
With rapid progression in the science of restorative dentistry, particularly since the advent of ‘adhesive’ techniques, it is irrefutable that the demand and interest in cosmetic restorations has increased both from dentists and patients alike. Numerous materials and techniques are at our disposal in this modern age of dentistry, giving us the ability to work under the notion of minimal intervention and preserving tooth structure.
With this increase in patients seeking aesthetic improvement, it has become of paramount importance that the aesthetic dentist understands dentofacial aesthetics, contemporary materials, and their application, in conjunction with modern techniques and technologies. Facially driven aesthetic analysis and treatment planning has long been advocated in the field of aesthetic dentistry, with varying objective norms having been identified over the course of history. Digital record taking, combined with digital design techniques, has allowed for the simplification of this process, improving diagnostics and treatment planning, as well as improving communication between clinician and patient, and clinician and ceramist.
All-ceramic restorations are commonly used in aesthetic rehabilitations. Advancements in the physical properties of modern ceramics alongside adhesive bonding have allowed for such. One such family of commonly used all-ceramic materials are the lithium disilicate glass ceramics including Empress 2, e.max (Ivoclar), and Initial LiSi Press (GC), possessing flexural strengths of between 300-500MPA. They are available in varying translucencies and are commonly combined with either staining or cut-back and layering techniques, allowing for appropriate replication of the esthetic goal.
This case presentation highlights some of the key clinical steps involved in the provision of multiple indirect ceramic restorations highlighting the importance of adequate assessment of dentofacial aesthetic parameters and concepts, as well as the use of a digital workflow.
Case Report
A 48-year-old male patient presented, hoping to improve his smile. He sought a functional and aesthetic improvement, previously having undergone several dental procedures in pursuit of this. He was highly aesthetically aware, and prescriptive of his desire to obtain natural, long-lasting aesthetics.
The patient described a history of undersized maxillary teeth, which has been orthodontically repositioned to redistribute residual spaces which facilitated the placement of seven composite restorations. The patient deemed this a success for a period but was disheartened by constant chipping, discolouration and staining of these restorations. Clinically, the existing composite restorations had several associated overhangs and suffered from poor gingival emergence due to the large interproximal spaces. He requested a longer-lasting result which would help him ascertain a more natural aesthetic but was also conducive to basic dental health.
Treatment Planning
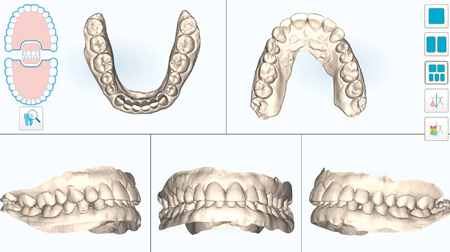
Prior to any intervention, comprehensive aesthetic records were taken, including photographic records, video and digitally acquired dental models (iTero, Align USA). Photographic records drive the initial chair-side discussion with the patient, facilitating evaluation of dentofacial, dentolabial, dentogingival and dental aesthetic parameters. (Fig. 2)
Fig. 1

Fig. 2A

Fig. 2B

Fig. 2C

Fig. 3A

Fig. B
Photographs were then imported into Microsoft PowerPoint, allowing for the use of preformed templates and calibrated rulers to determine and communicate aesthetic short-comings chairside with the patient in a collaborative manner. (Fig. 4)
Fig. 4

Several key aesthetic shortcomings were identified to be sources of visual tension including:
- Asymmetrical central incisors and lateral incisors when comparing with contralateral
- Inappropriate W:H Ratios of central incisors
- Gingival margin asymmetry between 12 and 22, 13 and 23.
- Increased size of buccal corridor due to inset 14 and 24
- Dyschromia due to underlying tooth discolouration and failing restorative margins
- Inappropriate flaring of teeth resulting in divergent axial inclinations
Aesthetic Planning
Multiple treatment plans were presented to the patient to address the above shortcomings, including:
1) Further Orthodontic treatment to improve overbite.
2) Gingival recontouring of 13, 22, 23
3) Provision of 8-10 new restorations, fabricated from either:
a. Direct composite resin
b. Indirect all-ceramic restorations
The patient declined further orthodontic treatment, however, was made to understand the implications of his overbite on restorative longevity. The patients desire for optimum aesthetics and longevity resulted in him electing for gingival recontouring and the placement of 8 all-ceramic restorations. GC Initial LiSi press restorations were proposed upon collaboration with DT Douglas White (Fusion Dental Lab, Brisbane, Australia).
An appropriate initial reference point when commencing aesthetic planning may be incisal display of the central incisors when the lip is at rest. Vig & Brundo suggested varying incisal display at rest between males and females, suggesting males display 1-2mm of incisal edge when the lip is at rest. (Fig. 5) Since no incisal edge was on display at rest, a perio-probe was utilised to determine the position of the incisal edge and its negative relationship with the upper lip. In this case, the incisal edge was flush with the position of the lip suggesting that the incisal edge could be increased by 1-2mm to fit the aesthetic norms described in the aforementioned study. It may be interesting to note that many studies have been conducted since the previously mentioned study, with some suggesting the canines are a more stable reference point with less variation amongst patients.
Fig. 5

at rest will vary between males and females with 1-2mm of display being deemed aesthetic for males and 2-4mm for females.
Digital scans of the patient’s dentition were transferred to the ceramist, alongside the full photographic series. A digital wax-up was requested to allow the patient to pre-visualise the final treatment, facilitate in-mouth evaluation, guide depth of reduction during preparation phases and in the fabrication of provisional restorations.
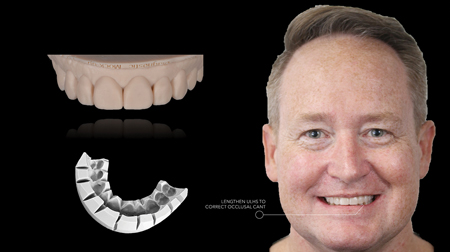
The digital models were calibrated with the patient’s facial photographs prior to fabricating a digital wax-up. Screenshots were shared by the ceramist alongside virtual conferencing with screen-sharing enabled. This ensured laboratory procedures were being conducted in accordance with the patient’s prescription, allowing for several modifications through open-communication and collaboration prior to finalisation of the wax-up. (Fig. 6)
Fig. 6

Upon approval of the proposed digital wax-up, a digital model was created which was then prepared for 3D printing. A 3D printed model of the wax-up facilitated fabrication of a PVS key allowing for the use of bis-acryl temporary crown material to create an in-mouth nonbonded mock-up. This allows both clinician and patient to assess the suitability of the proposal prior to intervention and make any modifications which may be desired prior to tooth preparation. This is considered a critical step in consenting the patient prior to irreversible intervention. (Fig. 7)
Fig. 7
Technique
1. The patient was suitably anesthetised and bone sounding was completed around 13, 22, and 23. Significant gingival excess was noted allowing for simple gingivectomy to be undertaken to harmonise the gingival margin levels without invading biological width. This was completed through use of a dual-wavelength diode laser (Gemini, Ultradent USA).
2. The PVS key fabricated from the wax-up was used to transfer Bis-Acryl Temporary Crown material intra-orally. Since the target shade was approximately 2 shades from the original shade, a facial reduction of 0.6mm was required to compensate for the influence of the underlying stump colour.
3. Preparation was completed under 5x magnification and illumination. Margins were finished equi-gingivally and care was taken to ensure appropriate path of insertion. Where diastemas are present, extension of the margins interproximally allows for the recreation of appropriate emergence profiles in the interproximal area. Evaluation using CAD software can help highlight areas that are undercut in relation to the desired path of insertion.
4. The restorations were polished and photographs of the prepared stumps with reference shade tabs were taken to assist the ceramist with final layering and ingot selection.
5. A double cord technique was utilised to allow appropriate horizontal and vertical deflection of the gingival tissue adjacent the preparations. Size 000 cord soaked in Viscostat Clear was packed into the gingival sulcus followed by size 0 cord.
6. Digital impressions were taken in the following sequence:
a. Opposing arch–Mandible
b. Each prepared tooth individually
c. Preparation Arch – Maxilla
d. CO Bite
The restorations were tried in with RelyX veneer Try-in paste to ensure appropriate marginal adaptation. Aesthetic approval was sought from the patient after review under various light sources, including in-surgery and natural outdoor light.
The operative field was isolated with rubber dam and the adjacent teeth protected with PTFE tape during the adhesive procedures.
Fig. 8
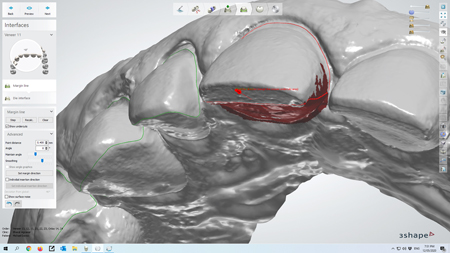
Fig. 9

Fig. 10A

Fig. 10B

Fig. 10C

Fig. 11A

Fig. 11B

Fig. 11C

7. The 000 cord was removed and the teeth provisionalised. The interproximal soft tissue was protected using PTFE tape and the teeth spot etched. A bis-acryl material was loaded in the putty key and the material was shrink wrapped to the prepared teeth. The PTFE tape was removed, the margins finished with high-speed tungsten carbide burrs. The restorations were modified to ensure appropriate aesthetics and glazed with a GC Optiglaze Clear HV to improve patient comfort and aesthetics. A final digital scan was acquired of the adjusted provisionals in-situ to ensure appropriate communication of desired final tooth form to the ceramist.
8. 8 units of GC Initial LiSi Press restorations were fabricated by ceramist Douglas White (Fusion Dental Lab, Brisbane Australia) and characterised using a cut-back technique.
9. The restorations were tried in with RelyX veneer Try-in paste to ensure appropriate marginal adaptation. Aesthetic approval was sought from the patient after review under various light sources, including in-surgery and natural outdoor light.
10. The operative field was isolated with rubber dam and the adjacent teeth protected with PTFE tape during the adhesive procedures.
11. The tooth surfaces were prepared with 43 Micron AlO2 air abrasion followed by phosphoric acid etching and application of Scotchbond Universal. A light curing resin, RelyX Veneer, in a translucent shade was used to bond the restorations in place.
12. Final marginal clean up was completed using a 12 scalpel and the occlusion was checked and adjusted as required prior to scheduling review appointments at 2 weeks and 6-weeks post-operatively.
Fig. 12A

Fig. 12B

Fig. 12C

Fig. 12D

Fig. 12E

Fig. 13

Fig. 14
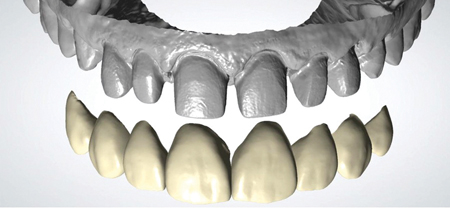
Fig. 15

Discussion
Embarking on any form of aesthetic intervention must start with appropriate diagnosis and communication between the clinician, patient, and the entire restorative team. The use of appropriate dental records can facilitate this conversation, allowing the patient to perceive treatment need, anticipate potential outcomes alongside allowing the clinician and ceramist to best determine restoration design, material choice and workflow.
The digital workflow facilitated simplified smile design, as well as simplifying clinical impression taking, and feedback from the ceramist on preparation design. The ability to manage the soft tissue around each tooth sequentially can streamline the impression taking process, only having to worry about margin visualisation and haemostasis one tooth at a time as opposed to managing 8 preparations simultaneously as per traditional impression taking techniques. Direct to lab workflow and CAD design also allowed the technician to provide appropriate feedback on preparation design, identifying areas of undercut due to inappropriate interproximal taper of the preparations. Such workflows can allow immediate rectification of the preparation design prior to dismissing the patient, minimising wasted chair-time, and improving the patients overall clinical experience by minimising appointment times, additional anaesthesia, and clinical procedures.
A novel approach in assessing the patients dentofacial aesthetic parameters was utilised in this case, particularly in reference to the interrelationship of the facial midline, dental midline and tooth axis cant. The coincidence of the dental midline with the facial midline has been somewhat controversial, in that several landmarks have been advocated as the appropriate reference for facial midline including the glabella, mid-exocanthus, mid-intrapupillary, and philtrum amongst these.
All these landmarks resulted in the evaluation of a straight line against the tooth axis, rendering this approach somewhat flawed when dealing with the majority of the population that present with facial asymmetries. Silva et al have presented the concept of facial flow, suggesting the structures in the middle of the patients face actually follow a line with a directional component that flows between the glabella, nose bridge, philtrum and chin. This is not always straight, referring to this as the facial flow line suggesting all facial structures are positioned relative to this resulting in what we perceive as a sense of harmony and balance. (Fig. 16)
Fig. 16

Fig. 17A

Fig. 17B

Fig. 17C

Fig. 17D

Fig. 17E

Fig. 18

Facial flow analysis was completed at all diagnostics steps, including the 3D digital wax up, intra-oral mock-up evaluation, evaluation of the provisional restorations and during try-in of the final restorations to ensure appropriate harmony was attained. If the cant or shift was to occur towards the red side, considerable visual tension could be expected, and an unsuccessful aesthetic result may have ensued. Although symmetry has been aspirational in aesthetic dentistry for decades, we must endeavour to look towards creating restorations that are in harmony and balance within our patient’s facial structures.
Eight restorations were delivered that appropriately rehabilitated natural aesthetics for our patient, sitting in harmony within the patients face, and improving shape, colour, and surface texture. The restorations were bonded with care, ensuring adequate moisture control during the adhesive process, and the use of a bondable restorative material with approximately 500MPa of flexural strength.
Oral Health welcomes this original article.
References
- Vig RG, Brundo GC: The kinetics of anterior tooth display. J Prosthet Dent 1978;39:502-504
- Misch CE. Guidelines for maxillary incisal edge position-a pilot study: the key is the canine. J Prosthodont. 2008 Feb;17(2):130–4.).
- Silva BP, Mahn E, Stanley K, Coachman C. The facial flow concept: An organic orofacial analysis—the vertical component. The Journal of Prosthetic Dentistry. 2019 Feb;121(2):189–94.
About the Author
 Dr Bharat Agrawal completed a Bachelor of Oral Health in Dental Science and Graduate Diploma of Dentistry at Griffith University, Gold Coast, with multiple final year awards. His passion for aesthetic and restorative dentistry led him to complete a Masters in Aesthetic Dentistry with Distinction through King’s College in London and a Postgraduate Diploma in the Management of Advanced Aesthetic and Restorative Dentistry through the Academy of Dental Excellence. He has presented on tooth whitening, Invisalign, Aligner-Restorative pathways around the world. Currently a partner in private practice on the Gold Coast, he is passionate about the paradigm shift towards minimally invasive approaches to comprehensive smile makeovers.
Dr Bharat Agrawal completed a Bachelor of Oral Health in Dental Science and Graduate Diploma of Dentistry at Griffith University, Gold Coast, with multiple final year awards. His passion for aesthetic and restorative dentistry led him to complete a Masters in Aesthetic Dentistry with Distinction through King’s College in London and a Postgraduate Diploma in the Management of Advanced Aesthetic and Restorative Dentistry through the Academy of Dental Excellence. He has presented on tooth whitening, Invisalign, Aligner-Restorative pathways around the world. Currently a partner in private practice on the Gold Coast, he is passionate about the paradigm shift towards minimally invasive approaches to comprehensive smile makeovers.
RELATED ARTICLE: Provisional Restorations in Fixed Prosthodontics: An Essential Step for Success










