
Wouldn’t it be amazing if there was a product you could just paint on a tooth to stop caries, prevent caries and decrease tooth sensitivity? Well, it exists and it’s called silver diamine fluoride (SDF). It is inexpensive, easy to apply, painless and does not create aerosols. SDF can be used on patients of all ages, has minimum contraindications and can be applied by certified dental assistants, dental hygienists and dentists. Your patients will be thrilled: no painful needle, no noisy drill, no expensive bill and it’s done in minutes. I started using SDF at the start of the COVID-19 pandemic when I needed a way to treat caries without generating aerosols. I quickly realized that SDF has many more benefits and I continue using it now and will in the future.
What is silver diamine fluoride?
SDF is composed of silver, fluoride and ammonia. Silver is antimicrobial, fluoride re-mineralizes and ammonia stabilizes silver and fluoride in solution. Silver is substantive preventing reinvasion of cariogenic bacteria. In fact, SDF does not just stop caries, it prevents future decay. How does it work? SDF decreases acid dissolution of the tooth structure and increases: hydroxyapatite, fluorapatite, mineral density and hardness. It also occludes dentinal tubules which decreases tooth sensitivity.1
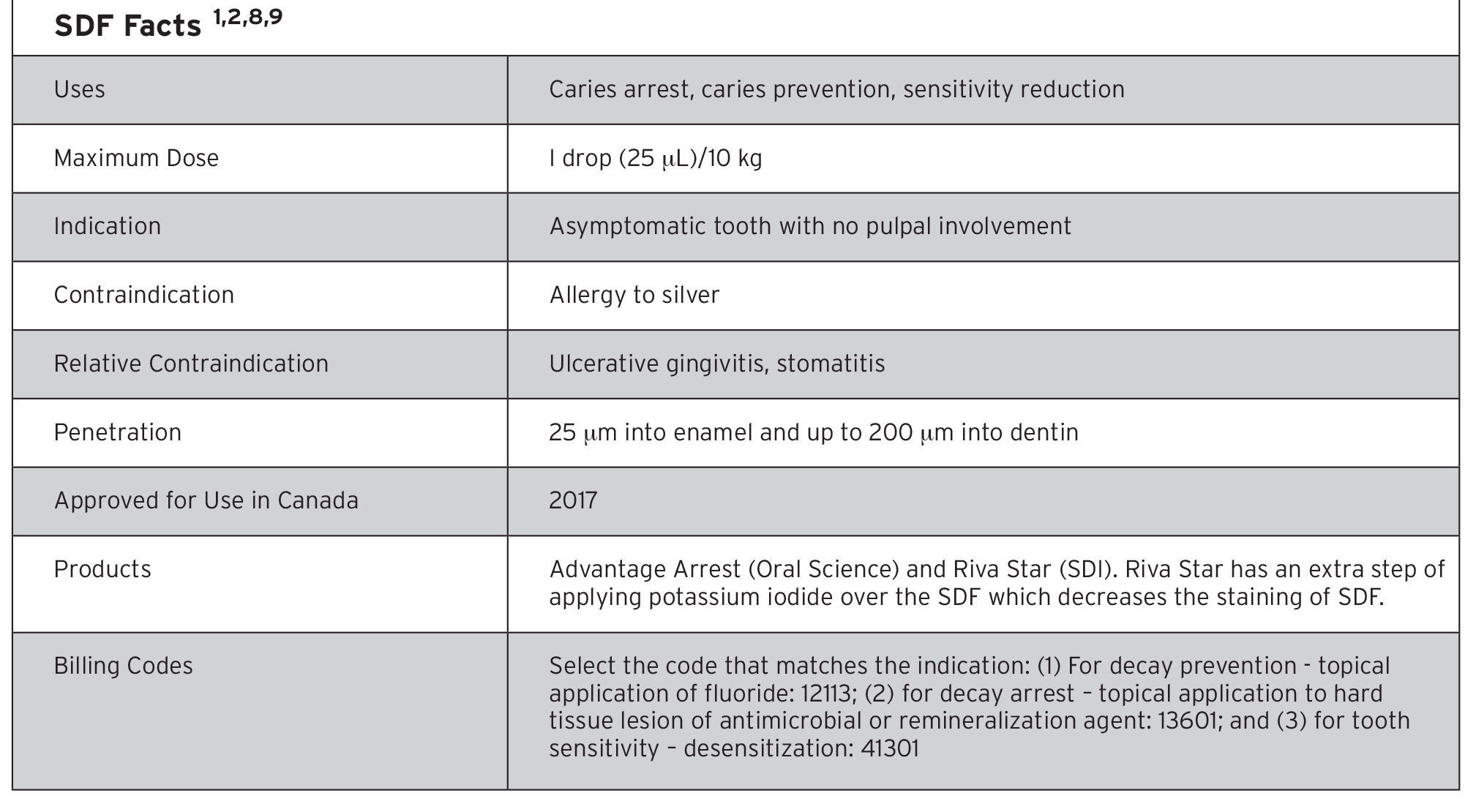
Here is a fun fact: SDF was discovered from the Japanese practice of tooth blackening, called Ohaguru, in the 19th century. Blackened teeth were a sign of beauty and it was discovered that the blackening agent made teeth stronger. This beauty trend led to the discovery of SDF which has been used in Asia for 80 years with no long-term consequences,2 See Table 1.
Table 1
How effective is SDF?
SDF has 3 uses: 1) caries arrest, 2) caries prevention and 3) reduction of sensitivity. How does SDF compare to other options for these uses? SDF is better than topical fluoride and atraumatic restorative treatment (ART), similar or better than glass ionomer (GI) and cheaper than sealants. The fluoride concentration is 44,800 ppm F- ion, which is about double the F- concentration of fluoride varnish.3 A systematic review with a high level of evidence showed that SDF is 89% more effective than other treatment options such as placebos in arresting caries.4 Another systematic review showed that 81% of active caries was arrested in clinical trials.5 After one application, 47%-90% of carious lesions were arrested, depending on the location (anterior teeth yield better results than posterior) and the size of the caries. This sounds great, but the effectiveness decreases over time. Ideally, one needs to apply it every 6 months for at least the first 2 years.1
Clinical applications for SDF use
- In patients who cannot tolerate traditional restorative treatment, such as those unable to cooperate, medically compromised and dentally anxious groups
- To arrest existing decay until the teeth can be restored, when there are long wait times for appointments and/or the patient has generalized decay
- For carious lesions that are difficult to treat, for example: decay around crown margins, teeth that can’t be isolated and those that are hard to access
- In patients who have a high caries risk
- In patients who do not have access to dental care
Staining
SDF is a great product, but it has one major disadvantage: it turns the tooth black. (Figs. 1-3) This is due to the oxidation of silver. It will not darken healthy tooth structure, but it will turn demineralized enamel and dentin, including white spot lesions, permanently black. While the darkness is unappealing, it is an indicator of effectiveness. It also stains soft tissue, clothing and countertops, so be careful when applying it. While soft tissue stains will clear after about two weeks, they can be avoided by applying Vaseline on the face and nearby soft tissue before using SDF. Instruct the patient to remain still and isolate the area using dri-angles and cotton rolls to reduce collateral staining. You are probably thinking that patients will not agree to SDF because of the blackening side-effect, but many do not mind it and they would rather have the stain than go through traditional treatment or general anaesthesia. In fact, 67.5% found the staining in the posterior tolerable compared to 29.7% for anterior sites.6 For situations where aesthetics is not of primary importance, SDF is a great option. Make sure you inform your patients about the staining and get their informed consent for treatment before proceeding with SDF application. Let them know that the carious lesion will darken over time after SDF application.
Fig. 1

Fig. 2

Fig. 3

How to apply SDF2
- Isolate the area
- Dry the lesion
- Apply SDF to the lesion
- Allow SDF to absorb into the lesion for 60 seconds
- Remove excess by dabbing the lesion with a cotton pellet
- Let it dry for 60 seconds or apply fluoride varnish
- Re-apply in 1-3 weeks
- Re-apply in 6 months or apply glass ionomer (GI)
It is not necessary to excavate caries before application, but you can elect to do so if you want to diminish staining. However, it is essential to remove gross debris in order to allow SDF to contact dentin.
For interproximal lesions, place puffy floss in between the teeth, dab SDF on the floss near the contact, pull the dampened floss into contact area and leave it there for 1 minute. Alternatively, elastic separators can be placed and the patient can be recalled a week later to remove the elastics and apply the SDF.
Covering SDF with fluoride varnish increases its effectiveness and decreases the metallic taste of SDF. If a restoration is done the same day, do not place F- varnish over the SDF, as it will interfere with bonding of the restoration.
Yes, it is that simple. No pain. Easy to do. Little time.
Placing a Restoration
If you place a light-cured restoration on the same day as SDF application, the entire restoration will turn black, as the silver precipitates out with light-curing. You can avoid this by restoring the tooth on a subsequent day. If you need to place the restoration the same day, follow these steps to improve esthetics: mechanically remove stain from margins, use a self-cure GI for the restoration or use a sandwich technique of opaque self-cure GI followed by a top layer of composite resin.1,7 Note that any tooth-coloured restoration placed over SDF will be a little dark. Practise applying SDF and restorations on extracted teeth to get comfortable using it.
Conclusion
As you can see, SDF is simple, quick, conservative, inexpensive and very effective. Although it does not restore form and function, it stains and it doesn’t taste great, all of the benefits make SDF an important product to have in your bag of tricks. Many dentists prefer this conservative option as it avoids general anaesthesia for uncooperative patients, it is a safer option for medically-compromised patients and it is a great solution for people in long-term care facilities. SDF can be used for deeper lesions to avoid pulp exposure, to prevent and arrest root caries and it is a cheaper option than restorations. As you can see, there are many uses and advantages of SDF. Why not give your patients a conservative option in stopping and preventing decay and decreasing sensitivity?
Oral Health welcomes this original article.
References
- Horst, J. A., Ellenikiotis, H., & Milgrom, P. L. (2016). UCSF Protocol for Caries Arrest Using Silver Diamine Fluoride: Rationale, Indications and Consent. Journal of the California Dental Association, 44(1), 16-28.
- Oral Science: Advantage Arrest. (n.d.). Retrieved September 07, 2020 from https://oralscience.com/en/products/advantage_arrest/
Sarvis, Elise & Karp, Jeffrey. - (August 5, 2016). Silver Diamine Fluoride Arrests Untreated Dental Caries But Has Drawbacks. American Academy of Pediatrics. Retrieved September 07, 2020 from https://www.aappublications.org/news/2016/08/05/SilverDiamine080516
- Chibinski AC, Wambier LM, Feltrin J, Loguercio AD, Wambier DS, Reis A. Silver Diamine Fluoride Has Efficacy in Controlling Caries Progression in Primary Teeth: A Systematic Review and Meta-Analysis. Caries Res. 2017;51(5):527-541.
- Gao SS, Zhao IS, Hiraishi N, et al. Clinical Trials of Silver Diamine Fluoride in Arresting Caries among Children: A Systematic Review. JDR Clin Trans Res. 2016;1(3):201-210.
- Crystal YO, Janal MN, Hamilton DS, Niederman R. Parental perceptions and acceptance of silver diamine fluoride staining. J Am Dent Assoc. 2017;148(7):510-518.
- MacLean, Jeanette. (August 2017). Top 5 Misconceptions about silver diamine fluoride. Jeanette MacLean. August 2017. Dentaltown.com. pp. 89-93.
- Riva Star. (n.d.) Retrieved September 07, 2020, from https://www.sdi.com.au/en-ca/product/rivastar/
- Ontario Dental Association. Ontario Dental Association Suggested Fee Guide 2020. Toronto: ODA 2020.
About the Author
 Dr. Sanjukta Mohanta graduated from the University of Toronto’s Faculty of Dentistry in 1999. She volunteers for the Halton Peel Dental Association, the Ontario Dental Association and the Canadian Dental Association. She is involved in community service, oral health promotion, education and advocacy. She is a general dentist at a community health centre in Brampton, ON.
Dr. Sanjukta Mohanta graduated from the University of Toronto’s Faculty of Dentistry in 1999. She volunteers for the Halton Peel Dental Association, the Ontario Dental Association and the Canadian Dental Association. She is involved in community service, oral health promotion, education and advocacy. She is a general dentist at a community health centre in Brampton, ON.
RELATED ARTICLE: Silver Diamine Fluoride Unstained and Liberated










