
Introduction
Aclinical career in dentistry provides a multitude of experiences that consolidate what we learn during our formal training. As clinicians, we have the privilege of taking care of our patient family. This is an honour we don’t take lightly. If we are fortunate enough to practice in the same community for many years, we learn to appreciate the outcomes of the care we prescribed and provided – what works well and what does not stand the test of time. The luxury of managing the oral health needs of these same patients over many years also teaches us a critical lesson – the importance of carefully listening to what our patients really want. Patients don’t necessarily seek us out specifically for onlays or implants or removable cast partial dentures. Individuals consistently ask for teeth that are esthetically pleasing, comfortable and that allow them to function normally without having to give their teeth a second thought.
As the current decade draws to an end, this group of authors believes very strongly that a patient-centered approach to dentistry is the only way forward to satisfy what we believe all dental patients are looking for. This notion is going to seem very intuitive to most readers. We are practising at a time when patients are the beneficiaries of treatment solutions that reconcile most of their needs in a safe, time-efficient and cost-effective manner. We believe that a patient-centred approach to dentistry is Essential, Inevitable and Achievable. This article will highlight the reasons why and how we believe this to be true.
Patient Centred Care: Essential
A consistent message heard from practice consultants today is that successful dental practices need to deliver services that make sense to our patients, that are patient friendly and that reconcile the common barriers to care. These barriers can be summarized under the following themes – Fear, Trust, Time, Cost and Value.
It is widely accepted that patients report fear as the number one deterrent to seeking care for their oral health needs. In many instances, an unfavourable experience as a child can have a profound impact on an adult in need of dental care. Therefore, as much as fear can motivate one to act, it can just as often prevent an individual from seeking out advice and/or proceeding with treatment. Some of the most common concerns cited in this regard are the fear of pain, fear of requiring complex surgery, fear of having to miss work, fear of the treatment failing, fear of being able to socialize with confidence during treatment, fear of the outcome/unknown and even simply admitting that one is fearful.
Your patients trust you. This is an enormous privilege. We can all appreciate how hard it is to gain someone’s trust, how long it takes to do so and how easy it is to potentially lose the goodwill we sometimes spend a career nurturing. When it comes to patient care, we can look at the issue of trust through two different lenses:
The potential for a conflict of interest in the eyes of the patient – whose interests are being served with a treatment recommendation?
The competence of the dentist recommending a solution – is this the best person to take care of me?
We are living at a time when one of the most common responses to the question “how are you doing?” is “Oh, I am so busy!” which translates to “I have so little time”. Time is an expensive commodity. Our patients’ lifestyles, occupations and responsibilities at home challenge their availability to meet our available times of operation and the duration of treatment that we often prescribe. Although patients are made aware of a variety of options to address their diagnoses, time is a commonly cited barrier that often forces patients to choose a course of treatment that may not be ideal.
Fig. 1

Fig. 2

Fig. 3

The anticipated high cost of dental treatment is another commonly referenced barrier to care. Understandably, many patients are influenced in their decision-making by the type of treatment that third-party coverage allows them to receive. One of the biggest challenges that we face, as clinicians presenting complex treatment to patients, is the uncertainty associated with unknown and/or unexpected laboratory and component costs. Indeed, the costs can be significant and can include both biologic (morbidity) and specific financial costs. Furthermore, the financial costs are not limited to the treatment estimate patients receive. We must be sensitive to the time required for a patient to be away from work (number and duration of appointments), as well as transportation costs to our offices. We also need to consider that a patient may have the financial resources but chooses instead not to proceed with treatment because they may not value dental care.
Understanding what new patients to our office value is difficult. It requires time and specific skills on our part in order for them to feel comfortable telling a complete stranger what is important to them. Patients value feeling confident, being free from embarrassment and, most often, overall good health. These universal values impact their professional and social lives and, therefore, must be considered and respected when prescribing treatment.
As children, many of us we were taught the Golden Rule – treat others as you want to be treated. A patient-centred care approach for dentistry in 2019 demands that we instead adopt the Platinum Rule – treat others as they want to be treated. It is our view that a profound appreciation for these five barriers is essential in order for our practices to grow and continue to be successful in providing evidence-based solutions that make sense to our patients. There is no script to follow that relates to all of our patients. Each patient presents with unique needs and demands that need to be identified, respected and addressed.
Patient Centred Care: Inevitable
In the early 2000s, many clinicians around the world made a pilgrimage to Lisbon, Portugal to see an example of a facility that was specifically conceived for and designed to provide patient-friendly dental solutions. At that time, the technology had evolved such that patients could be presented with same-day treatment solutions that were safe, predictable and suitable to a patient’s lifestyle without compromising on the treatment outcome. This clinic was built to house a dental laboratory, the latest diagnostic technology and surgical and restorative operatories staffed by clinicians from all disciplines. To this day, patients continue to fly to this facility in Lisbon to be treated comprehensively with immediate solutions that support their quality of life. Over the years, this model has been replicated in other centres around the world with great success.
Fig. 4

Fig. 5

Fig. 6

The advent of rapidly developing digital technology, and its presence in many dental practices, is forcing dentists to rethink how they service the needs of their patients family. Reconciling this trend with a profound appreciation for the barriers to care described above, allows us to offer dental solutions that can complement our patients’ busy lives. Access to CBCT imaging has dramatically changed and improved our ability to diagnose. Our endodontist colleague, Dr. Manor Haas, describes how he has adopted this technology to determine which teeth warrant root canal therapy and will have a successful outcome. He can now see things at the diagnosis phase of care that previously could only be imagined with two-dimensional imaging. Patients are the beneficiaries of the work of clinicians like Dr. Haas, who use CBCT imaging for endodontic related diagnoses. Teeth with a hopeless prognosis are identified before treatment is initiated and instead alternative treatment options are made available to these patients.
Appreciating that fear is a barrier to care necessitates that we present solutions to our patients that respect this common emotion. This can be achieved by designing treatment plans that, when possible, include sedation, avoid extensive grafting procedures and provide patients with transitional protheses that allow them to resume normal activity. Many patients are reluctant to consider augmentation procedures that involve their maxillary sinuses despite the very impressive track record of implants placed in grafted sinuses. By simply tilting implants, for patients missing posterior maxillary teeth, we can very often place implants to retain short span fixed prostheses, avoiding the need for sinus involvement.
Same-day treatment solutions are an exciting way for clinicians to address the cost and time barriers. Dentists have offered same-day indirect restorations for many years by investing in housing the manufacturing of these restorations in their offices. The concept of “immediacy” in implant prosthodontics is another example of this type of service. Patients can present to our office with a non-restorable tooth that requires extraction and leave our offices a few hours later with the tooth extracted, a dental implant placed and a screw-retained provisional in place. This is a predictable, safe and very efficient way of addressing a hopeless tooth.
The idea of immediate implant placement and provisionalization for a full arch continues to be the answer many patients have been looking for. The available protocols, supported by the required infrastructure and logistics, yield a transformative experience for the thousands of patients that have benefited from this treatment solution. In our collective experience, patients repeatedly report that this solution addresses the barriers they had encountered when interfacing with dentistry in the past.
Michelle Ryckman, in her role as a treatment co-ordinator, has been instrumental in identifying solutions to the barriers we have discussed. She has consistently made a compelling argument for dentists to focus on the dentistry – the field we are trained in – leaving the discussions with patients, regarding treatment goals, to other members of the dental team. This patient-centred approach to care removes the dentist from any perceived conflict of interest, allowing him/her to focus exclusively on their responsibilities as trained clinicians. As small business owners, it is understandable that some dentists find it difficult to relinquish that control. However, in time, with the right person coordinating the patient’s care, it becomes liberating for clinicians. We dedicate a lot of time, energy and resources to developing clinical protocols in our practices. We would recommend that this effort should be matched with the same degree of attention when planning our patients’ experiences at our offices.
Fig. 7
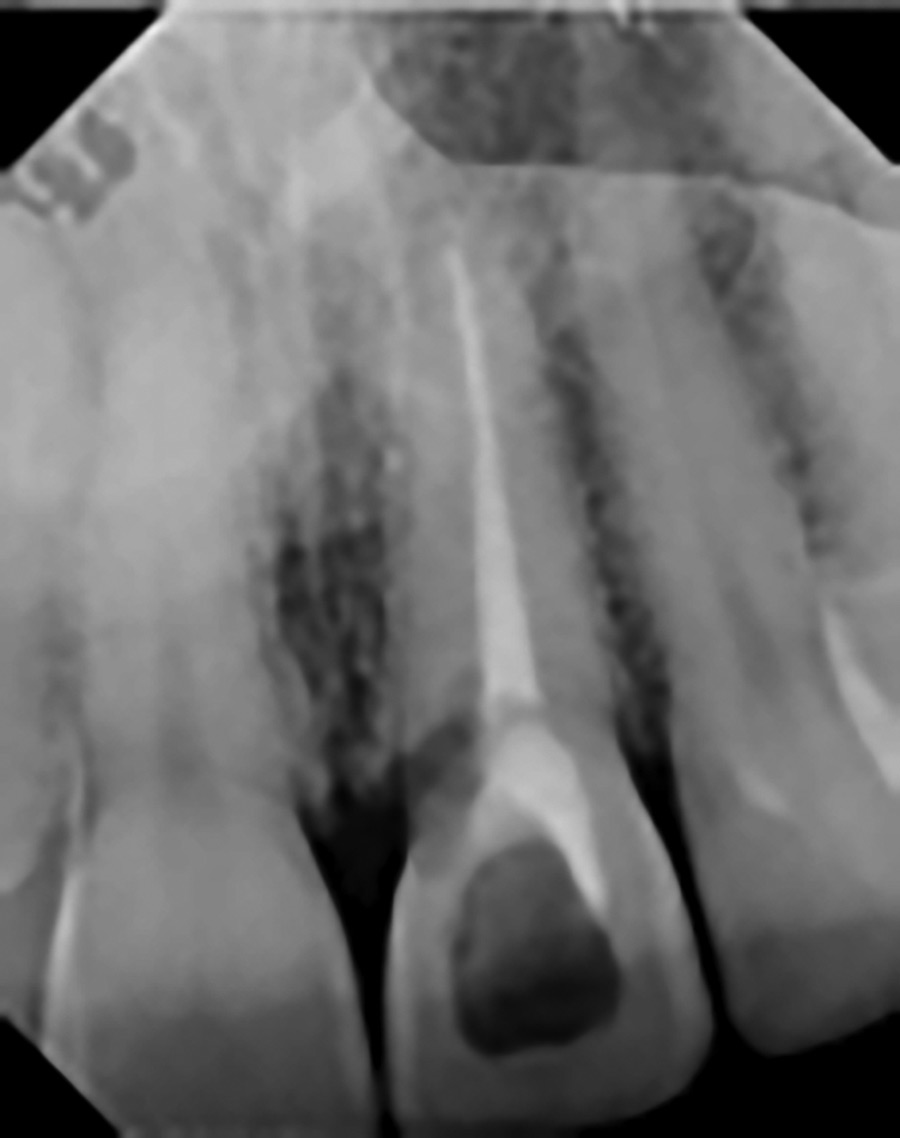
Fig. 8

Fig. 9

Fig. 10

Patient-Centred Care: Achievable
Our industry partners have recognized that the next frontier in developing technology, materials and products for us to consume, must complement protocols that are patient-friendly, efficient, predictable and, of course, cost-effective. Clinicians developing these procedures now have these novel tools to utilize in the development of clinical protocols that can overcome the established barriers to care. Although this is not an exhaustive list, it reflects some of the commonly available technological advances available to most clinicians today.
1. Cone Beam Computed Tomography (CBCT)
• A powerful diagnostic tool that allows clinicians to:
i. Visualize the entire maxilla and mandible and associated anatomic structures
ii. Identify missed canals in specific teeth
iii. Identify suspected external and internal root resorption
iv. Identify the presence and location of supernumerary and impacted teeth
v. Identify pathology
vi. Assess the bones related to the TMJ
2. Intraoral Scanning (IOS)
• This is another very useful diagnostic and treatment tool that:
i. Captures the anatomy of a patient’s dentition, hard and soft tissues in the context of time
ii. Captures the shade of a patient’s teeth
iii. Captures tooth preparations for indirect restorations
iv. Captures the location of single and multiple implants
3. Diagnostic and planning software
• Incorporates the information captured with the CBCT and IOS, that allows clinicians to:
i. Plan prosthetically driven implant placement
ii. Design implant retained prostheses
iii. Design indirect restorations
iv. Plan tooth movement using aligners
4. In-office milling
• Same-day fabrication of indirect restorations
5. Printing machines
• Fabrication of implant placement guides for guided surgery
• Fabrication of removable prostheses and stabilization appliances
• Fabrication of aligners
6. Aligners
• Minor tooth movement
7. Dental implants designed for immediate placement and immediate load protocols
• Surface topography and micro/macro architecture innovation
Fig. 11

Fig. 12

Conclusion
Dentists are privileged to provide solutions for their patients’ needs that, in some small measure, improve their quality of life. We have thankfully moved away from the paternalistic and dogmatic approach to how we design and communicate proposed treatment options. By understanding and recognizing the known barriers to care – Fear, Trust, Time, Cost, and Value – and by adopting the available advancements in technology, we are in a good position to provide patient-friendly solutions that resonate with our patients. In fact, some colleagues would argue that the patient-centric approach – where choice of treatment modality has moved from dentist to the patient, meeting both expectations for esthetics and faster time to teeth – is the only way one can be successful today. However, we can all agree that at the dawn of the new decade, patient-centred care is Essential, Inevitable and definitely Achievable.
Fig. 13

Fig. 14

Fig. 15

Oral Health welcomes this original article.
Acknowledgements: We would like to thank Michelle Rykman and Dr. Steven Bongard for championing the importance of the patient experience.
References
- A critical review of approaches to the treatment of dental anxiety in adults. Gordon D, Heimberg RG, Tellez M, Ismail AI. J Anxiety Disord. 2013 May;27(4):365-78. doi: 10.1016/j.janxdis.2013.04.002. Epub 2013 Apr 13. Review.
- Cone beam computed tomography in Endodontics–a review of the literature. Patel S, Brown J, Pimentel T, Kelly RD, Abella F, Durack C. Int Endod J. 2019 Aug;52(8):1138-1152. doi: 10.1111/iej.13115. Epub 2019 Apr 9. Review
- Immediate loading in partially and completely edentulous jaws: a review of the literature with clinical guidelines. De Bruyn H, Raes S, Ostman PO, Cosyn J. Periodontol 2000. 2014 Oct;66(1):153-87. doi: 10.1111/prd.12040. Review.
- Without Teeth Koka S, TEDx Boca Raton, November 12, 2018
About the Author
 Dr. John P. Zarb is a staff prosthodontist in the Graduate Prosthodontic Department at the University of Toronto and at Mt Sinai Hospital in Toronto, and a Clinical Assistant Professor at the University of Rochester, Eastman Institute for Oral Health. Dr. Zarb joined Barrie Dental Specialists in 2003. He is a Fellow, examiner and Director of the Royal College of Dentists of Canada, a Fellow in the Academy of Dentistry International, and Fellow in the Academy of Prosthodontics and a former Director of the American College of Prosthodontists.
Dr. John P. Zarb is a staff prosthodontist in the Graduate Prosthodontic Department at the University of Toronto and at Mt Sinai Hospital in Toronto, and a Clinical Assistant Professor at the University of Rochester, Eastman Institute for Oral Health. Dr. Zarb joined Barrie Dental Specialists in 2003. He is a Fellow, examiner and Director of the Royal College of Dentists of Canada, a Fellow in the Academy of Dentistry International, and Fellow in the Academy of Prosthodontics and a former Director of the American College of Prosthodontists.
 Ms. Michelle Ryckman is currently responsible for the development and implementation of the “new patient journey” and consultations with potential implant patients every day in a large thriving dental implant practice.
Ms. Michelle Ryckman is currently responsible for the development and implementation of the “new patient journey” and consultations with potential implant patients every day in a large thriving dental implant practice.
 Dr. Steven Bongard is the founder and clinical head of Chrysalis Dental Centre in Toronto, a dental implant only facility focused on “same day” dental implant solutions. Dr. Bongard has extensive experience in implant placement, bone grafting procedures, as well as the prosthetic component of implant restoration.
Dr. Steven Bongard is the founder and clinical head of Chrysalis Dental Centre in Toronto, a dental implant only facility focused on “same day” dental implant solutions. Dr. Bongard has extensive experience in implant placement, bone grafting procedures, as well as the prosthetic component of implant restoration.
 Dr. David Powell currently practices at Barrie Dental Specialists and is a member of the prosthodontics division at Chrysalis Dental Implant Centres. He is also a lecturer and assistant professor of Prosthodontics at University of Toronto.
Dr. David Powell currently practices at Barrie Dental Specialists and is a member of the prosthodontics division at Chrysalis Dental Implant Centres. He is also a lecturer and assistant professor of Prosthodontics at University of Toronto.
RELATED ARTICLE: Patient-Centred Care, Soft Skills and Good Business










