
Restorative dentistry and periodontology have always been and forever will be inextricably linked. Integrating all elements of dentistry is an art and the science and is salient to long-term success of dental restorations and patient care. When placing a restoration, one must consider its effect on the entire stomatognathic complex. Case in point, the placement of “a simple” occlusal restoration that is “too high” by some small amount can potentially result in a hypersensitive tooth, possible TMJ issues and a disgruntled patient. Thus, I suggested that there is no such restoration that is simple. Careful attention to all elements of the process is required. Success is no accident; it is a planned event that culminates with the adherence and the employment of the following 5 Key Principles.
- Evidence-based knowledge.
- Protocols with a proven track record of success.
- Exacting techniques.
- Durable materials.
- Meaningful clinical experience.
The first four 4 are self-explanatory. I wish to clarify Key Principle 5. I quote the late oral surgeon and educator Dr. Simon Weinberg. “Good judgment comes from meaningful clinical experience. However, meaningful clinical experience often comes from bad judgment”. That is to say, we learn best from our mistakes. I define clinical experience as the accumulation of knowledge by way of careful observation and honest assessment of not only one’s own treatment outcomes, but those of other well respected clinicians. With this article, I hope to share my meaningful experiences with the reader.
For more than 6 decades, it has been known that we must not violate the biologic with dental restorations. Transgressing this fundamental rule will result in adverse biological outcomes and failures.
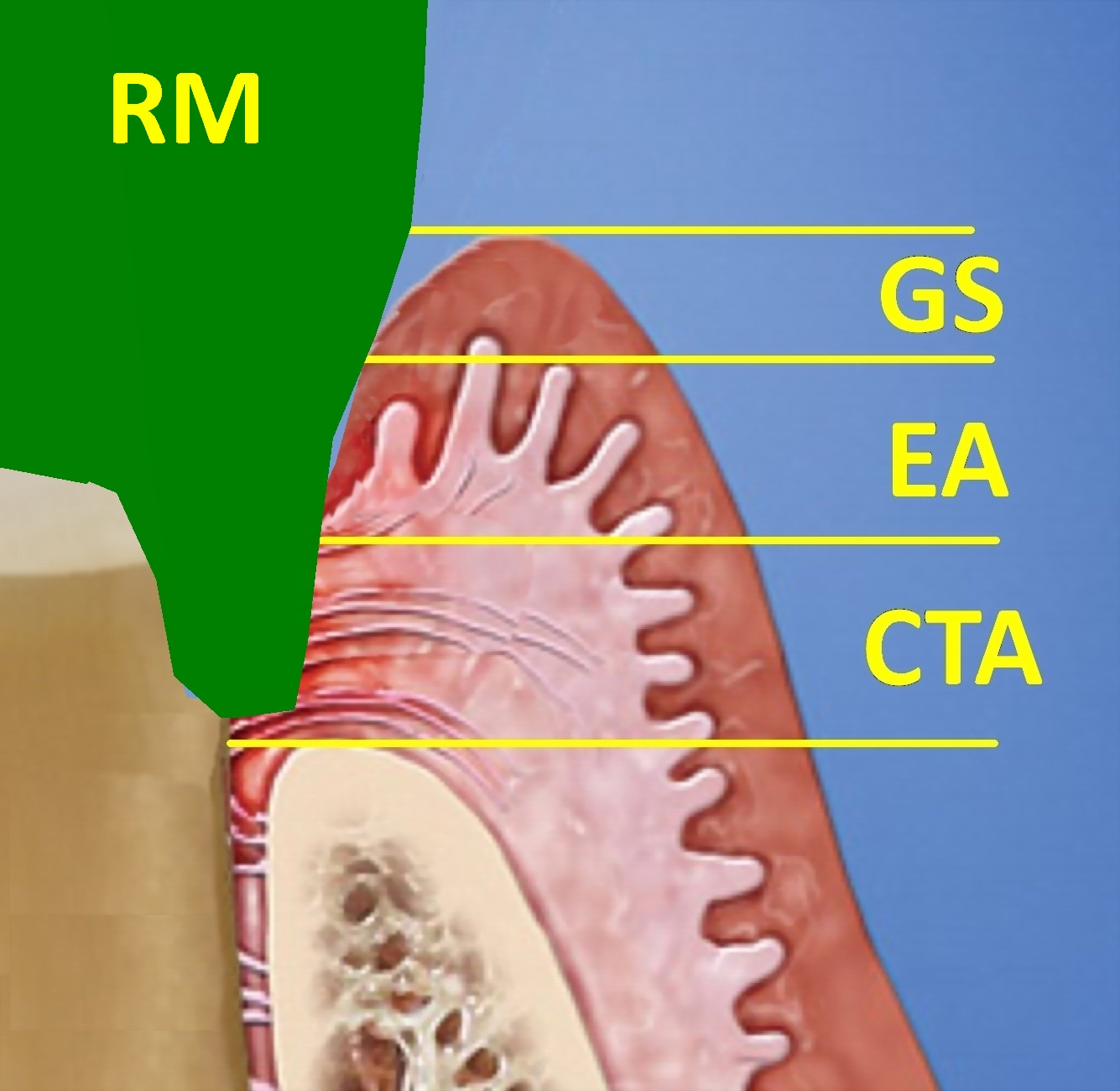
The Biologic Width, Fig.1, also called the attached gingiva, contains the barrier against the ingress of oral microbes that cause periodontal breakdown. It is typically divided into 3 zones: Fig.2 the Gingival Sulcus (GS), the Epithelial Attachment (EA), and the Connective Tissue Attachment, (CTA), which is located apical to the Cemento-Enamel Junction, (CEJ). In Fig.3, we have the ideal arrangement where the Restorative Margin (RM) is just “tucked” into the Gingival Sulcus. This is often required to hide a crown margin in the anterior segment. When chasing decay, we may find ourselves deeper and passed the sulcus into the epithelial attachment. The gingival complex may tolerate this if the restorative margin is well executed and thus imperceptible, as in Fig. 4. Hence we must strive to capture the prepared crown margin with an accurate impression and guide the lab phase accordingly to avoid a perceptible “open margin” at the interface that is not optimal, as in Fig. 5. Ultimately this will fail.
Fig. 1

Fig. 2
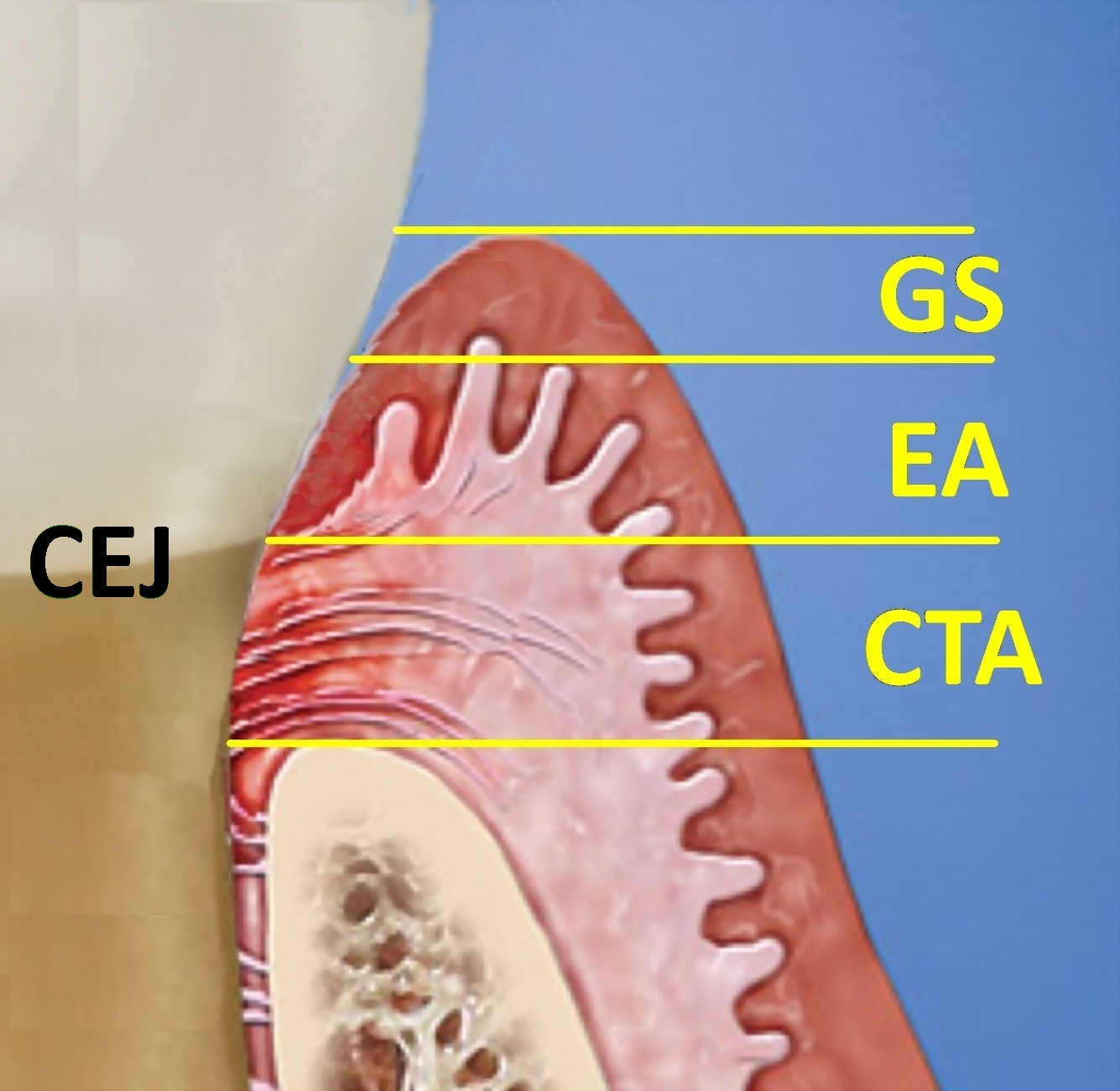
Fig. 3
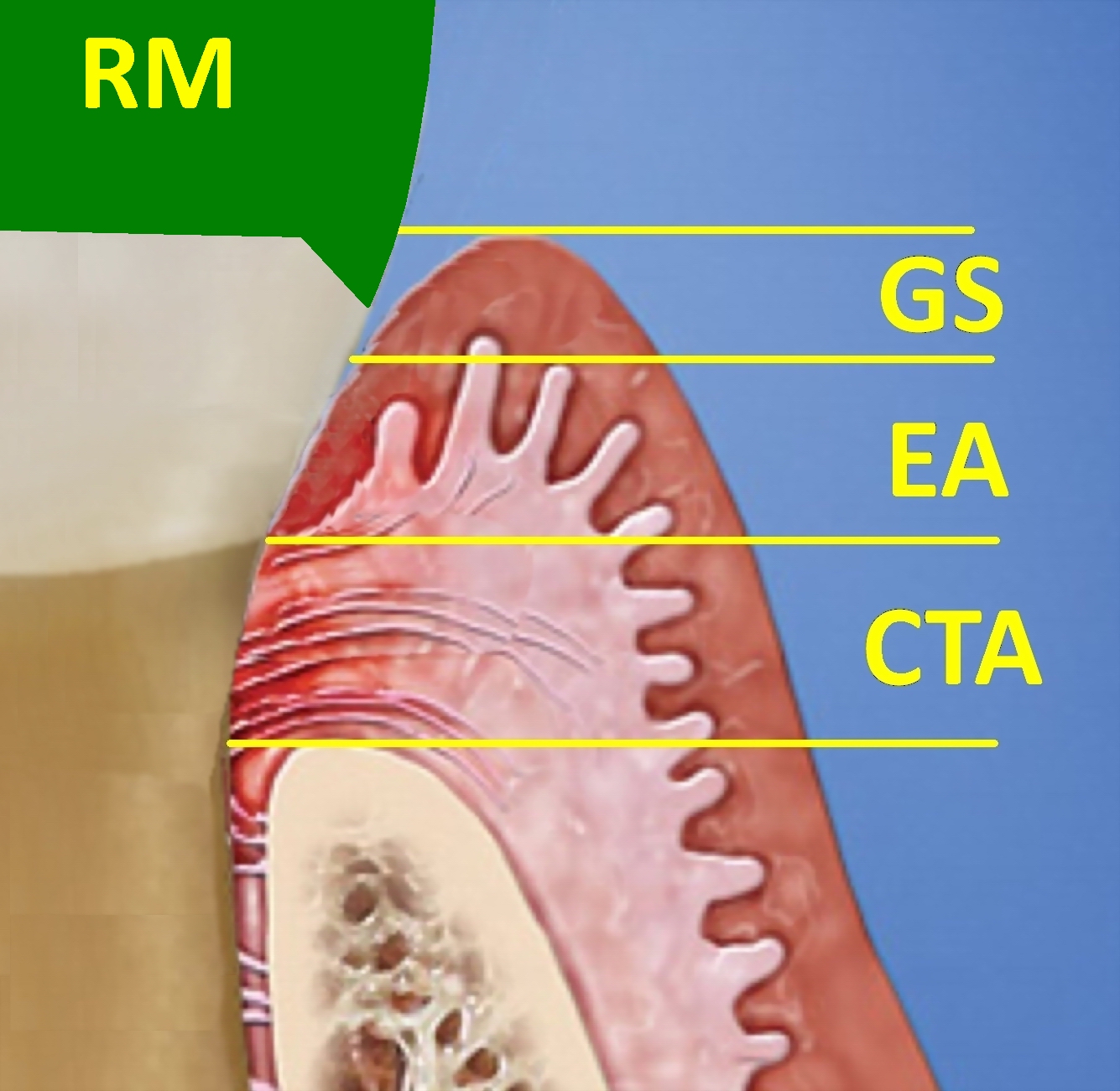
Fig. 4
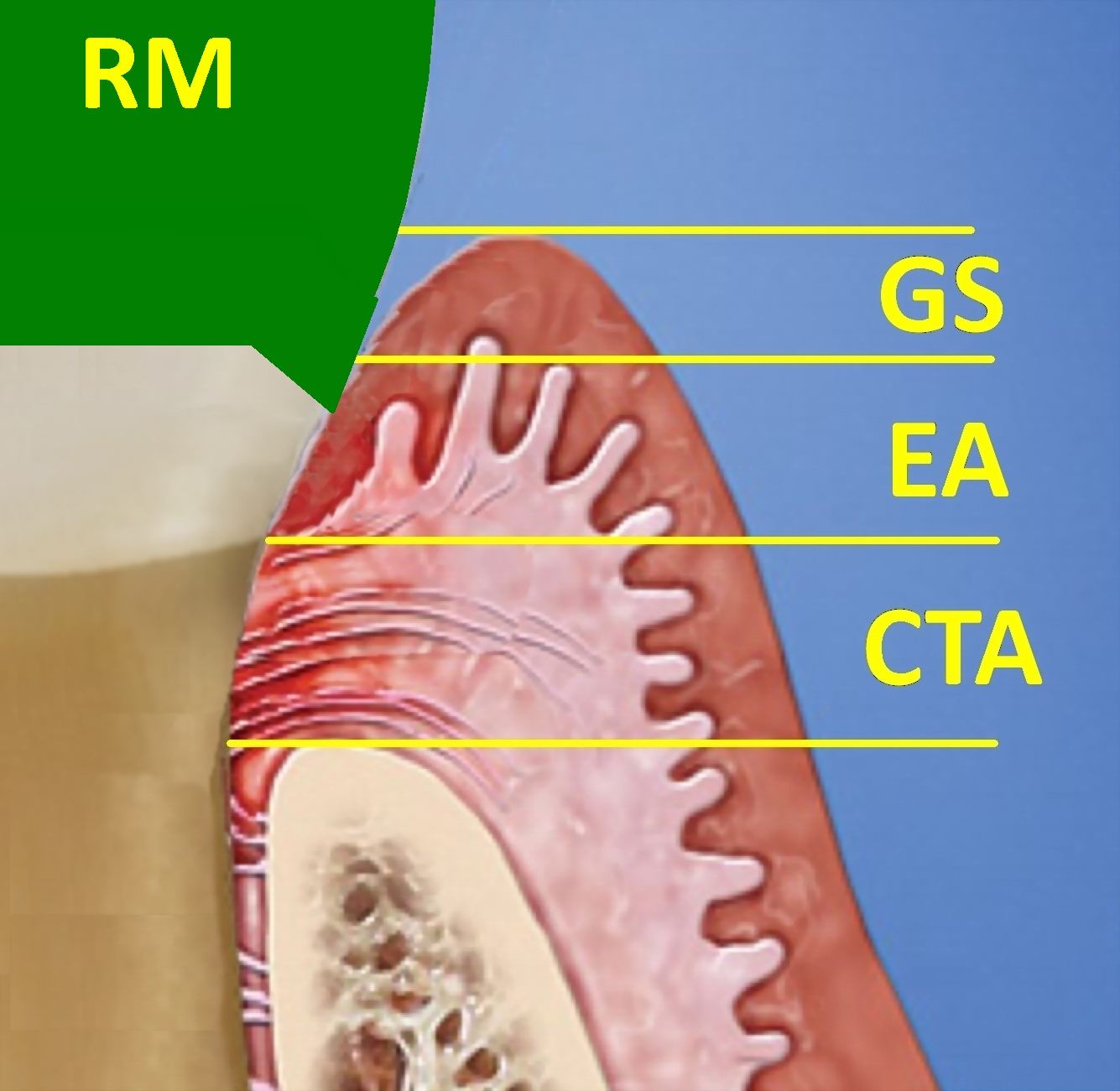
Fig. 5

The deeper one drills into the epithelial attachment and beyond into the connective tissue attachment, the greater the potential for operative trauma and the less likely one is to obtain an accurate impression by any method. (Fig. 6) This will result in a poorly executed crown margin. (Fig. 7) That is a mechanical insult as well as a source of chemical irritation as the cement may degrade with the ingress of oral fluids and bacteria. The biological barrier against the ingress of bacteria has been iatrogenically wounded and potentially destroyed. Most importantly, if a periodontal problem is not present preoperatively, one must ensure that a problem is not introduced postoperatively. As such, the Biologic Width is always a consideration in any operative manoeuvre that approaches the soft tissue.
Fig. 6
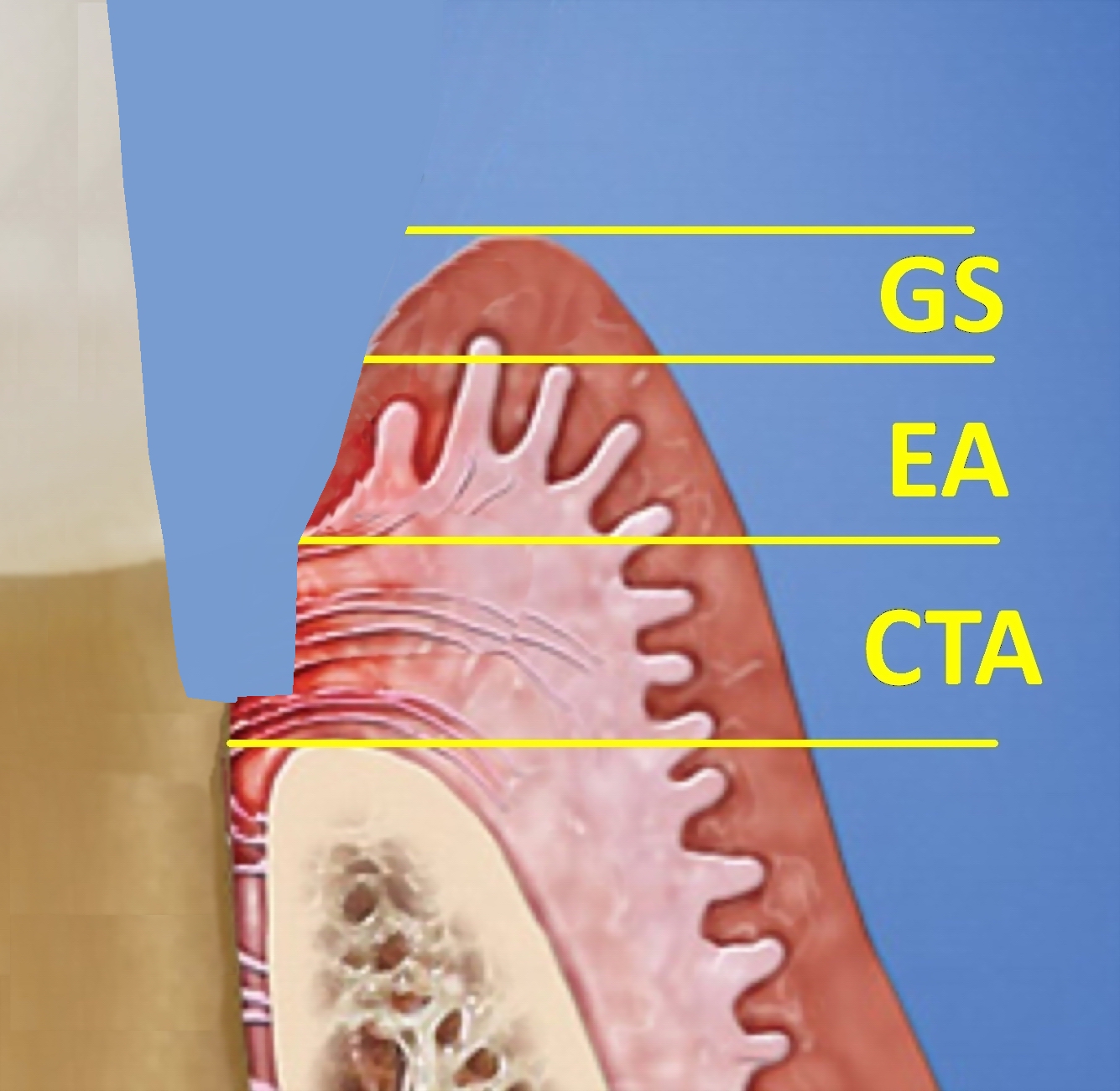
Fig. 7
With this in mind, integrating endodontics, periodontics and restorative dentistry is key to the long-term success of dental restorations. What follows are case examples that illustrate this integration. These cases were completed by the author who is a general-practitioner that provides periodontal surgery, endodontics in addition to restorative protocols.
Figs. 8-10 is a case undertaken in 1983-1984 and is of a male patient who was 57 years old at that time. Gingival inflammation was present with mild generalized horizontal bone loss, but the teeth were not mobile. In such cases, one must plan to eliminate factors resulting in diseased tissue before moving to definitive tooth preparation and impression taking. An intact and stable Biologic Width must be developed. By employing standard surgical protocols, Key Principles 1 and 2, full-thickness flaps were elevated to allow for thorough root debridement and pocket reduction by securing the flaps in a more apical position. Figs. 11, 12 & 12A illustrate post surgical wound healing. The teeth were prepared to accept one complete splinted reconstruction with ball attachments to secure a cast partial denture. Fig. 13 highlights Key Principle 3, employing an exacting technique. Every task must be executed as perfectly as possible, especially tooth preparation. Here, great care was taken to not injure the gingival architecture developed by way of surgical intervention. The restorative dentist who comprehensively understands the periodontal surgery involved, develops tremendous respect for the tissues during tooth preparation. The custom in 1983 was the placement of porcelain-fused-to-metal (PFM) restorations with a very fine metal margin that was just “tucked” into the gingival sulcus, as illustrated in Figs. 3 & 4. The protocols for the placement of implants in partially edentulous sites had not yet been fully established in 1983. Hence a removable appliance was employed to replace missing posterior teeth. Fig. 15
Fig. 8

Fig. 9

Fig. 10

Fig. 11

Fig. 12

Fig. 12A

Fig. 13

Fig. 14

Fig. 15
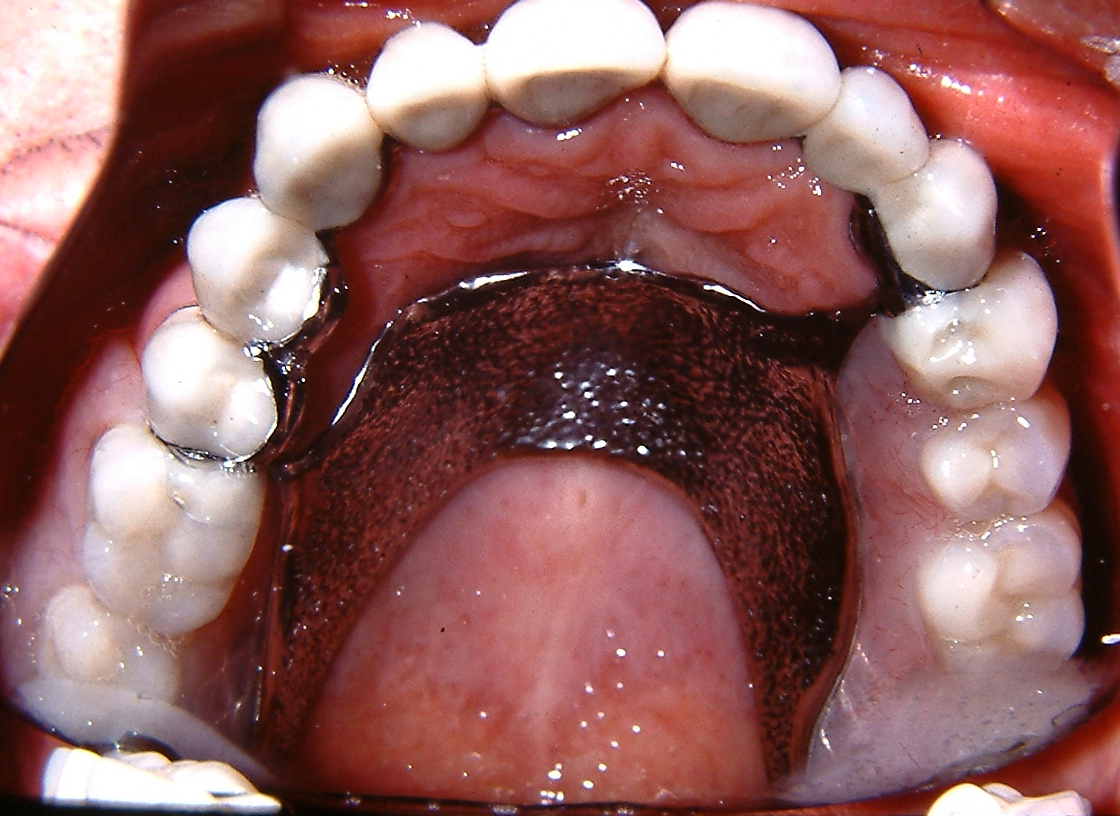
Figs. 16 & 17 below, show the case in 2006 when the upper reconstruction was 22 years-old. Note that the lower teeth were restored over the intervening years. It is noted that some recession had taken place due to normal physiological aging. This brings me to Key Principle #5, the employment of durable materials. Over 4 decades of practice, I observed that PFM restorations composed of a Gold alloy or Silver-Palladium have proven to be very biocompatible and durable restorations. I am also confident in restorations consisting of porcelain fused to a Zirconia core in the anterior segment for single units and small fixed bridges where aesthetic demands are critical.
Fig. 16

Fig. 17

Fig. 18 shows that the recession and exposure of metal margins were never an aesthetic issue due to the presence of a forgiving smile line. The patient passed away in 2014 with this upper reconstruction and original cast partial denture that had given service for 30 years. Often after inserting a restoration, a patient may ask, “How long will this last?” I habitually offer the following: “The mouth is a harsh environment. A restoration starts to fail the instant it is inserted. My job is to make it fail as slowly as possible, so that you the patient fail before the restoration”. My 43 years of clinical experience have informed me that this is often the rule rather than the exception. This level of success was a result of definitively addressing the pre-existing periodontal issues in conjunction with restorations that were harmonious with host tissue. Restoration fabricated by Gabriel and Carol Pintos.
Fig. 18

CASE 2
Figs. 19 & 20 reveal the crown on tooth 24 initially inserted in 1979 had failed in 2009. Close-up views of the remaining tooth structure (Figs. 21 & 22) indicate that there may be insufficient tooth material coronal to the crest of bone to allow for an ideal crown preparation without violating the Biologic Width. The tooth was otherwise asymptomatic, and surrounding periodontal structures were healthy. At the time, the patient was 50 years old. Treatment was to place a pin and post retained amalgam core build-up and provisional crown in conjunction with periodontal surgery to facilitate crown lengthening through osseous recontouring to expose more tooth structure for the Biologic Width. Orthodontic eruption was another possible approach to achieve this goal and may have been favoured over a surgical procedure if aesthetics were a primary concern. However, in the vast majority of my cases, a patient will routinely desire treatment that provides the least amount of inconvenience. By the method outlined here, the patient was never without a functionally intact smile.
Fig. 19

Fig. 20

Fig. 21

Fig. 22

Fig. 23 shows that the fracture resulted from cyclic fatigue rather than decay, as the prepared tooth structure was present within the crown and the cement was patent. Gutta-percha was removed from the canal space, and a post-space was developed to accept the narrowest Dentatus post that would fill the space. Great care was taken to not oversize the canal but rather reduce the diameter of the post by grinding away the threads where required. In addition, the threaded posts were not screwed into place. Instead, they fit snugly and were cemented to avoid lateral force vectors that might split the root. Two additional self-tapping pins were placed (Figs. 24 & 25). Note that this was done before the elevation of the soft-tissue flap to have a relatively dry working field. Fig. 26 shows the elevation of the flaps. The pre-existing crown margin is highlighted in green. There is inadequate tooth structure to allow crown preparation to include a ferrule on healthy tooth structure without getting too close to the bone and violating the Biological Width. In Fig. 27, with elevated flaps, the margin was prepared as visibility and access to this delicate area are now optimal. This avoids macerating the gingiva with rotary instrumentation. Simply removing “some gums” with a dental laser does not address the need to expose more tooth structure coronal to the crest of bone. A PFM crown with a metal margin was anticipated; therefore, a shallow bevel or knife edge margin would suffice. This allowed for minimal tooth reduction where root structure was limited.
Fig. 23

Fig. 24

Fig. 25

Fig. 26
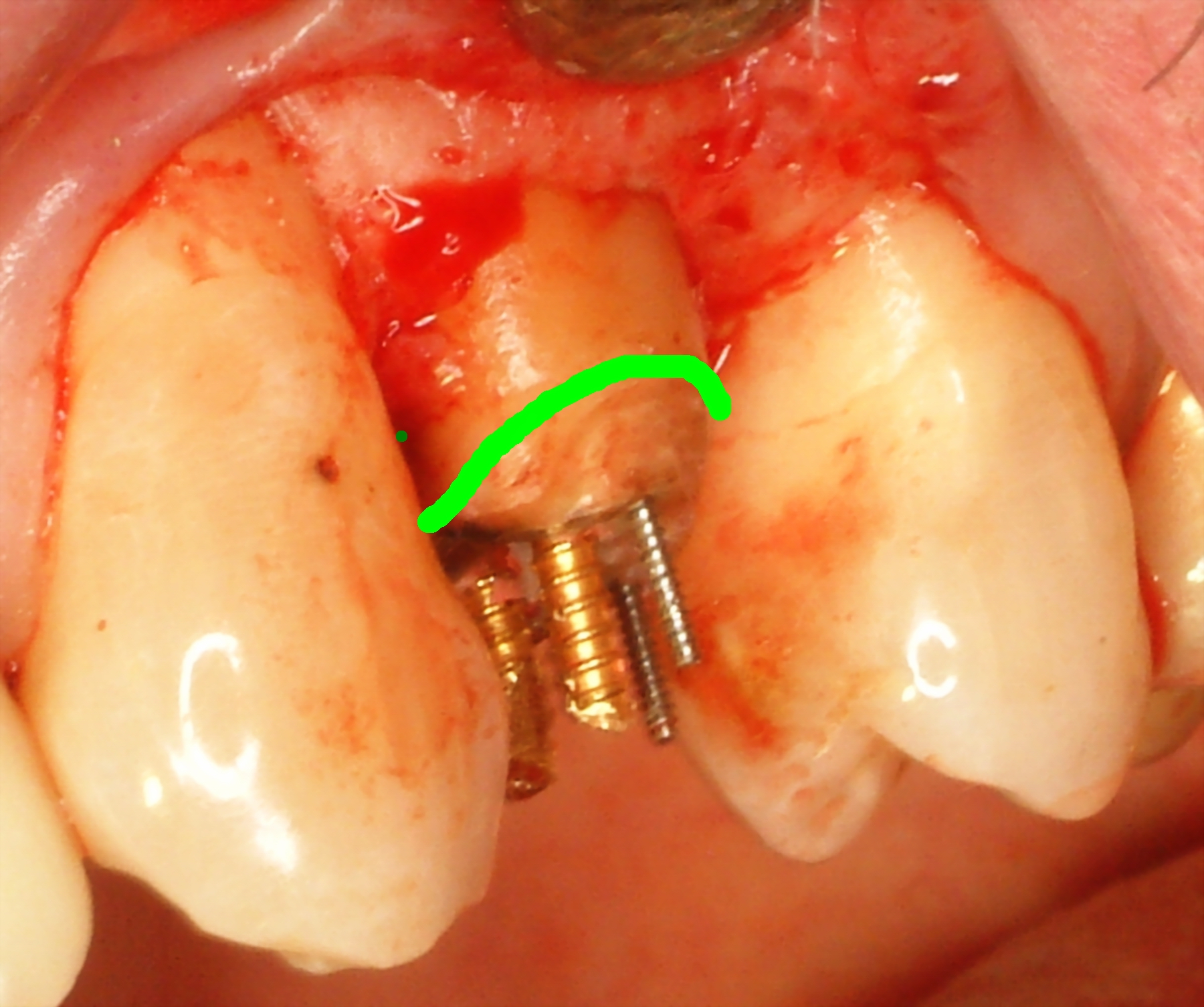
Fig. 27

The crest of bone was recontoured to expose approximately 2 mm of tooth structure apical to the anticipated crown margins circumferentially. Bone removal can often be accomplished carefully and atraumatically with a scalpel blade by cleaving off fragments of bone, akin to carving hard soap. End cutting burs are also helpful if a thick cortical plate is encountered. A cautiously slow approach is stressed to avoid gouging the root surface and unnecessary removal of excess bone. It was anticipated that another millimetre of bone would be lost due to raising a flap. This was factored into the amount of bone that was removed. Figure 28 shows the gingival tissue in relation to the prepared tooth structure. This photograph demonstrates the benefits of simultaneous restorative and periodontal protocols guided by a unified vision of the final restoration. Should a greater dimension of ferrule be deemed necessary for resistance/retention form, it is quickly appreciated and additional bone can be removed without the patient having to undergo a second surgery. If this integration is to be carried out by a team approach, all involved must share a common vision of the ideal outcome before and during treatment.
Fig. 28

Fig. 29 – At this time, the presence of open flaps greatly facilitates the placement and stability of a matrix band on the exposed tooth structure. This is far less traumatic than forcing a band on the insufficient tooth structure as depicted in Figs. 21 & 22, only to have it slip off repeatedly during the placement of the core material. The amalgam core was condensed uneventfully and with confidence as this wonderful material is relatively insensitive to moisture and has documented durability in terms of decades. There is no substitute and in my opinion the use of amalgam is defini-tively justified by all 5 Key Principles. After a few moments of setting time, the matrix band was carefully removed. (Fig. 30)
Fig. 29

Fig. 30

Using only handcarvers, the excess amalgam was removed (figure 31). The large shavings are easily removed with high-volume suction, and care is taken to ensure no excess amalgam remains under the tissue. Furthermore, a rotary instrument should not be used to trim amalgam in the presence of open flaps. A resulting fine grit of amalgam is forced into the tissue that is impossible to remove regardless of the irrigation used. Hence, it is critical not to leave the patient’s side once the amalgam is condensed, only to return to a mass that is too hard to carve by hand. A provisional crown was fabricated and inserted with Tempbond. (Fig. 32) Great care was taken to ensure that the crown margins were precisely adapted to maintain the patency of the cement and thus avoid chemical, mechanical and bacterial irritation during the healing phase. Contacts with adjacent teeth must be firm to avoid food impaction, and the occlusion with the opposing teeth is refined to prevent interferences. Still, contact must be present to stabilize the tooth position. Provisionals must restore proper form and function as they guide the healing phase. The fabrication of provisionals is not “some slap-dash affair that takes place at the end of a long crown and bridge appointment after one has secured an adequate impression” (quote attributed to Dr. Blake MacAdam). Provisionals should strive to match the final restoration in terms of fit and finish. My preference is powder/liquid methyl methacrylate because this material can be added to itself an indefinite number of times. This is indispensable in complex and protracted cases where the provisionals may undergo revision or repair several times. In addition, this material also facilitates provisional fabrication in the presence of open flaps as it is moisture insensitive. After removing excess cement, the surgical site was sutured. (Fig. 33) After three months of healing, Figs. 34 & 35 show that the tissue is pink and healthy. The radiograph (Fig. 36) reveals the bone level. These images help illustrate the integration of restorative and periodontal therapies. This was accomplished by employing the 5 Key Principles. The last task was the fabrication of a final restoration that mimicked the provisional as that design had successfully managed and maintained an intact Biologic Width/zone of attachment. The provisional crown was removed. The green line indicates the crown margin that was established at the time of surgery. (Fig. 37) A retraction cord was placed, and the margin was reprepared to the gingival sulcus. (Fig. 38)
Fig. 31
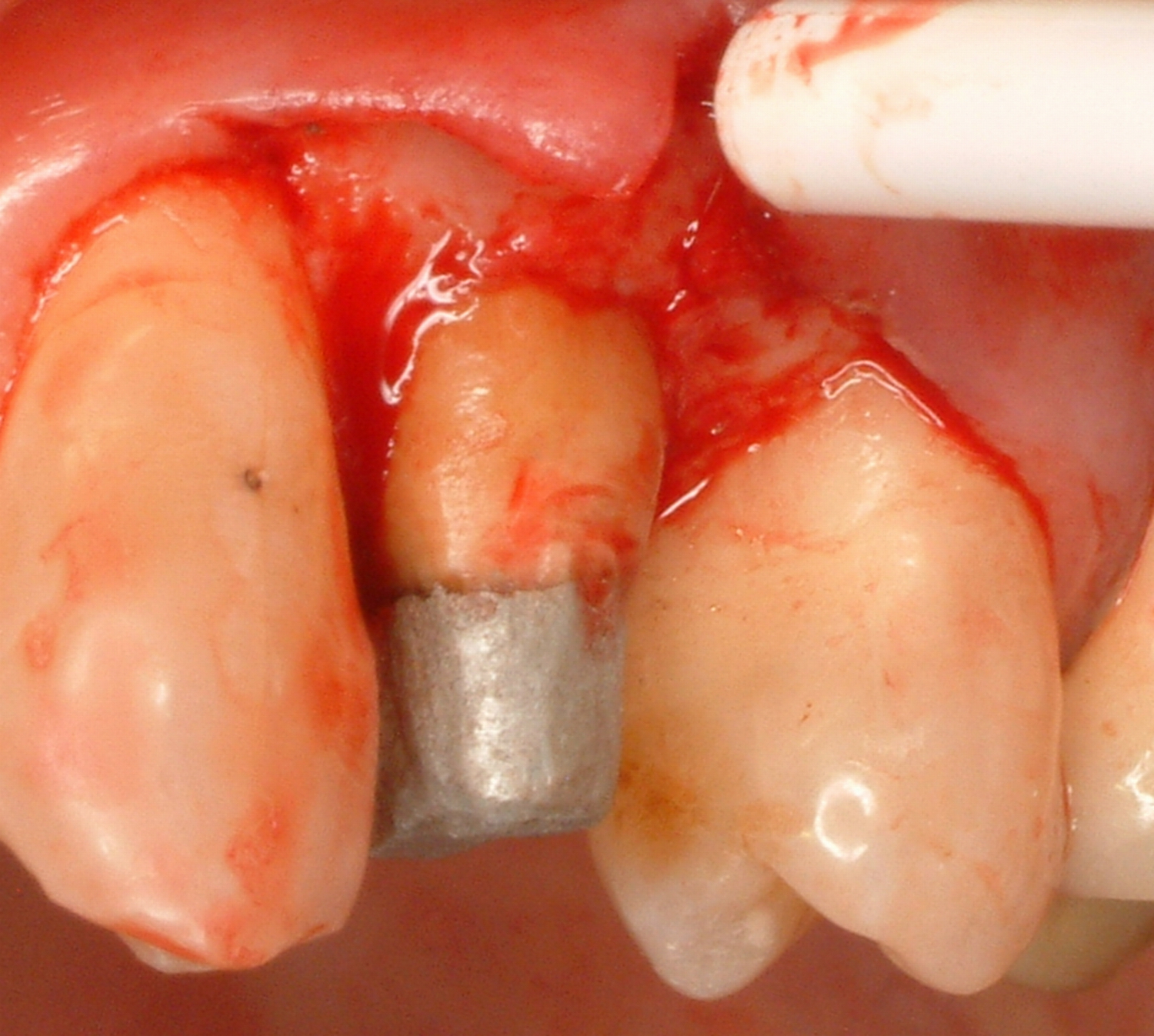
Fig. 32

Fig. 33

Fig. 34

Fig. 35

Fig. 36

Fig. 37

Fig. 38

It is my preferred technique to use vinyl polysiloxane impression material in a full-arch custom tray, even to fabricate one crown. (Fig. 39) This facilitates communication with the laboratory technician by providing as many land-marks as possible. Every detail must be captured with the highest degree of fidelity to allow the lab technician the ability to produce a crown margin that will maintain the health of the Biologic Width. (Fig. 40) The PFM crown has porcelain-over-metal only on the buccal segment that may be readily visible. This ends at the buccal line-angle noted by the arrow. (Figs. 41 & 42) A fine metal band is present elsewhere, as it is my opinion that bare metal allows for the most accurate marginal adaptation. In addition, there was no unnecessary bulk of porcelain interproximally that may become a source of mechanical irritation or a reservoir for bacteria.
Fig. 39
Fig. 40

Fig. 41

Fig. 42

Conclusion
After four decades of clinical experience and the analysis of carefully documented cases, it is apparent that the 5 Key Principles are critical in ensuring predictable and lasting restorative dentistry for my patients. Understanding the interrelatedness of endodontics, periodontics and restorative dentistry and combining and creatively sequencing treatment cannot be understated. As cases are rarely identical, creating a “step-by-step” recipe is challenging. Whenever a restoration approaches the gumline, we are forced to deal with a restorative-periodontal interface, as depicted in Fig. 3. Success cannot be achieved through tooth preparation alone; one often requires a surgical component.
The first case demonstrated that three to four decades of service could be achieved by employing fundamental methods and materials. These methods and materials are still available and relevant today and should not be discounted. The second case encompassed many steps required to salvage what might have been considered a restoratively hopeless tooth.
It is hoped this paper sparks awareness of the importance of periodontal surgery and thereby motivates the reader to seek closer working relationships with surgical colleagues to achieve optimal restorative results. Knowledge, cooperation and a willingness to learn are vital to a successful patient outcome. Patients deserve the best we can give. From a personal perspective, one garners immense pride and satisfaction by securing and maintaining patient trust and loyalty over a long career.
Finally, for the interested GP/Restorative dentist, acquiring the skills to provide surgical protocols not only increases clinical success, it also enhances ones creativity in managing ever-increasing clinical complexities. For this author, it has resulted in a career that is both technically challenging and intellectually stimulating. Here I ask the reader to ponder, ”What’s in your Toolbox?…Is it adequate?”
Oral Health welcomes this original article.
About the Author
 Paul Belzycki Since graduation from UofT faculty of Dentistry in 1979, I still enthusiastically provide dental-care as a solo-practicing GP in Toronto. In many regards, I consider Dentistry a hobby. For 35 years, I have preferred Skeet and Trap Shooting as opposed to golf. Lately, this has been superseded by running after 5 adorable grandchildren and two wonderful daughters.
Paul Belzycki Since graduation from UofT faculty of Dentistry in 1979, I still enthusiastically provide dental-care as a solo-practicing GP in Toronto. In many regards, I consider Dentistry a hobby. For 35 years, I have preferred Skeet and Trap Shooting as opposed to golf. Lately, this has been superseded by running after 5 adorable grandchildren and two wonderful daughters.
RELATED ARTICLE: Periodontal Health and Maintenance for Clear Aligner Therapy










