
Introduction
Local anesthesia forms the backbone of pain control techniques in dentistry. Local anesthetics represent the safest (when used properly) and most effective drugs for the prevention and management of perioperative and post-operative pain.
The first known injection of a local anesthetic (1885) was an inferior alveolar nerve block administered by the famed medical surgeon Dr. William Stewart Halsted (1852–1922).1 The drugs injected were the combination of cocaine and epinephrine. The dental profession quickly adopted local anesthesia as its primary means of controlling pain eschewing general anesthesia that had been, along with no anesthesia, the techniques of choice prior to 1885.
The introduction, in 1905, of procaine (2% with epinephrine 1:50,000), led to a rapid increase in the use of local anesthesia by dentists and to the burgeoning of access to dentistry for millions of people worldwide.2 Known everywhere by its primary proprietary name ‘Novocain,’ procaine is synonymous, to most people, as the ‘shot’ you receive when you visit the dentist.
The amino-ester local anesthetics (LAs), primarily procaine, propoxycaine and tetracaine, were the drugs used from 1906 until the mid-1940’s when Astra Pharmaceuticals, in Sweden, synthesized and introduced the first amino-amide local anesthetic, lidocaine (Xylocaine) in 19483 (Fig. 1). The demonstrably superior clinical characteristics of lidocaine compared to the most commonly used esters in dentistry led to its rapid adoption and to the development of other drugs in this same category. The amide local anesthetics mepivacaine (1960), prilocaine (1965), bupivacaine (1972), and etidocaine (1976), were ‘borrowed’ from medicine for use in the dental profession. The ester local anesthetics are rarely employed today for pain control in the dental profession, worldwide.
FIGURE 1. Chemical formula of procaine (ester), lidocaine (amide) and articaine.
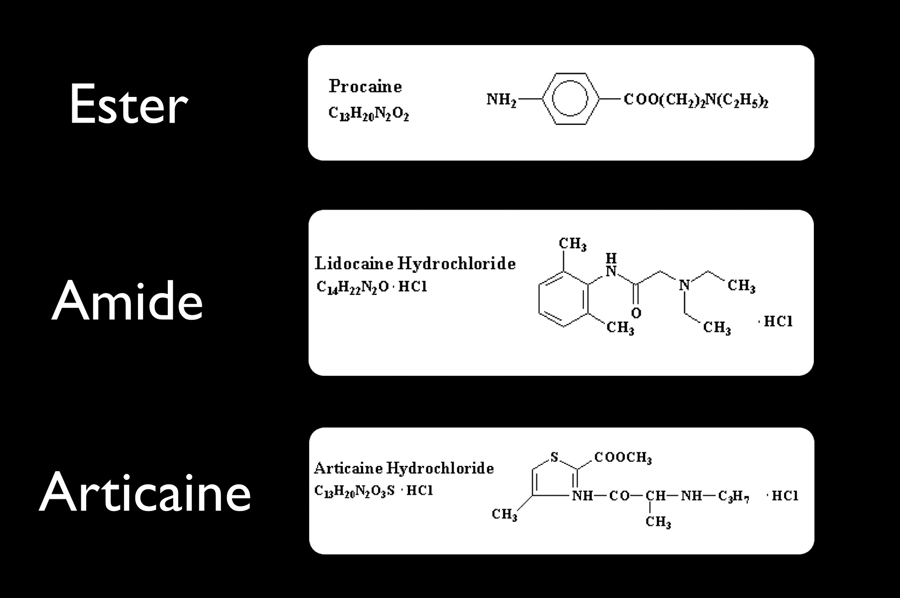
Carticaine, first prepared by Rusching and colleagues in 1969, had its generic name changed to articaine when it entered clinical practice in Germany in 1976.4 Its use gradually spread, entering North America in Canada in 1983.5 The United Kingdom launched the drug in 1998, the United States in 2000, and Australia in 2005. Articaine represents the first, and still only, local anesthetic developed specifically for use in dentistry. Though articaine is classified as an amide LA, articaine possesses chemical characteristics of both the amide and ester groups (Fig. 1). It has become an extremely popular local anesthetic wherever it has been made available. In 2014, articaine was the second most used local anesthetic in the United States with a 34.86% market share (lidocaine was first at 49.35%).6 In Australia 70% of dentists use articaine.7 In 2012, in Germany, where the drug was introduced in 1976, 97% of local anesthetic use by dentists was articaine.8 Articaine is being used increasingly by the medical profession.9
Articaine – Chemistry and Pharmacokinetics
Articaine is 4-methyl-3(2-[propylamino]propionamido)-2-thiophenecarboxylic acid, methyl ester hydrochloride with a molecular weight of 320.84. It is the only amide local anesthetic that contains a thiophene ring. In addition, articaine is the only widely used amide local anesthetic that also contains an ester linkage (Fig. 1). Ester LAs undergo metabolism (biotransformation, detoxification) as soon as the drug diffuses into capillaries and veins (hydrolysis by plasma esterase). Amide LAs enter the blood as still active drugs, circulating throughout the body until they enter the liver where they undergo metabolism by hepatic microsomal enzymes. Unlike the other amide local anesthetics that undergo metabolism in the liver, the biotransformation of articaine occurs in both the liver and in plasma.
The elimination (beta) half-life of a drug is the time required to decrease its blood (plasma) level or concentration by 50%. It is commonly stated that a drug is ‘gone’ (eliminated) from the body in six half-lives (The blood level has actually decreased by 98.25% at six-half lives).
The elimination half-lives of esters and amides are found in Table 1. Elimination half-lives of esters is comparatively short to those of the amides. Procaine has a half-life of 6 minutes, lidocaine approximately 90 minutes. It is important to remember that the half-life of a drug has absolutely no relevance to the clinical duration of action of that drug. A drug is clinically effective as long as it remains in its target organ (e.g. inferior alveolar nerve) in a high enough (therapeutic) concentration. The clinical action (e.g. ‘anesthesia’) of the drug ceases when it diffuses out of the target organ into capillaries and veins. It is then that the elimination half-life starts.
TABLE 1. Elimination half-lives of local anesthetics.
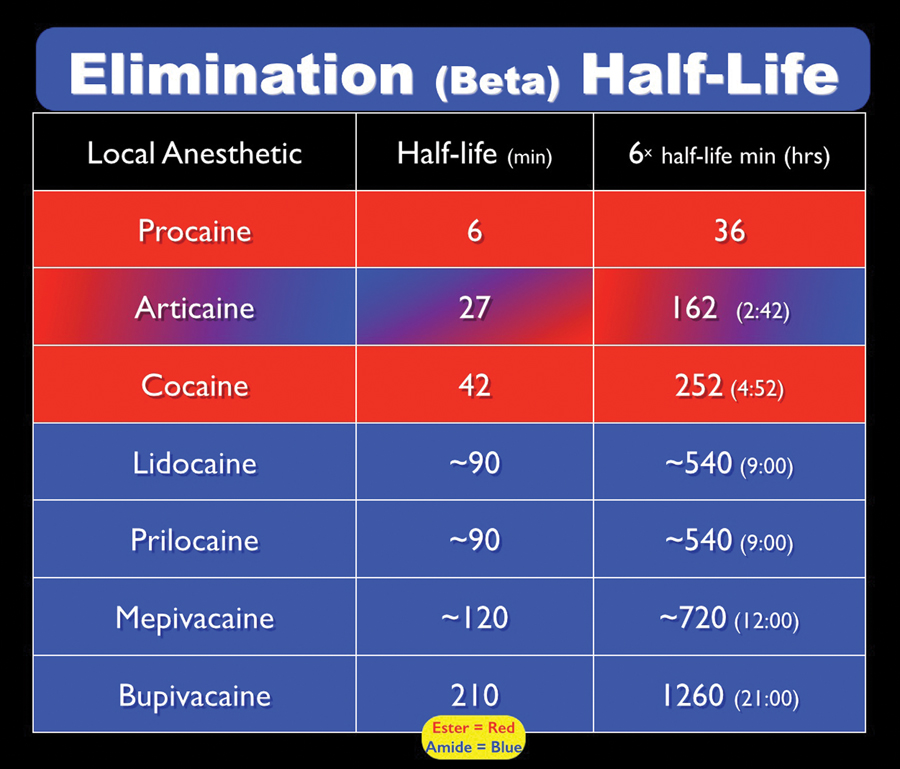
Articaine, possessing both ester and amide characteristics, has an elimination half-life of approximately 27 minutes. It is eliminated from the blood in 162 minutes (2 hours 42 minutes). This becomes clinically significant when treating (1) pregnant patients, (2) nursing mothers, and (3) lighter weight patients (persons weighing less than 30 kg).
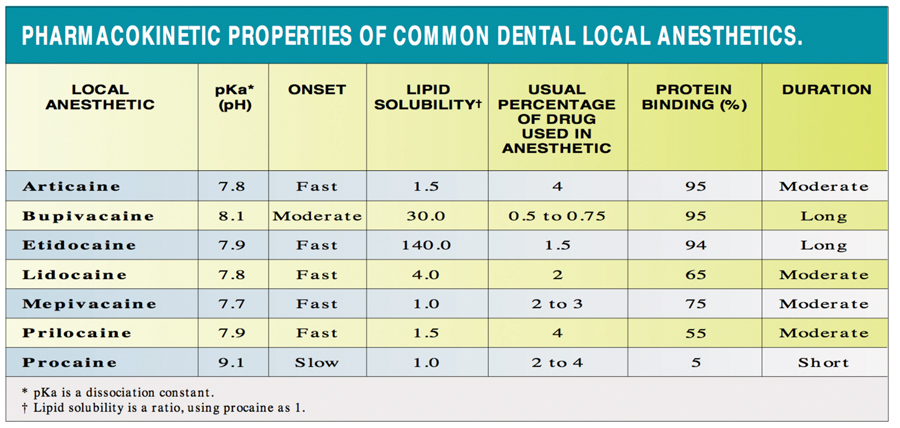
Articaine has many of the physicochemical properties of the most commonly used local anesthetics (lidocaine, mepivacaine and prilocaine) with the exception of the aromatic ring and its degree of protein binding (Table 2). Articaine effectively penetrates tissue and is highly diffusible. Its plasma protein binding of approximately 95 percent is higher than that observed with many local anesthetics. Additionally, the thiophene ring of articaine increases its liposolubility.
TABLE 2. Physicochemical characteristics of common LAs.
Articaine and Allergy
The incidence of true, documented and reproducible allergy to amide LAs is exceptionally low, though alleged ‘allergy’ is reported occasionally. True allergy to the ester LAs is – though still quite rare – more common. The immunogenic potential of articaine is very low. Historical experiences indicate that allergic reactions resulting from sensitivity to articaine are rare. However, all LA solutions with a vasoconstrictor (e.g. epinephrine) contain the antioxidant, sodium bisulfite, which can cause allergic reactions. Allergic reactions that have been reported with articaine include edema, urticaria, erythema and anaphylactic shock. In three studies (number of subjects = 1332) comparing articaine 4% with epinephrine 1:100,000 to lidocaine 2% with epinephrine 1:100,000, reports of rash or pruritis were no more frequent with articaine (n = 2) than with lidocaine (n = 4), and no serious allergic reactions were seen in either treatment group. Patients allergic to articaine likely would be allergic to lidocaine and the other amide local anesthetics.10-12 Furthermore, the allergen paraminobenzoic acid (PABA), a frequent metabolite of ester metabolism, is not a byproduct of the hydrolysis phase of articaine.13
As articaine possesses a sulfur-containing thiophene ring (Figure 1) this author is frequently asked if a patient having a sulfa, sulfite or sulfur allergy represents a contraindication to its administration. The answer is ‘no’. The ‘S’ in articaine is an integral part of the thiophene ring and as such cannot be ‘seen’ or recognized by the patient’s immune system.
Methemoglobinemia has been shown to develop with some types of local anesthetics. Clinical tests of articaine, bupivacaine and etidocaine administered as central nerve block anesthetic for urological procedures (n = 103) indicated no elevation of methemoglobin with articaine.14
Articaine – Clinical Characteristics
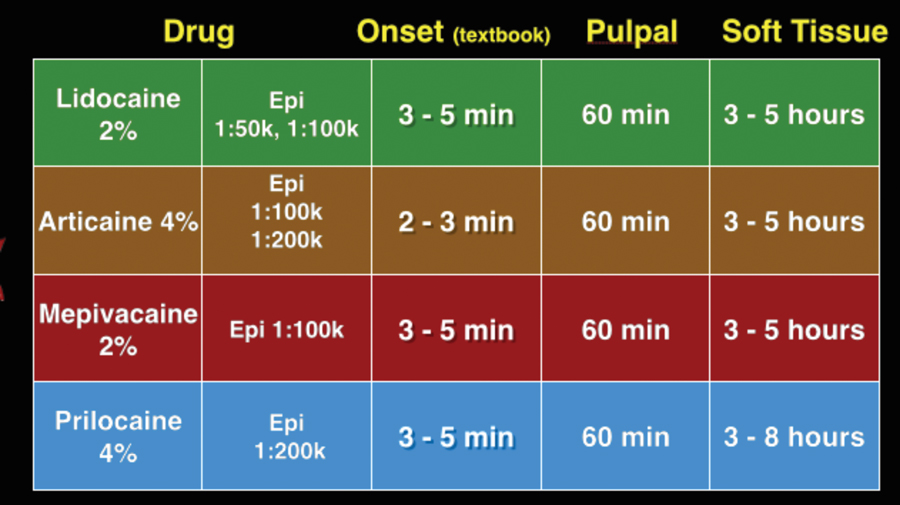
The clinical preparations of articaine in North America – 4% with 1:100,000 and 1:200,000 epinephrine – are classified as intermediate duration local anesthetics (Table 3). Patients responding normally to the drug (normo-responders on a ‘bell-shaped curve’) should experience pulpal anesthesia of approximately 60 minutes duration and soft tissue anesthesia of between three to five hours duration. Duration of pulpal anesthesia is of slightly longer duration following nerve block compared with infiltration.15 The depth and duration of anesthesia are the same with both epinephrine concentrations.
TABLE 3. Intermediate duration LAs north america.
Many doctors report that ‘in their opinion’ the onset of anesthesia following both infiltration and nerve block with articaine is more rapid than with other local anesthetics. This assertion is not supported by clinical research.10,16 In studies including a combined 1554 patients there was no clinical difference noted in the onset of pulpal anesthesia following inferior alveolar nerve block between 2% lidocaine, epinephrine 1:100,000 and 4% articaine epinephrine 1:100,000.
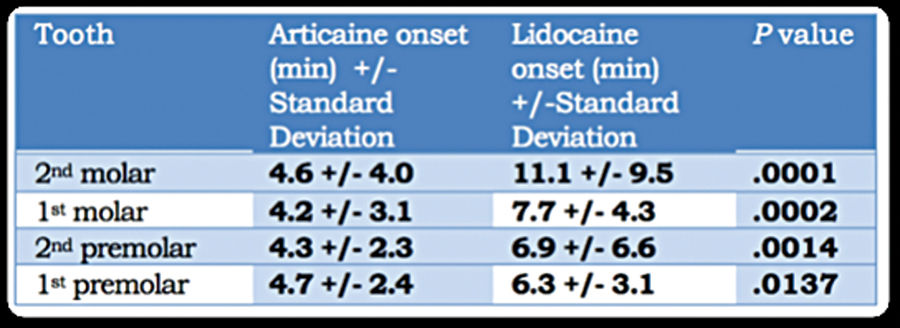
However, the administration of articaine by mandibular infiltration in adults has been shown to be significantly more effective in providing pulpal anesthesia than lidocaine infiltration when used as a sole injection for mandibular anesthesia.17 Successful pulpal anesthesia was assessed (using electric pulp tester [EPT]) following articaine or lidocaine infiltration of 1.8 mL in the buccal fold adjacent to the mandibular 1st molar. Table 4 shows the percentages of successful pulpal anesthesia (Table 4). Onset time for pulpal anesthesia was also considerably more rapid with articaine than lidocaine (Table 5). The result was attributed to articaine’s thiophene ring, which is more lipid-soluble than the benzene ring found in other local anesthetics.
TABLE 4. Articaine, lidocaine pulpal anesthesia success rates – Robertson, Nusstein etal, reference #16.
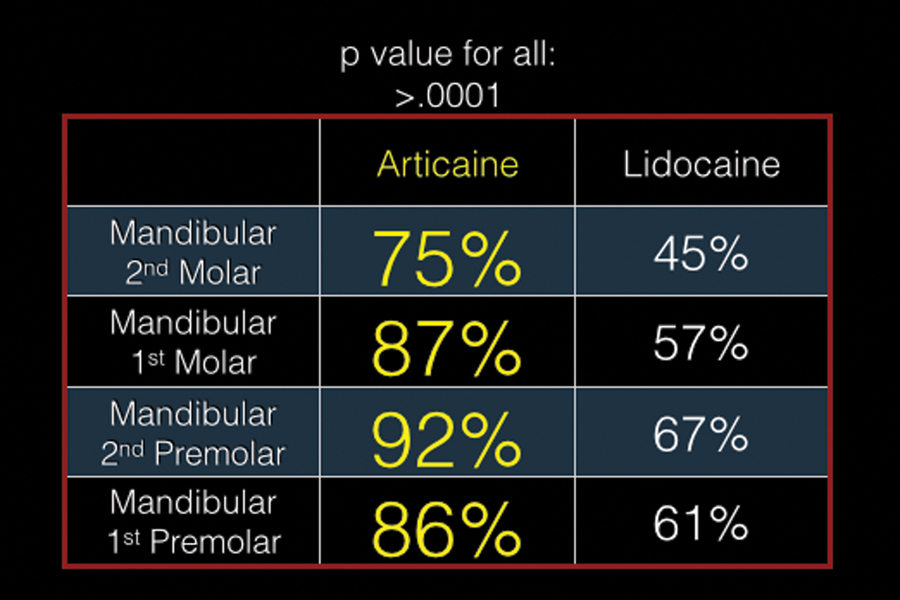
TABLE 5. Articaine, lidocaine onset of pulpal anesthesia – Robertson, Nusstein etal, reference #16.
Meechan and Ledvinka compared the infiltration of 4% articaine with epinephrine 1:100,000 and 2% lidocaine with epinephrine 1:100,000 on mandibular incisors, both for success and duration of pulpal anesthesia.18 Infiltrating 0.5 mL in the buccal fold produced a 94% success rate for articaine compared with 70% for lidocaine. Infiltrating 0.5 mL on both the buccal and lingual of the lateral incisor increased the success rate to 97% for articaine and 88% for lidocaine. The duration of pulpal anesthesia was also significantly longer with both articaine infiltrations. (Table 6). The increased success rate for infiltration in the adult mandible was thought to be due to the fact that the cortical plate of bone, both buccal and lingual, is quite thin and might provide little resistance to infiltration.18
TABLE 6. Lingual nerve involvement in reports of paresthesia.

Given articaine’s ability to diffuse through the thick cortical plate of bone following infiltration in the adult mandible, Kanaa et al looked at the ability of articaine infiltration to increase the success rate of pulpal anesthesia following an inferior alveolar nerve block (IANB) with 2% lidocaine with epinephrine 1:80,000.19 Patients received IANBs at each of two occasions (2.0 mL lidocaine with epinephrine). Then they received either a buccal infiltration of 4% articaine with epinephrine 1:100,000 or a ‘dummy’ injection in the buccal fold by the mandibular 1st molar. The 1st molar and 1st premolar were pulp tested every three minutes for 45 minutes. Results are shown in Figures 2 and 3. In both teeth the additional articaine infiltration significantly increased the success rate of pulpal anesthesia (55.6% to 91.7% for 1st molar; 66.7% to 88.9% for 1st premolar). Though the study concluded at 45 minutes there was no indication that pulpal anesthesia was waning at that time.19
FIGURE 1B. Duration of pulpal anesthesia following mandibular infiltration. Meechan, Ledvinka, reference #17.
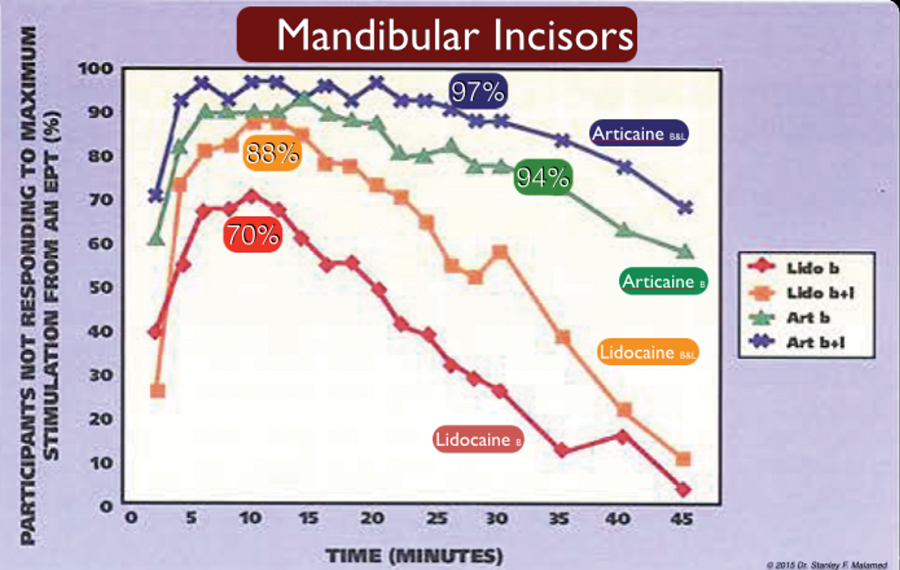
FIGURE 2. & 3. Successful pulpal anesthesia. Blue = IANB – Lidocaine 2% + epi 1:80,000 + “dummy” infiltration. Purple = IANB – Lidocaine 2% + epi 1:80,000 + “articaine” infiltration. Reference #18.


Articaine in Special Patient Populations: Pregnancy, Nursing and Pediatrics.
In the United States the Food and Drug Administration classifies drugs by their safety during pregnancy and nursing.20 The author is unaware of similar listings by Health Canada (www.hc-sc.gc.ca).
Pregnancy: All injectable local anesthetics, including articaine, and epinephrine, are classified as ‘B’ [Caution advised – no evidence of 2nd or 3rd trimester risk; fetal harm possible but unlikely] or ‘C’ [Weigh risk/benefit – weigh possible fetal risk vs. maternal benefit; see package insert for drug-specific recommendations]. Lidocaine and prilocaine are ‘B’ rated, all other local anesthetics (including articaine), and epinephrine are ‘C’. To minimize exposure of the fetus to the effects of the local anesthetic drug, a drug with a shorter elimination half-life is preferred. The 27-minute half-life of articaine is preferable to the 90-minute or greater half-life of the other available local anesthetics.
Nursing: FDA categories for nursing infants are ‘S’ (Safe for nursing infant); ‘S?’ (Safety in nursing infants unknown); ‘S*’ (Potential for significant effects on nursing infants) and ‘NS’ (Not safe for nursing infants).20 Lidocaine is the only ‘S’ local anesthetic. All others are ‘S?’ including epinephrine (in dental concentrations). As nursing mothers are normally reluctant to expose their infant to any drug that child does not need, it is not uncommon in the dental environment to have a nursing mother in need of dental care ask their dentist, ‘Will the drug (e.g. lidocaine) be in the milk?” The answer will always be ‘Yes.’ The mother immediately states that they do not want the drug. This becomes problematic when the dental procedure is potentially painful. The concept of “pump and discard’ successfully handles this situation. Following exposure to a drug the nursing mother should pump and discard the milk for a period covering six elimination half-lives of the drug administered. For all local anesthetics except articaine this is a period of nine hours. The FDA states ‘When using articaine, nursing mothers may choose to pump and discard breast milk for approximately four hours (based on plasma half life) following an injection of articaine (to minimize infant ingestion) and then resume breastfeeding.”
Pediatrics: All local anesthetics can produce seizures (a classic local anesthetic overdose manifests as a generalized tonic-clonic convulsion) if their blood level becomes elevated above the seizure threshold for that drug. One cartridge of any local anesthetic administered rapidly (<10 seconds) intravenously will induce a rapid onset severe seizure. Aspiration for blood prior to administration of a local anesthetic and slow injection of the drug can prevent this from occurring.
Most local anesthetic overdoses, however, develop as a result of the overadministration of the drug. Once injected into the oral cavity the local anesthetic will be absorbed into capillaries and a blood level of the drug becomes detectable. Local anesthetic overdose is most likely to occur in patients weighing under 30 kg (66 lb.), who are well-behaved and in need of multiple quadrants of dental care.21 Of the amide local anesthetics, articaine – because of its 27-minute elimination half-life – is least likely to induce an overdose resulting from the administration of too many cartridges.
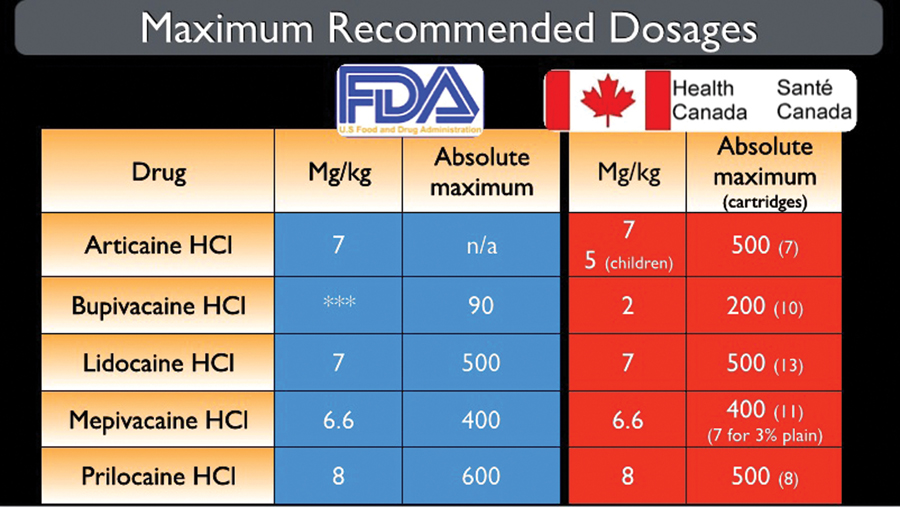
Maximum recommended doses (MRDs) of local anesthetics are provided by the US FDA (Table 7). Though Health Canada does not specify MRDs, there are authoritative Canadian publications listing recommended maximum doses that are generally considered the ‘standard of care’ in Canada.22 Some subtle differences are noted in several of the available formulations. In the USA, the articaine MRD is 7 mg/kg, with no absolute dose listed (due to its 27-minute elimination half-life). In Canada the dose for adults is 7.0 mg/kg. with an absolute maximum of 500 mg, and 5.0 mg/kg for ‘children.’
TABLE 7. MRD: USA – Food & Drug Administration, Canada – various sources
To summarize the clinical characteristics of available articaine formulations, it is a 4% solution containing epinephrine in either a 1:100,000 or 1:200,000 concentration. Cartridges contain 72 mg. of articaine. (Recent labeling changes state the cartridge contains a ‘minimum volume of 1.7 mL. A clinical study determined the actual volume of both lidocaine and articaine cartridges to be 1.76 mL +/- 0.02 mL.17 Both formulations provide a rapid onset of pulpal anesthesia (approximately 2 to 5 minutes), pulpal anesthesia of approximately 60 minutes in duration, and residual soft tissue anesthesia lasting between 3 to 5 hours,15 similar to other amide local anesthetics containing epinephrine. Because of articaine’s greater lipid solubility, the drug demonstrates increased clinical success when administered by mandibular infiltration in molars, premolars and incisors. Reports of palatal soft tissue anesthesia developing after articaine maxillary infiltration in the buccal fold, though anecdotal, can be attributed to the drugs greater lipid solubility.
As a result of it undergoing metabolism in the plasma (as well as in the liver) articaine is a preferred local anesthetic during pregnancy, nursing and in lighter-weight patients (<30 kg).
Articaine and Paresthesia
As described above, articaine possesses significant advantages over the other currently available local anesthetic formulations. However, there have been reports that the administration of 4% local anesthetic formulations by inferior alveolar nerve block is associated with a greater risk of paresthesia than that of 2% and 3% formulations.23-26 As a result of these reports, regulatory bodies in the province of Ontario, Canada, have cautioned against the dental use of 4% local anesthetics by inferior alveolar nerve block.27,28
What is paresthesia? Stedman’s Medical Dictionary29 defines a paresthesia as an abnormal sensation, such as of burning, pricking, tickling, or tingling. Paresthesias are one of the more general groupings of nerve disorders known as neuropathies. Paresthesias may manifest as total loss of sensation (e.g., anesthesia), burning or tingling feelings (ie, dysesthesia), pain in response to a normally non-noxious stimulus (ie, allodynia), or increased pain in response to all stimuli (e.g., hyperesthesia).30
For simplicity’s sake, the term paresthesia will be used to encompass all forms of nerve dysfunction. We will define paresthesia as a “persistent anesthesia or altered sensation well beyond the expected duration of anesthesia.” Symptoms can vary significantly, including sensations of numbness, swelling, tingling and itching, tongue biting, drooling, loss of taste, and speech impediment.23,31-34
Prior to delving into this subject there are a number of ‘truisms’ regarding anatomy, injections and local anesthetics that need to be considered.
1. Anatomy: Everybody is different. We teach technique based on ‘normal’ anatomy (e.g. insert needle here, advance 25 mms, aspirate, deposit the drug). We hope, or it is assumed that, the nerve is in the area – if the patient’s anatomy is ‘normal.’
2. Injections: Once a needle penetrates skin or mucous membrane, every injection is blind. In most intramuscular (IM) injections when therapeutic drugs are being administered, the site selected for IM administration is one that it is considered anatomically ‘safe’. The vastus lateralis muscle (located in the anterior lateral portion of the thigh) is considered the safest place in the human body to administer an IM injection with minimal risk of damaging important structures (e.g. nerves, arteries, veins). Local anesthetic administration in dentistry is different. Consider that with a local anesthetic injection we are ‘aiming’ to deposit a volume of local anesthetic solution as close to the ‘target nerve as possible (a few millimeters) so the deposited local anesthetic can diffuse into it and block nerve conduction. Yet, we cannot ‘see’ where the needle tip actually is located.
3. Local anesthetics: Local anesthetics are chemicals that transiently (hopefully) interrupt the normal functioning of a nerve (they interrupt the nerves ability to conduct a nerve impulse either to [sensory nerve] or from [motor nerve] the brain).
4. Local anesthetics: All local anesthetics are neurotoxic – they can damage nerves. Miller, in his seminal textbook on anesthesia35 has stated “All the clinically used local anesthetics can produce direct toxicity to nerves if they achieve sufficiently high intraneural concentrations.” In the United States the dental local anesthetic producing the greatest number of reports of paresthesia is lidocaine. Lidocaine is also the most used local anesthetic in dentistry in the United States.6,36,37
5. Paresthesia: Paresthesia has existed ever since injections were first administered. References to paresthesia associated with the administration of local anesthetics, both in medicine38 and dentistry,31-33,39-41 predate the introduction of articaine in North America by decades.
The first publication to address the incidence of paresthesia following the administration of 4% local anesthetics appeared in 1995.23 Reviewing reports of paresthesia from dentists in the province of Ontario, Canada to the Provincial Insurance Commission, Haas and Lennon reported an overall risk of paresthesia following injection of local anesthetic of 1 case in 785,000 (1:785,000). Two and three percent LAs (mepivacaine, lidocaine) had an incidence of 1:1,250,000. The two 4% LAs, prilocaine and articaine had reported risks of 1:588,235 and 1:440,529 respectively.
This paper has become the most cited reference purporting to demonstrate that 4% LAs are associated with a greater risk of paresthesia. Virtually all papers reporting increased risk of paresthesia from articaine ultimately cite this reference as their initial source.
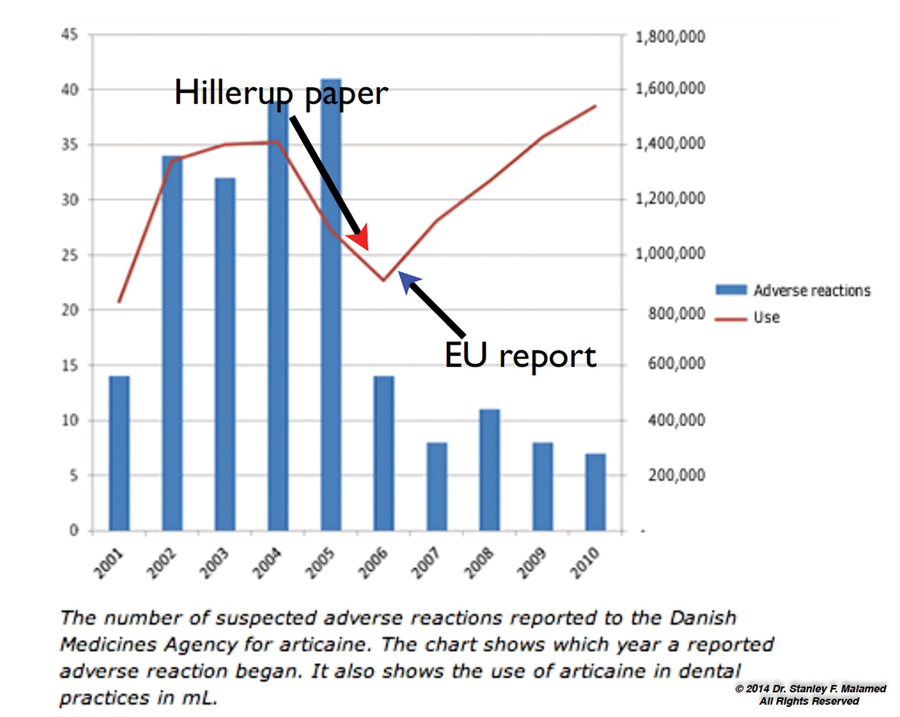
Articaine was introduced into Denmark in 2001 and by 2005 had garnered 35% of the dental local anesthetic market.24 A 2006 paper by Hillerup and Jensen reported that articaine was the drug most often associated with reports of paresthesia by dentists to the Danish Medicines Agency (Laegemiddel Styrelsen). The paper recommended that “Until factual information is available, a preference of other formulations to Articaine 4% may be justified, especially for mandibular block analgesia.”24 As a consequence of this paper the Danish Dental Association recommended that articaine not be used by inferior alveolar nerve block.
The Pharmacovigilance Working Party of the European Union (the EUs equivalent of the United States FDA and Canada’s TGA) investigated the question of paresthesia and dental local anesthetics, specifically articaine.42 They reviewed the use of articaine in 57 countries, estimating that approximately 100 million dental patients received articaine annually. Their findings, published 20 October 2006 stated “regarding articaine, the conclusion is that the safety profile of the drug has not significantly evolved since its initial launch. Thus, no medical evidence exists to prohibit the use of articaine according to the current guidelines listed (in) the summary of product characteristics.”
The report went on to state: “All local anaesthetics may cause nerve injury (they are neurotoxic in nature). The occurrence of sensory impairment is apparently slightly more frequent following the use of articaine and prilocaine. However, considering the number of patients treated, sensory impairments rarely occur. For example, the incidence of sensory impairment following the use of articaine is estimated to be 1 case in 4.8 million treated patients.”…“Nerve injuries may result from several incidents: Mechanical injury due to needle insertion; Direct toxicity from the drug; Neural ischaemia.” And finally: “There is no need for new experimental studies or clinical trials.”42
In October 2011 the Danish Medicines Agency followed up with this report: “The Danish Medicines Agency’s database of side effects contain 160 reports on adverse reactions from articaine that occurred from 2001-2005. The adverse reactions are mainly sensory impairment and nerve damage. Since 2005, we have seen a drop in the number of reports of new adverse reactions, up until 1 October 2011, we have received 2 reports on suspected adverse reactions from articaine which occurred in 2011. In both cases, the patients have experienced sensory impairment after treatment with articaine.”43
This is an example of two phenomena: (1) the Weber Effect and (2) the effect of publicity, either negative or positive, on drug prescription and usage (Fig. 4).
Articaine was introduced into the United States in June 2000 and, as in most countries, quickly became a popular dental local anesthetic. In 2014 articaine was the 2nd most administered local anesthetic (34.86% market share) in dentistry in the USA.6 A 2010 paper by Garisto et al reviewing 248 reports of paresthesia to the United States FDAs Adverse Event Reporting System (AERS) occurring following dental procedures over an 11-year period (1997 – 2008) concluded that “Reports involving 4% prilocaine and 4% articaine were 7.3 and 3.6 times, respectively, greater than expected on the basis of local anesthetic use by U.S. dentists.”44 The relative risks of paresthesia from this paper are shown in Table 8, compared with the same drugs in the 1995 Ontario paper.
TABLE 8. Comparative incidence of paresthesia reported in USA and Ontario.
![Table 8[1]](https://media.oralhealthgroup.com/uploads/2016/02/Table-81.jpg)
Regarding articaine, it appears from the numbers in these two papers that the risk of paresthesia is 9.4 times greater in Ontario than in the United States. The overall risk of paresthesia from a dental local anesthetic injection in Ontario is 17.58 times greater.23,44
Regarding the AERS data base, the following is posted on its website:45 “AERS data do have limitations. First, there is no certainty that the reported event was actually due to the product. FDA does not require that a causal relationship between the product and event be proven. Furthermore, FDA does not receive all adverse event reports that occur with a product.” (authors note: it is estimated that only about 10% of all adverse events are reported). “Many factors can influence whether or not an event will be reported, such as the time a product has been marketed (Weber Effect) and publicity about an event. Therefore, AERS cannot be used to calculate the incidence of an adverse event in the US population.”45
Resolution of paresthesia was reported in 108 of the 248 cases, with complete resolution occurring between 1 day and 736 days. Confirmed resolution of the paresthesia was reported in 34 of the 108 cases. Of these, 25 resolved in less than 2 months with the remaining 9 resolving within 240 days.44 92.7% of the reports involved the lingual nerve (89.0% lingual nerve alone, 3.7% both lingual and IA nerves).44
Articaine was approved for use in 2005 in Australia. It was reported in a (January) 2012 paper that 70% of Australian dentists were using articaine in their clinical practices.7 However, a (December) 2011 paper in the same journal, cited 5 case reports of paresthesia following local anesthetic administration, concluded that “Careful consideration needs to be given before using higher concentration local anaesthetic agents for mandibular and lingual blocks as lower concentration local anaesthetics are safer.” The report also stated that, “It is safe to use the higher concentration agents for infiltrations way from major nerves.”26 Four of the five reported cases involved paresthesia of the lingual nerve only, and in two of these cases an ‘electric shock’ was experienced by the patient during injection.
Citing this paper, the 2012 edition of the Australian Dental Associations Therapeutic Guidelines (Oral and Dental) stated: “Articaine has been claimed to be more effective, but there are reports of an increased risk of neurotoxicity, presenting as prolonged numbness in the areas of distribution, often with pain. This may be due to the higher concentration of the solution rather than to the anaesthetic itself. Consequently, it is recommended that articaine should not be used for regional blocks (e.g. inferior alveolar).28
The Weber Effect and the Effect of Publicity on Drug Usage
The Weber Effect, named after the epidemiologist, Dr. JCP Weber46 is an epidemiological phenomenon which states that the number of reported adverse reactions for a drug rises until about the middle to end of the 2nd year of marketing, peaks, and then steadily declines despite steadily increasing prescribing rates.”
The validity of the Weber Effect has been challenged and demonstrated to be verifiable.47 Hartnell and Wilson attempted to ‘validate or refute a widely accepted epidemiological phenomenon known as the Weber effect by replicating Weber’s original observation by using drugs (author’s note – NSAIDs) that were marketed in the United States and using reports from a U.S. database.” They concluded “The Weber effect was replicable.”47
Publicity affects drug prescribing and usage habits. Following the Danish Dental Associations ‘recommendation’ to avoid the use of articaine by inferior alveolar nerve block (IANB), its use in Denmark declined significantly (Fig. 4, red line). In 2006 following the European Unions report stating there was no scientific evidence of an increased risk of paresthesia from articaine, use of the drug increased.
FIGURE 4. Articaine sales (red line) and adverse event reports (blue bars) in Denmark, 2001-2010, reference #42.
Paresthesia Following Non-Surgical Dental Treatment
Surgery, especially 3rd molar extraction and placement of mandibular implants, is the primary cause of paresthesia following dental treatment.48,49 Informed consent, specifically discussing the risk of paresthesia is required prior to these procedures.
Given that most dental treatment is non-surgical (e.g. restorative, periodontal), the primary risk of paresthesia would involve local anesthetic administration.
In a Medline search for reported cases of paresthesia in dentistry dating to 1946, more than 95% of all cases occurred in the mandible.50 The overwhelming percentage involve the lingual nerve. Table 6 shows lingual nerve involvement in four published articles.
Considering we have been told that 4% articaine appears to be more neurotoxic than other local anesthetic formulations, and that its administration by inferior alveolar nerve block should be avoided, the following needs to be considered: If 4% articaine is more neurotoxic than other local anesthetics, then how do we explain that paresthesia is rarely reported in the maxilla when half of all dental treatment involves maxillary teeth? (<5% of all cases in the dental literature dating to the 1950s involve the maxilla).50 Considering the mandible, paresthesia has not been reported following alternative nerve blocks, such as the Gow-Gates mandibular nerve block.50 Articaine has been used increasingly in medicine, primarily dermatology, plastic and reconstructive surgery, ophthalmology and orthopedic surgery. There are no reported cases of paresthesia following the non-dental use of articaine.9,51
Is it possible for a drug to be so specifically neurotoxic that it only damages nerves with the oral cavity, specifically in the mandible and more specifically the lingual nerve?
The Lingual Nerve
The lingual nerve appears to be involved in reports of dentally-related paresthesia a disproportionate percentage of cases. (Table 6). Pogrel has studied paresthesia, with publications dating to the early 1990s.31-33 In a 2000 paper, Pogrel and Thamby estimated the risk of permanent nerve damage following IANB at 1 in 26,762 injections.52 They stated that “it is reasonable to suggest that during a career, each dentist may encounter at least one patient with an inferior alveolar nerve block resulting in permanent nerve involvement. The mechanisms are unknown and there is no known prevention or treatment.”52 In the course of a twenty- to thirty-year dental career, it is estimated that more than 30,000 IANBs will be administered.52
Why is it that the lingual nerve is primarily involved in cases of paresthesia? Considering that when administering the IANB the vast majority of local anesthetic volume is deposited close to the IAN (e.g. 1.3 to 1.5 mL), not the lingual nerve (e.g. 0.2 to 0.3 mL), if paresthesia was a local anesthetic neurotoxic phenomenon, we would expect the IAN to be affected much more often than the lingual nerve.
The fact that the lingual nerve is stretched when the patient opens their mouth for an IANB probably prevents the lingual nerve from ‘getting out of the way’ of the needle. The resulting injury is more likely than not to be a result of mechanical trauma to the lingual nerve from the metal needle. Stated in another manner: “the lingual nerve is in the way.”
A 2003 paper by Pogrel et al attempted to explain why lingual nerve damage was commonly seen as more profound.53 At the level at which the injection is administered, the inferior alveolar nerve had 5 to 7 fascicles, whereas the lingual nerve in that area usually had around three, but in a third of the cases was actually unifascicular in the area where the IANB was given.53 (Fig. 5) If a nerve with many fascicles (e.g. IANB) is damaged, only a small portion of the sensory distribution would be affected. When a nerve with 1 to 3 fascicles (e.g. lingual nerve) is damaged, the resulting area of sensory involvement will be considerably larger.
FIGURE 5. Fascicles within a nerve.
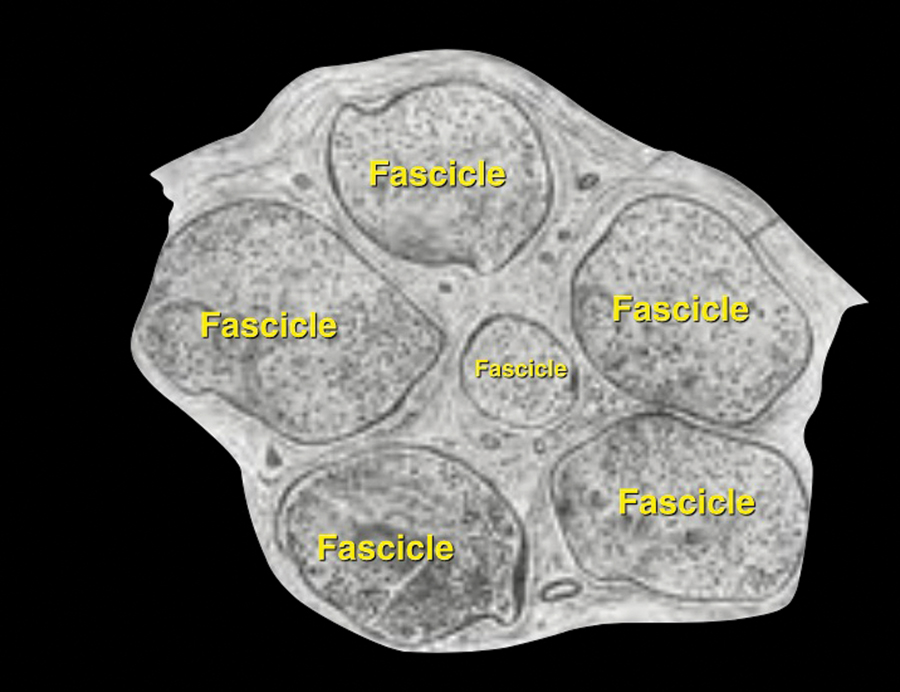
It is this author’s opinion that if paresthesia involves the distribution of the lingual nerve – and especially when an ‘electric shock’ (e.g. ‘zap’) is experienced during injection, the cause is likely to be mechanical trauma caused by direct contact of the metal needle with the nerve. If paresthesia involves the distribution of the IAN (e.g. chin, lip, mucous membrane) then possible etiologies include (1) neurotoxicity of the LA, (2) mechanical contact of the needle to the IAN, (3) edema, and (4) hemorrhage.
Local Anesthetics are Neurotoxins
All local anesthetics are neurotoxic. If all local anesthetics were equally neurotoxic than the percentage of reported cases of paresthesia for the drug should be equal to its market share. The resulting fraction ideally should be 1.0.
In Pogrel’s 2007 paper36 of 52 patients, lidocaine produced the greatest number (20) and percentage (35%) of cases of paresthesia. However, with a market share of 54% at the time the ratio was 0.64, better than expected. (Table 9). Prilocaine, on the other hand, with a 6% market share was involved with 29.8% (N=17) of the cases of paresthesia (4.96 ratio). Articaine with a market share of 25% had a 29.8% (N=17) involvement for a ratio of 1.19. Pogrel concluded “Therefore, using our previous assumption that approximately half of all local anesthetic used is for inferior alveolar nerve blocks, then on the figures we have generated from our clinic we do not see a disproportionate nerve involvement from articaine.”36
TABLE 9. Market share and observed incidence of paraesthesia.

In a 2012 update reporting on 38 patients seen in his clinic between 2006 and 2011, Pogrel stated that “articaine is still causing permanent inferior alveolar and lingual nerve damage (36%) which is proportionate to its market share (37%).”37 “The number of cases caused by lidocaine, on the other hand, appears to be only around 50% of its market share.” Prilocaine however by causing 26% of all cases seen since 2005 with a market share of only 8% is somewhat disproportionate to its market share.”37 Table 9 shows the results of the two papers.

Is Articaine a More Effective Local Anesthetic and Does it Have a Greater Risk of Paresthesia?
Meta-analyses comparing articaine to lidocaine have concluded “that articaine as compared with lignocaine provides a higher rate of anaesthetic success, with comparable safety to lignocaine when used as infiltration or blocks for routine dental treatments.”…“This meta-analysis thus supports a recommendation for 4% articaine (1:100,000 epinephrine) in routine dental practice over and above 2% lidocaine (1:100,000 epinephrine).54,55
A 2012 paper reporting on a histological analysis of the neurotoxicity of lidocaine, articaine and epinephrine on the mental nerve in rats, concluded that “articaine is not toxic to the nervous structure and (that) further studies are necessary to explain the possible relation between articaine injection and paresthesia.”56
In a 2013 clinical study, human neuroblastoma cells were exposed to varying concentrations of articaine, lidocaine and prilocaine to determine neurotoxicity at six different drug concentrations.57 The results of this in-vitro study stated that lidocaine 2% had a lower neurotoxicity profile compared to prilocaine 4% and that articaine 4% had a lower neurotoxicity profile compared to lidocaine 2%. In-vitro studies are accurate, sensitive and reproducible because they are conducted in a controlled environment. However, in-vitro studies do not take into account other factors such as (1) local pharmacokinetics (concentration in tissues, local diffusion, absorption); (2) potential influence of other drugs on local pharmacokinetics (e.g. epinephrine); (3) systemic behavior of the drug after absorption (distribution, elimination, metabolism), and (4) all other variables such as differences between patients.
So, What Should You Do?
Doctors must always consider the benefit to be gained from use of a procedure or drug versus the risk involved in the procedure or drug. Only when, in the opinion of the treating doctor, the benefit to the patient to be gained clearly outweighs the risk should the procedure be done or the drug administered.
All reports claiming an increased risk of paresthesia with articaine are anecdotal. There is no scientific evidence demonstrating an increased risk of paresthesia following the administration of articaine compared with other local anesthetics. Choices for IANB include (1) continuing the use of articaine 4% with epinephrine 1:100,000 or 1:200,000, or (2) if unconvinced or still concerned, use either lidocaine 2% with epinephrine 1:100,000 or mepivacaine 2% with epinephrine 1:100,000 for IANB, following it immediately with a buccal infiltration of 0.6 to 0.9 mL of articaine at the apex of the tooth to be treated.
The administration of 4% prilocaine with epinephrine appears to be associated with a considerably greater risk of paresthesia to the lingual and/or inferior alveolar nerves. OH
Dr. Stanley Malamed is a dentist anesthesiologist and emeritus professor of dentistry at the Herman Ostrow School of Dentistry of U.S.C, in Los Angeles, California.
Oral Health welcomes this original article.
Editors Note:
Oral Health welcomes this original article from the well-respected Dr. Stanley Malamed on articaine. In his review, Dr. Malamed discusses articaine and paraesthesias. It is worth noting that the use of articaine and other 4% local anaesthetic solutions for mandibular blocks has been an actively debated topic for years. With regard to paraesthesias currently, the bulk of the literature suggests a higher-than-expected incidence when higher concentration (4%) local anaesthetic preparations are used. In the interest of presenting topics in a balanced way, and acknowledging Dr. Malamed’s enthusiastic support for the continued use of articaine for inferior alveolar nerve blocks in this article, our readers may wish to also review articles by Dr. Dan Haas and Dr. Søren Hillerup. Drs. Haas and Hillerup are two of the more notable additional authors on the incidence of paraesthesias and some associated factors. Their viewpoint represents a more guarded approach in the use of 4% solutions for mandibular blocks.
Also at issue in this article is the use of articaine in pregnant women. Dr. Malamed suggests that articaine, an FDA C-rated agent should be used instead of B-rated lidocaine. The reason given is the shorter fetal exposure time to articaine because of its faster metabolism. What is not clear is why exposing a fetus to a potentially more harmful drug, even for a shorter time is advantageous.
As always, how you choose to treat your patients is ultimately your decision. At Oral Health, we would like these decisions to be based on the best information available. We hope that you enjoyed Dr. Malamed’s article.
Dr. Peter Nkansah
References:
1. Lopez-Valverde A; De Vicente J; Cutando A. The surgeons Halsted and Hall, cocaine and the discovery of dental anaesthesia by nerve blocking. Br Dent J. 211(10):485-487, 2011
2. Ruetsch YA; Boni T; Borgeat A. From cocaine to ropivacaine: the history of local anesthetic drugs. Curr Top Med Chem. 1(3):175-182, 2001
3. Lofgren N. Studies on local anesthetics: Xylocaine, a new synthetic drug. Stockholm: Hoegstroems, 1948
4.Muschaweck R, Rippel R. Ein neues Lokalanasthetikum (Carticain) aus der Thiophenreihe [A new local anaesthetic (carticaine) in the thiophene series]. Prakt Anaesth 9(3):135-146, 1974
5. Lemay H; Albert G; Helie P; Dufour L; Gagnon P; Payant L; Laliberte R. Ultracaine en dentisterie operatoire conventionnelle. [Ultracaine in conventional operative dentistry]. J Can Dent As soc. 50(9):703-708, 1984
6. Dental local anesthetic market share, United States, Calendar year–2014, 23 April 2015. Septodont Inc. Lancaster, PA
7. Yapp KE; Hopcraft MS; Parashos P. Dentists’ perceptions of a new local anaesthetic drug-articaine. Aust Dent J. 57(1):18-22; quiz 109, 2012
8. Deutcher Dentalmarkt Jahresbericht (DDM) 2010 (German Dental Market Annual Report 2010). GfK HealthCare, Nuremberg, Germany
9. Vree TB; Gielen MJ. Clinical pharmacology and the use of articaine for local and regional anaesthesia. Best Pract Res Clin Anaesthesiol. 19(2):293-308, 2005
10. Malamed SF, Gagnon S, Leblanc D: Efficacy of articaine: a new amide local anesthetic. J Amer Dent Assoc 131(5):635-642, 2000
11. Malamed SF, Gagnon S, Leblanc D: Safety of articaine: a new amide local anesthetic. J Amer Dent Assoc, 132(2):177-185, 2001
12. Malamed SF, Gagnon S, Leblanc D: Articaine hydrochloride in pediatric dentistry: safety and efficacy of a new amide-type local anesthetic. Pediatr Dent 22(4):307-311, 2000
13. Hawkins, JM, Moore, PA. Local anesthesia: advances in agents and techniques. Dent Clin N Amer 46:719-732,2002.
Rupieper N; Stocker L. Haemiglobinspiegel unter Lokalanaesthesie mit Bupivacain, Carticain und Etidocain. [Met-Hb formation and local anesthesia using bupivacaine, carticaine and etidocaine]. Anaesthesist. 30(5):23-25, 1981
15. Ultracaine DS Forte 1:100,000, Drug package insert. HANSAmed, Mississauga, Ontario, Canada, September 2015
16. Malamed SF, Tavana S, Falkel M. Faster onset and more comfortable injection with alkalinized 2% lidocaine with epinephrine 1:100,000. Compendium 34(Spec issue #1):1-11, 2013
17. Robertson D, Nusstein J, Reader A, Beck M, McCartney M. The anesthetic efficacy of articaine in buccal infiltration of mandibular posterior teeth. J Am Dent Assoc 138:1104-1112, 2007
18. Meechan JG, Ledvinka JI. Pulpal anaesthesia for mandibular central incisor teeth: a comparison of infiltration and intraligamentary injections. Int Endod J 35:629-634, 2002
19. Kanaa JM, Whitworth JM, Corbett IP, Meechan JG. Articaine buccal infiltration enhances the effectiveness of lidocaine inferior alveolar nerve block. Int Endod J 42:238-246, 2009
20. United States FDA Pregnancy Categories. http://www.drugs.com/pregnancy-categories.html. Accessed 17 September 2015
21. Malamed SF. Systemic complications, in Handbook of Local Anesthesia, 6th ed. 2013, Mosby Elsevier, St. Louis, pages 313-314
22. Hawkins JM. Local anesthetic maximum doses. Adapted from various sources, 2012. Dr. J Mel Hawkins, Anesthesia Services for Dentistry, Inc. Toronto, ON, Canada
23. Haas DA, Lennon D : A 21 year retrospective study of reports of paresthesia following local anesthetic administration , J Can Dent Assoc 61:319 – 320 , 323 – 326, 329 – 330 , 1995 .
24. Hillerup S, Jensen R. Nerve injury caused by mandibular block analgesia. Int J Oral Maxillofac Surg. 35:437-443, 2006
25. Garisto GA; Gaffen AS; Lawrence HP; Tenenbaum HC; Haas DA. Occurrence of paresthesia after dental local anesthetic administration in the United States. J Am Dent Assoc. 141(7):836-844, 2010
26. Kingon A; Sambrook P; Goss A. Higher concentration local anaesthetics causing prolonged anaesthesia. Do they? A literature review and case reports Aust Dent J. 56(4):348-351, 2011
27. Practice alert: Paraesthesia following local anaesthetic injection. Dispatch. Royal College of Dental Surgeons of Ontario. 19(3) 26, 2005
28. Oral and Dental Expert Group. Therapeutic guidelines: oral and dental 2012, Version 2, Australian Dental Association, Melbourne, page 116
29. Stedman’s Online Medical Dictionary. Paresthesia (definition). Available at: www.stedmans.com. Accessed 16 September 2015
30. Haas DA. Articaine and paresthesia: epidemiological studies. J Am Coll Dent 73(3):5 – 10, 2006
31. Pogrel MA , Thamby S : Permanent nerve involvement resulting from inferior alveolar nerve blocks , J Am Dent Assoc 131:901–907, 2000
32. Pogrel MA , Thamby S : The etiology of altered sensation in the inferior alveolar, lingual, and mental nerves as a result of dental treatment , J Calif Dent Assoc 27:531–538, 1999 .
33. Pogrel MA , Thamby S : The etiology of altered sensation in the inferior alveolar, lingual, and mental nerves as a result of dental treatment , J Calif Dent Assoc 27:531–538, 1999
34.Dower JS Jr : A review of paresthesia in association with administration of local anesthesia, Dent Today 22:64–69, 2003
35. Berde CB, Strichartz GR. Local Anesthetics, in Miller’s Anesthesia, Miller RD editor. 8th ed. 2015. Saunders Elsevier, pages 1028-1054
36. Pogrel MA. Permanent nerve damage from inferior alveolar nerve blocks – an update to include articaine. J Calif Dent Assoc 36(4):271-273, 2007
37. Pogrel MA. Permanent nerve damage from inferior alveolar nerve blocks: a current update. J Calif Dent Assoc 40(10):795-797, 2012
38. McDowell AJ. Effective practical steps to avoid complications in face-lifting. Review of 105 consecutive cases. Plast Reconstr Surg. 50(6):563-572, 1972
39. Lagarde P. Paresthesies du territoire mentonnier, secondaires a un traitement endodontique. [Paresthesia in the area of the chin, secondary to endodontic treatment]. Inf Dent. 60(19):17-23, 1978
40. Hickel R, Spitzer WJ, Petschelt A, Voss A. Zur Problematik von Sensibilitatsstorungen nach Leitungsanasthesie im Unterkiefer. [Sensitivity problems following mandibular conduction anesthesia]. Dtsch Zahnarztl Z. 43(11):1159-1161, 1988
41. Nickel AA Jr. A retrospective study of paresthesia of the dental alveolar nerves. Anesth Prog. 37(1):42-45, 1990
42. Stenver DI, Case number: 3200-1367, Adverse effects from anaesthetics used in relation with dental care with a special focus on anaesthetics containing articaine. Pharmacovigilance Working Party of the European Union. 20 October, 2006
43. Danish Medicines Agency (Laegemiddel Styrelsen), Report 25 October 2011
44. Garisto GA, Gaffen AS, Lawrence HP, Tenenbaum HC, Haas DA. Occurrence of paresthesia aftert dental local anesthetic administration in the United States. J Am Dent Assoc 141(7):836-844, 2010
45. U.S. Food and Drug Administration Center for Drug Evaluation and Research, Office of Post-Marketing Drug Risk Assessment. Revised 9 January 2009. http://www.fda.gov/Drugs/GuidanceComplianceRegulatoryInformation/Surveillance/AdverseDrugEffects/default.htm
46. Weber JCP. Epidemiology of adverse reactions to nonsteroidal antiinflammatory drugs. In Rainsford KD, Velo GP eds. Advances in Inflammation Research. Vol. 6. New York, Raven Press, 1984, pages 1-7
47. Hartnell NR; Wilson JP. Replication of the Weber effect using postmarketing adverse event reports voluntarily submitted to the United States Food and Drug Administration. Pharmacotherapy. 24(6):743-749, 2004
48. Alling CC 3rd. Dysesthesia of the lingual and inferior alveolar nerves following third molar surgery. J Oral Maxillofac Surg. 44(6):454-457, 1986
49. Ellies LG. Altered sensation following mandibular implant surgery: a retrospective study. J Prosthet Dent. 68(4):664-71, 1992
50. Medline search. Years 1946-2015 key words: paresthesia, dentistry. Search 16 September 2015
51. Snoeck M. Articaine: a review of its use for local and regional anesthesia. Local Regional Anesth 5:23-33, 2012
52. Pogrel MA, Thamby S. Permanent nerve involvement resulting from inferior alveolar nerve blocks. J Am Dent Assoc 131:901-907, 2000
53. Pogrel MA; Schmidt BL; Sambajon V; Jordan RC. Lingual nerve damage due to inferior alveolar nerve blocks: a possible explanation. J Am Dent Assoc. 134(2):195-199, 2003
54. Katyal V. The efficacy and safety of articaine versus lignocaine in dental treatments: a meta-analysis. J Dent. 38(4):307-317, 2010
55. Brandt RG; Anderson PF; McDonald NJ; Sohn W; Peters MC. The pulpal anesthetic efficacy of articaine versus lidocaine in dentistry: a meta-analysis. J Am Dent Assoc. 142(5):493-504, 2011
56. Baroni DB; Franz-Montan M; Cogo K; Berto LA; Volpato MC; Novaes PD; Groppo FC. Effect of articaine on mental nerve anterior portion: histological analysis in rats. Acta Odontol Scand. 71(1):82-87, 2013
57. Malet A; Faure MO; Deletage N; Pereira B; Haas J; Lambert G. The comparative cytotoxic effects of different local anesthetics on a human neuroblastoma cell line. Anesth Analg. 120(3):589-596, 2015











