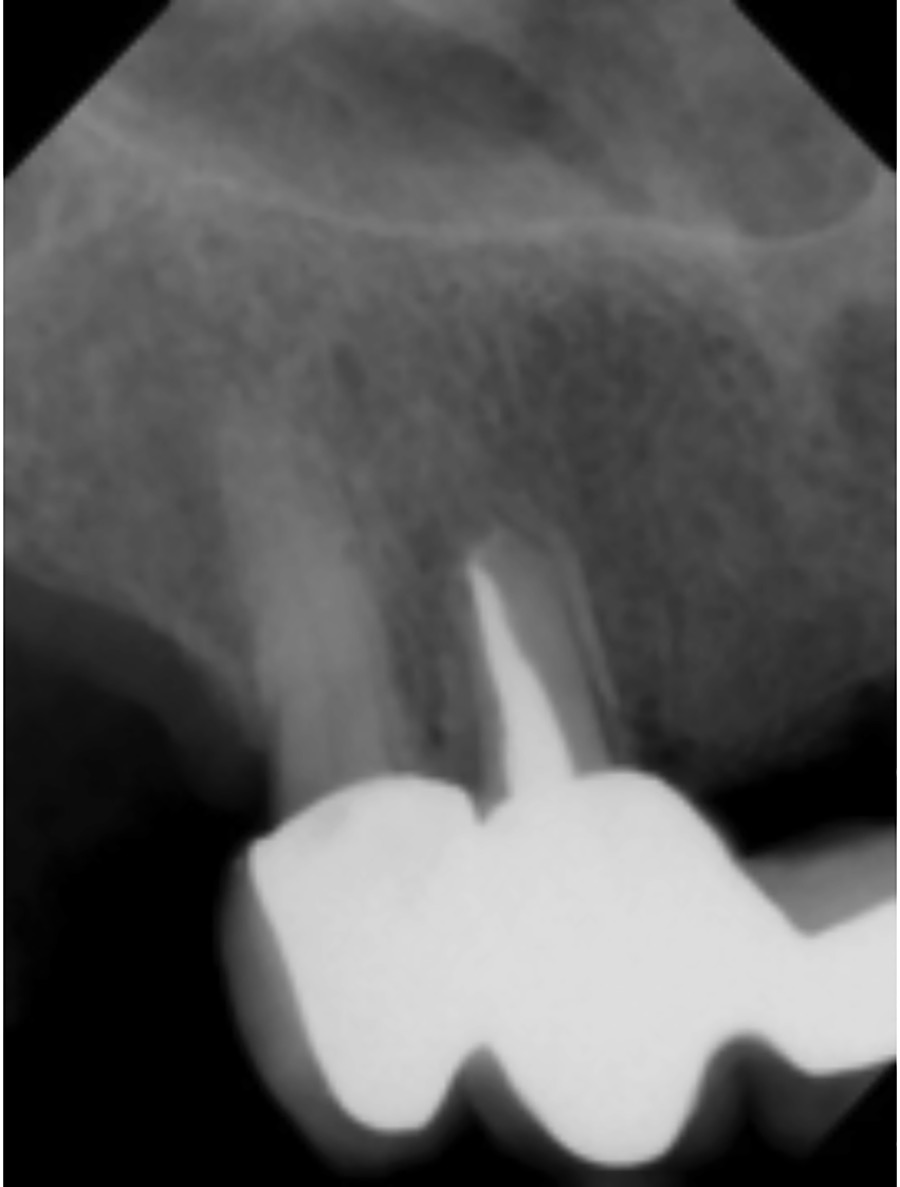
An 85-year-old female presented with pain and swelling of her maxillary right cuspid. Clinical exam revealed that tooth #6 (13) had swelling close to the apex. The tooth was painful to percussion and palpation. A periapical X-ray revealed bone resorption around the apical area of tooth #6 (13). It was confirmed that a periapical abscess was the cause of patient’s pain and swelling.
Upon further examination, tooth #6 (13) was an abutment of eight units of fixed porcelain-fused-to-metal bridge from #5 (14) to #12 (24). The periodontal condition was healthy, and the condition of this multi-unit fixed bridge of 10 years was acceptable. No mobility was found in any of the abutments including the abscessed tooth #6 (13)(Figs. 1 & 2).
Fig. 1
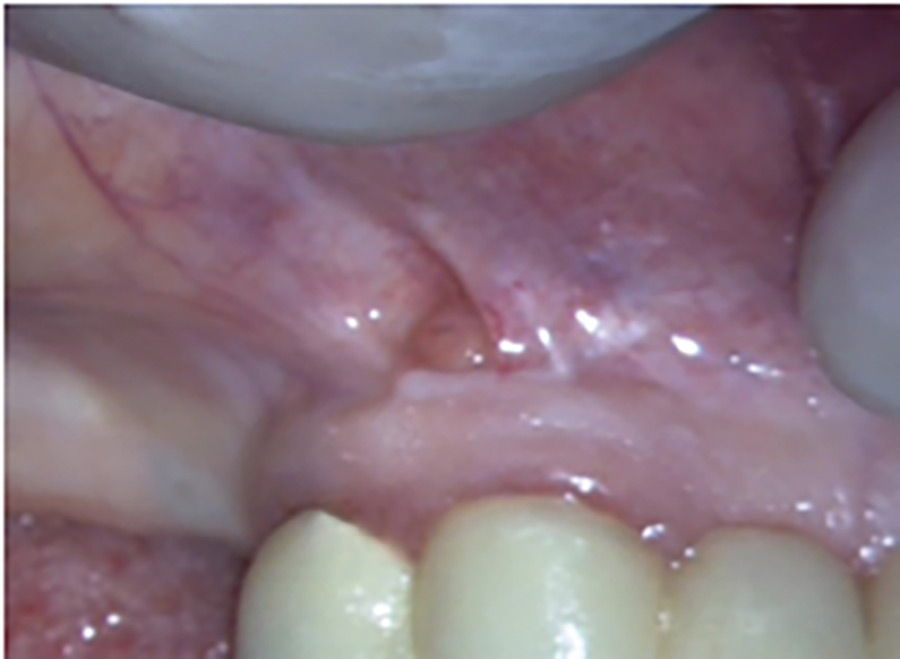
Fig. 2
No outstanding medical or dental history was noted, as indication not to consider performing an apicoectomy on tooth #6 (13) , as a resolution procedure for damage repair and salvage of the fixed prosthesis. The patient was treated as planned with an apicoectomy consisting of a retrofill with MTA (mineral trioxide aggregate). In addition, the Er,Cr:YSGG laser was used to perform the endodontic surgery.
Materials
The laser:
- Er,Cr:YSGG
- Wavelength: 2780nm
- Manufactured by Biolase Technologies, Inc., Irvine, California.
The model:
- Waterlase MD System
- Gold Hand Piece
- MZ5 Tip – 14 mm long
Treatment
Local anesthetic was administered to the surgical area from tooth #5 (14) to #9 (21) using two carpules of 2% lidocaine with 1:100,000 epinephrine. An incision was made using the Er,Cr:YSGG laser, Waterlase MD system, and the gold handpiece with a MZ5-14mm long fiber tip.15 The setting was 2.50 Watts, 30Hz, 15% water, 11% air, H mode. A trapezoid flap was made at the mucogingival junction area several millimeters around the sinus tract opening. The vertical relief of the flap was made mesial to tooth #7 (12) and distal to tooth #5 (14) (Fig. 3).
Fig. 3

After the lesion was exposed by using a periosteal elevator, part of the periapical abscess showed a bone defect in the periapical area. The periapical granuloma was revealed more clearly by using the Er,Cr:YSGG laser to remove a portion of bone at the osseous crypt opening (Fig. 4).
Fig. 4

The laser setting used for bone ablation was 5.00 Watts, 20Hz, 50% water, 70% air, H mode. Some granulomatous tissue was removed by the laser (Fig. 5).
Fig. 5

The setting for granuloma removal was 3 Watts, 30Hz, 15% water, 11% air, H mode. Some carbonized tissue was noted in the surgical site. The carbonized spot was removed by the laser under the hard tissue setting during the final debridement of the apex and the osseous crypt (Fig. 6).
Fig. 6

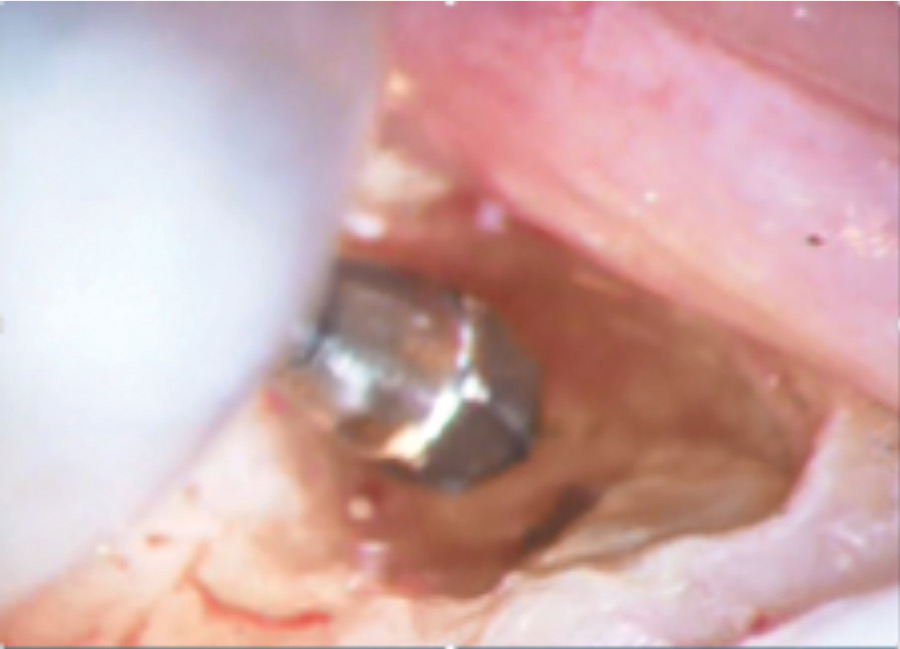
The endodontic post perforation past the apex was noted. The micro-leakage at the apex was presumed to be the main cause of the periapical abscess (Fig. 7).
Fig. 7

About 3 mm of the apex was ablated, followed by Er,Cr:YSGG laser apicoectomy. The settings were 4.00 Watts, 20 Hz, 50% water, 70% air, H mode. The extruded post was cut off by use of a high-speed electric handpiece using a SS#556 and a SS#2 round bur (Fig. 8).
Fig. 8
This was followed by a retrograde preparation at the apex using an endodontic surgical Cavitron18,20,21 and endodontic Cavitron tip (Fig. 9).
Fig. 9

The smear layer was then removed by using the Er,Cr:YSGG laser (Fig. 10).
Fig. 10

The setting for smear removal was 2 Watts, 20Hz, 50% water, 70% air, H mode. MTA (mineral trioxide aggregate) was placed as the retrograde material using a dry 2×2 gauze placed with pressure at the periapical area for five minutes, to allow the MTA to set before carving and cleaning. A 4-0 resorbable Vicryl sutures with mattress suture technique were used to close the surgical site. A biologic ‘band-aid’ procedure was performed using the Er:Cr:YSGG. In the planning of the biologic ‘band-aid’ procedure, we were expecting the following: hemostasis, disinfection, de-epithelization (reducing the chance for future smear formation), and low level laser therapy (LLLT). LLLT potentially reduces swelling and pain while promoting faster healing22 (Figs. 11A & B).
Fig. 11A

Fig. 11B
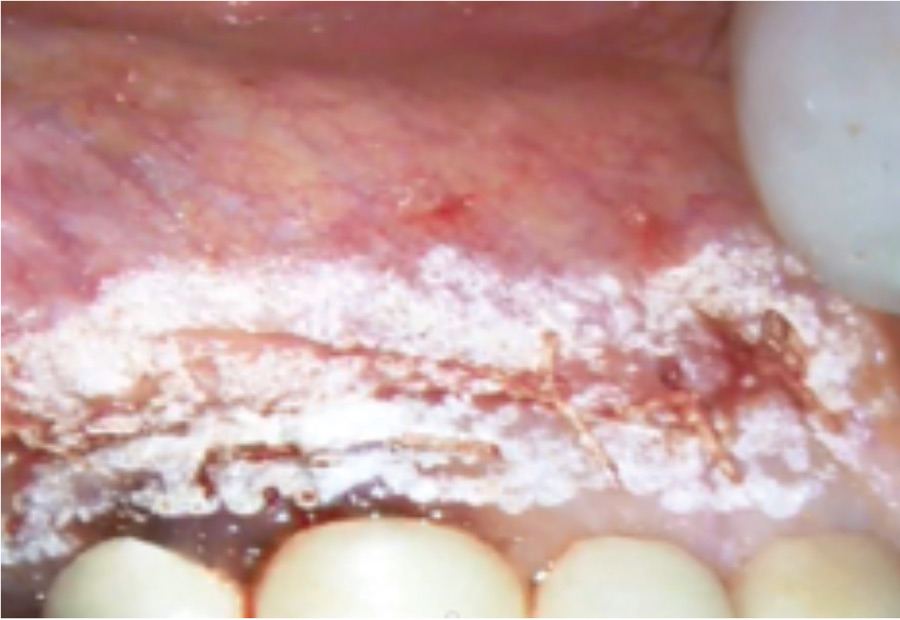
The laser setting for the biological ‘band-aid’ was 1.25 Watts, 30Hz, 0% water, 11% air, H mode, defocused at 5mm and using a fast-moving tip. Firm hemostasis was obtained, and the patient was given an antibiotic (Keffex 500mg, dispense #28, one capsule q.i.d) and some pain medication (Vicodin, one tablet every six hours as needed for pain) (Fig. 12).
Fig. 12

Fig. 13A

Fig. 13B

Post-operative instructions were provided to the patient similar to instructions provided following a tooth extraction. The patient was given appointments for a post-operation check-up and suture removal.
Fig. 14

Results
At the three day post-operative re-evaluation examination, clinical observation revealed that the surgical site healed extremely well with no evidence of secondary bleeding, infection or swelling. Patient did not report or show any indications of discomfort. The periapical X-ray at four years shows good periapical healing with good apical seal and evidence of bone regeneration at the apex.
Fig. 15A

Fig. 15B

Discussion
An apicoectomy using the Er,Cr:YSGG laser was used to treat an abscessed maxillary cuspid that had a perforated endodontic post. As a result of this perforation, a periapical micro-leakage and failure of root canal therapy occurred. The main reason to select the endodontic surgery was based on the difficulty of accessing the apical area via the root canal. These conditions have been reported to result in the persistence of the infection, which may interfere with resolution of the apical healing process.13
Er,Cr:YSGG laser application shows multiple convincing benefits compared to the standard of care for endodontic surgery. The standard procedure, including creating an incision for flap, bone ablation to reveal the apex, removal of granulated tissues, cutting 3 mm of the apex, removing smear and debris, and removing 3 mm of the extruded endodontic post using a rotary instrument often results in excessive pain and bleeding during and following the surgical procedure. Alternatively, laser incision reduces bleeding. Laser bone ablation results in less bleeding and a lack of microfractures in bone surfaces. Laser removal of granulation is efficient, clean, and less time consuming. Laser sectioning of the apical 3 mm is efficient, precise and does not create microfractures. Retrograde cavity preparation via laser results in a smear-free, debris-free cavity. The resulting surgical area is also microfracture-free prior to placement of MTA, which is allowed to set before closure of the surgical site. All the benefits of using the Er,Cr:YSGG laser are expected to improve the chance of success of an apicoectomy procedure and reduce potential pain and infection for patients during and post-surgery.
Fig. 16A

Fig. 16B

Fig. 17A

Fig. 17B

Conclusion
The FDA approved using an Er,Cr:YSGG laser to perform an apicoectomy in 2003. This procedure involves flap incision, bone removal, root sectioning, granulation tissue removal, and retrograde cavity preparations. All procedures are performed in a small surgical area of several square millimeters. The Er,Cr:YSSG laser is safe for performing multiple tissue ablation and cleaning in a tiny restrictive surgical site.22 This laser also has the potential to be used in a more extensive surgical procedures, such as an osseous periodontal surgery, single or multiple extractions, or in procedures used for salvaging an implant. This laser has been shown to be safe in performing these challenging procedures, providing such benefits as reduced bleeding, swelling, postoperative pain, and post-operative complications. It’s been almost 15 years since the FDA approved this laser to perform these procedures, which leads us to ask, “Why haven’t more clinicians adopted this technique to provide their patients with an improved standard of care, resulting in less pain, inflammation, and risk of infection?”
Oral Health welcomes this original article.
References
- Aparecida Maria, ‘Influence of the Parameters of the Er,Cr;YSGG Laser on the Apical Sealing of Apicoectomized Teeth’. Lasers Med Sci (2011) 26:433-438.
- American Association of Endodontists (AAE) Position Paper adopted 4/2/2000 on the use of Lasers in Dentistry.
- Gordon et. al., The Er,Cr;YSGG Laser with Radial Emitting Tip has a Significant Antimicrobial Effect on Dentinal Tubules Infected with E. Faecalis. JADA 2007:138(7):922-1002.
- Wanda Gordon, DMD, Vahid A. Atabakhsh, DDS, Fernando Meza, DMD, Aaron Doms, DDS, Roni Nissan, DMD, Ioana Rizoiu, MS and Roy H. Stevens, DDS, MS. The antimicrobial efficacy of the erbium, chromium:yttrium-scandium-gallium-garnet laser with radial emitting tips on root canal dentin walls infected with Enterococcus faecalis. JADA 2007; 138(7): 992-1002.
- U. Schoop, A. Barylyak, K. Goharkhay, F. Beer, J. Wernisch, A. Georgopoulos,W. Sperr, A. Moritz. The impact of an erbium, chromium: yttrium-scandium-gallium-garnet laser with radial-firing tips on endodontic treatment. Lasers in Medical Science; DOI 10.1007/s10103-007-0520-4.
- Ulrich Schoop, DDS, MD, Kawe Goharkhay, DMD, MD, Johannes Klimscha, DMD, MD, Manuela Zagler, DMD, Johann Wernisch, TD, PhD, Apostolos Georgopoulos, MD, PhD, Wolfgang Sperr, DDS, MD, PhD and Andreas Moritz, DMD, MD, PhD. The use of the erbium, chromium:yttrium-scandium-gallium-garnet laser in endodontic treatment. The results of an in vitro study. JADA 2007;138(7): 949-955.
- Gutknecht N., et. al. Photomed Laser Surg 2016; 34:11-6. The Bacterial effect of 2780 and 940nm laser irradiation on E. faecalis in Bovine Root Dentin Slices of Different Thicknesses.
- Schoop, U, Kluger, W, Moritz, A. Bactericidal effect of different laser systems in the deep layers of dentin. Lasers Surg Med 2004; 35:111–116.
- Angiero, F MD DDS. Apicoectomies with the Erbium Laser: A Complementary Technique….
- Blum, Y.J., and Abadie, M.J, (1997). Study of the Nd:YAP laser. Effect on canal cleanliness. J. Endod. 23, 669-675.
- Eldinez, A.U., Ozer, F., Hadimli, H.H., and Erganis, O. (2007). Bactericidal efficacy of Er,Cr:YSGG laser irradiation against Endericiccus faecalis compared with NaOCL irrigation: an ex vivo pilot study, Int. Endod. J. 40, 112-119.
- Wang, Q.Q., Zhang, C.F., and Yin, X.Z. (2007). Evaluation of the bactericidal effect of Er,Cr:YSGG and Nd:YAG lasers in experimentally infected root canals. J. Endod. 33, 830-832.
- Komori, T., Yokoyama, K., Tarato, T., and Matsumoto, K. (1997). Clinical application of the erbium:YAG laser for apicoectomy. J. Endod. 23, 748-750.
- Ishizaki, N.T., Matsumoto, K., Kimura, Y., et. al. (2004). Thermographical and morphological studies of Er,Cr:YSGG laser irradiation on root canal walls. Photomed Laser Surg. 22, 291-297.
- Jin JY, Lee SH. A comparative study of wound healing following incision with a scalpel, diode laser or Er,Cr:YSGG laser in guinea pig oral mucosa: A histological and immuno-histochemical analysis. Acta Odontol Scand 2010; 68:232-238.
- Takeda, A., Anjo, T., and Tkashina, M. (2003). Apicoectomy using Er:YAG laser–a clinical study. International Congress Series 1248, 261-263.
- Ebihara, A., Sekine, Y., Takeda, H., Suda. H (1997). Application of Er:YAG laser to apicoectomy–a preliminary study. J. Jpn. Soc. Laser Dent. 8, 23-30.
- Ebihara, A., Sekine, Y., Takeda, A., Suda, H. (1998). Application of Er:YAG laser to retrograde cavity preparation. J. Jpn. Soc. Laser Dent. 9, 23-31.
- Payer M., et. al. The Chemical effect of LLLT in endodontic surgery: a prospective study on 72 cases. Oral Surg Oral Med Oral Radio Endod 2005 September; 100 (3): 375-379.
- Rahimi, S., et. al (2010). A comparison of the effect of Er,Cr:YSGG laser and ultrasonic retrograde root-end cavity, preparation on the integrity of root apices. J. Oral Sci. 52, 77-81.
- Batista de Faria-Junior, N., et. al. (2009). Evaluation of ultrasonic and Er,Cr:YSGG laser retrograde cavity preparation. J. Endod. 35, 741-744.
- Boutoussov et al. Multiple Beam Laser Treatment Device. Patent Application No. 14/610,650. January 2015.
About the Author
 William Chen Graduated from Washington University School of Dental Medicine and has been in private practice in Granite City, Illinois for over 40 years. He is a Master of the World Clinical Laser Institute and a Master of the Academy of Laser Dentistry. His honours and awards include Fellow of the American College of Dentists, Fellow of the International College of Dentists, Fellow and Master of the Academy of General Dentistry. He has lectured all over the United States, Canada and many other countries, covering several continents. He was the chief investigator for Biolase Technology, Inc. in getting FDA Clearance for Laser Root Canal Therapy and Laser Bone Applications.
William Chen Graduated from Washington University School of Dental Medicine and has been in private practice in Granite City, Illinois for over 40 years. He is a Master of the World Clinical Laser Institute and a Master of the Academy of Laser Dentistry. His honours and awards include Fellow of the American College of Dentists, Fellow of the International College of Dentists, Fellow and Master of the Academy of General Dentistry. He has lectured all over the United States, Canada and many other countries, covering several continents. He was the chief investigator for Biolase Technology, Inc. in getting FDA Clearance for Laser Root Canal Therapy and Laser Bone Applications.
RELATED ARTICLE: A Novel Approach to Veneer Removal: A Clinical Case Report Using Er,Cr:YSGG Laser










